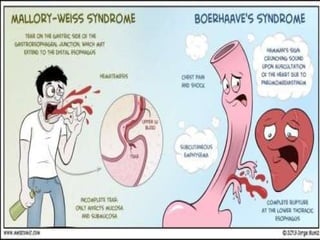
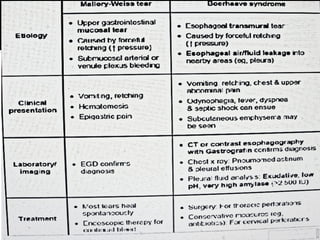
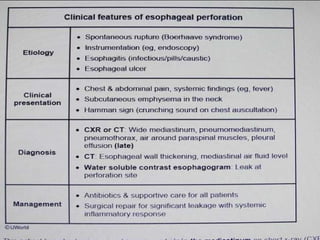
The document outlines various esophageal disorders, including their causes, symptoms, diagnosis, and management. Key conditions discussed include esophageal perforation, achalasia, Barrett's esophagus, and Mallory-Weiss syndrome, detailing specific complications and treatment strategies such as surgical interventions, endoscopy, and medical management. It highlights the importance of diagnosis through endoscopic examination and contrast studies to guide appropriate therapeutic approaches.























![Esophageal_Diseases_ENT_BY_NH[1].ppppptx](https://cdn.slidesharecdn.com/ss_thumbnails/esophagealdiseasesentbynh1-251115082945-26df9b86-thumbnail.jpg?width=640&height=640&fit=bounds)















































