- Background Paper 13 -
A national partnership for acA national partnership for acA national partnership for acA national partnership for action to tion to tion to tion to
end health dend health dend health dend health disparities in the United Statesisparities in the United Statesisparities in the United Statesisparities in the United States
Mirtha R. Beadle 1
Garth N. Graham 1
Paul E. Jarris 2
Carlessia A. Hussein 3
Alan Morgan 4
Ron Finch 5
1 Office of Minority Health, U.S. Department of Health and Human Services
2 Association of State and Territorial Health Officials; USA
3 National Association of State Offices of Minority Health; USA
4 National Rural Health Association; USA
5 National Business Group on Health; USA
- Draft Background Paper 13 -
Disclaimer
WCSDH/BCKGRT/13/2011
This draft background paper is one of several in a series commissioned by the World Health Organization for the
World Conference on Social Determinants of Health, held 19-21 October 2011, in Rio de Janeiro, Brazil. The goal
of these papers is to highlight country experiences on implementing action on social determinants of health.
Copyright on these papers remains with the authors and/or the Regional Office of the World Health Organization
from which they have been sourced. All rights reserved. The findings, interpretations and conclusions expressed in
this paper are entirely those of the author(s) and should not be attributed in any manner whatsoever to the World
Health Organization.
All papers are available at the symposium website at www.who.int/sdhconference. Correspondence for the authors
can be sent by email to [email protected]
The designations employed and the presentation of the material in this publication do not imply the expression of
any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines
on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific
companies or of certain manufacturers' products does not imply that they are endorsed or recommended by the
World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions
excepted, the names of proprietary products are distinguished by initial capital letters. The published material is
being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation
and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages ...
You should respond to at least two of your peers by extending- refutin.docxjosee57
You should respond to at least two of your peers by extending, refuting/correcting, or adding additional nuance to their posts.
Post #1
Jenna Horgan
NUR 420
Professor Roberts
January 12, 2023
Who are the clients in Community Health nursing?
Individuals, families, and groups who live in a specific geographic area and may be at risk for health problems or in need of health services are considered clients in community health nursing. People of all ages, from infants to the elderly, as well as those with physical, mental, or social challenges, may be included. The purpose of community health nursing is to promote the health and well-being of the entire community by addressing the health needs of its individual members (Rector & Stanley, 2021). Community health nurses work with clients to identify and address health risks, provide health and wellness education, and connect clients to suitable health services.
What government resources might they be eligible for?
Individuals and families may be eligible for a variety of government resources depending on their circumstances. Some of these resources are intended specifically for people with low incomes or who are experiencing financial hardship, while others are open to anyone who meets certain criteria. Among the resources available to them are (ISPOR, n.d):
1. Medicaid: It is a federal-state partnership program that provides health insurance to low-income individuals and families. Individuals must meet income and asset limits, as well as other requirements, to be eligible.
2. Children's Health Insurance Program (CHIP): It is a federally funded program that provides health insurance to low-income children that are not eligible for Medicaid but cannot afford private health insurance. It provides coverage for a variety of medical services, such as preventive care, doctor visits, hospital stays, and prescription medications. Eligibility is determined by income and family size.
3. Supplemental Nutrition Assistance Program (SNAP): It is also known as food stamps and it provides financial assistance to low-income individuals and families in order for them to purchase food. Income and assets, as well as other factors, determine SNAP eligibility.
4. Temporary Assistance for Needy Families (TANF): This program helps low-income families with children by providing financial assistance as well as other services such as job training and childcare. Income and assets, as well as other factors, determine TANF eligibility.
5. Low Income Home Energy Assistance Program (LIHEAP): It is program funded by the federal government that provides low-income households with financial assistance to help them pay for home energy costs such as heating and cooling. The Department of Health and Human Services (HHS) administers the program, which is intended to assist households that are struggling to pay their energy bills and may face having their service disconnected. Eligibility is determined by income and family size.
What ag.
Disparities in Health Care: The Significance of Socioeconomic StatusAmanda Romano-Kwan
This research paper discusses the disparities in the health care system, with a specific focus on socioeconomic status and how it affects the access and availability of quality care.
1
Literature Review Assignment
STUDENT NAME
Class
Date
2
Part A: Annotated Bibliography
Article 1: Immigration as a Social Determinant of Health
Castañeda, H., Holmes, S. M., Madrigal, D. S., Young, M.-E. D., Beyeler, N., & Quesada, J.
(2015). Immigration as a Social Determinant of Health. Annual Review of Public
Health, 36(1), 375–392. doi: 10.1146/annurev-publhealth-032013-182419
Abstract
Although immigration and immigrant populations have become increasingly important foci in
public health research and practice, a social determinants of health approach has seldom been
applied in this area. Global patterns of morbidity and mortality follow inequities rooted in
societal, political, and economic conditions produced and reproduced by social structures,
policies, and institutions. The lack of dialogue between these two profoundly related
phenomena—social determinants of health and immigration—has resulted in missed
opportunities for public health research, practice, and policy work. In this article, we discuss
primary frameworks used in recent public health literature on the health of immigrant
populations, note gaps in this literature, and argue for a broader examination of immigration as
both socially determined and a social determinant of health. We discuss priorities for future
research and policy to understand more fully and respond appropriately to the health of the
populations affected by this global phenomenon.
Annotated Bibliography
The article reports on the importance of identifying social determinants and the effects of
socially determined structures among immigrant populations in the United States. The study
identifies ways in which immigrants health outcomes are based on biases due to using
3
information based on group behaviors instead of on an induvial case. The impact of migrant and
immigrant individuals, physical and mental health in these communities’ changes as social,
economic, and political policies take place. This article is helpful in that broadens the
immigration experience including more central factors than just language, income, or education
as the cause of all health related problems in this community. But to show factors of power
structures and the ability to put in place effective health interventions that respond to direct
causes of poor or declining health in these populations.
Article 2: Fear by Association: Perceptions of Anti-Immigrant Policy and Health Outcomes
Vargas, Edward & Sanchez, Gabriel & Juárez, Melina. (2017). Fear by Association: Perceptions
of Anti-Immigrant Policy and Health Outcomes. Journal of Health Politics, Policy and
Law. 42. 3802940. 10.1215/03616878-3802940.
Abstract
The United States is experiencing a renewed period of immigration and immigrant policy
activity as well as heightened enforcement of such policies. This intensified activity can affect
various aspects of im ...
You should respond to at least two of your peers by extending- refutin.docxjosee57
You should respond to at least two of your peers by extending, refuting/correcting, or adding additional nuance to their posts.
Post #1
Jenna Horgan
NUR 420
Professor Roberts
January 12, 2023
Who are the clients in Community Health nursing?
Individuals, families, and groups who live in a specific geographic area and may be at risk for health problems or in need of health services are considered clients in community health nursing. People of all ages, from infants to the elderly, as well as those with physical, mental, or social challenges, may be included. The purpose of community health nursing is to promote the health and well-being of the entire community by addressing the health needs of its individual members (Rector & Stanley, 2021). Community health nurses work with clients to identify and address health risks, provide health and wellness education, and connect clients to suitable health services.
What government resources might they be eligible for?
Individuals and families may be eligible for a variety of government resources depending on their circumstances. Some of these resources are intended specifically for people with low incomes or who are experiencing financial hardship, while others are open to anyone who meets certain criteria. Among the resources available to them are (ISPOR, n.d):
1. Medicaid: It is a federal-state partnership program that provides health insurance to low-income individuals and families. Individuals must meet income and asset limits, as well as other requirements, to be eligible.
2. Children's Health Insurance Program (CHIP): It is a federally funded program that provides health insurance to low-income children that are not eligible for Medicaid but cannot afford private health insurance. It provides coverage for a variety of medical services, such as preventive care, doctor visits, hospital stays, and prescription medications. Eligibility is determined by income and family size.
3. Supplemental Nutrition Assistance Program (SNAP): It is also known as food stamps and it provides financial assistance to low-income individuals and families in order for them to purchase food. Income and assets, as well as other factors, determine SNAP eligibility.
4. Temporary Assistance for Needy Families (TANF): This program helps low-income families with children by providing financial assistance as well as other services such as job training and childcare. Income and assets, as well as other factors, determine TANF eligibility.
5. Low Income Home Energy Assistance Program (LIHEAP): It is program funded by the federal government that provides low-income households with financial assistance to help them pay for home energy costs such as heating and cooling. The Department of Health and Human Services (HHS) administers the program, which is intended to assist households that are struggling to pay their energy bills and may face having their service disconnected. Eligibility is determined by income and family size.
What ag.
Disparities in Health Care: The Significance of Socioeconomic StatusAmanda Romano-Kwan
This research paper discusses the disparities in the health care system, with a specific focus on socioeconomic status and how it affects the access and availability of quality care.
1
Literature Review Assignment
STUDENT NAME
Class
Date
2
Part A: Annotated Bibliography
Article 1: Immigration as a Social Determinant of Health
Castañeda, H., Holmes, S. M., Madrigal, D. S., Young, M.-E. D., Beyeler, N., & Quesada, J.
(2015). Immigration as a Social Determinant of Health. Annual Review of Public
Health, 36(1), 375–392. doi: 10.1146/annurev-publhealth-032013-182419
Abstract
Although immigration and immigrant populations have become increasingly important foci in
public health research and practice, a social determinants of health approach has seldom been
applied in this area. Global patterns of morbidity and mortality follow inequities rooted in
societal, political, and economic conditions produced and reproduced by social structures,
policies, and institutions. The lack of dialogue between these two profoundly related
phenomena—social determinants of health and immigration—has resulted in missed
opportunities for public health research, practice, and policy work. In this article, we discuss
primary frameworks used in recent public health literature on the health of immigrant
populations, note gaps in this literature, and argue for a broader examination of immigration as
both socially determined and a social determinant of health. We discuss priorities for future
research and policy to understand more fully and respond appropriately to the health of the
populations affected by this global phenomenon.
Annotated Bibliography
The article reports on the importance of identifying social determinants and the effects of
socially determined structures among immigrant populations in the United States. The study
identifies ways in which immigrants health outcomes are based on biases due to using
3
information based on group behaviors instead of on an induvial case. The impact of migrant and
immigrant individuals, physical and mental health in these communities’ changes as social,
economic, and political policies take place. This article is helpful in that broadens the
immigration experience including more central factors than just language, income, or education
as the cause of all health related problems in this community. But to show factors of power
structures and the ability to put in place effective health interventions that respond to direct
causes of poor or declining health in these populations.
Article 2: Fear by Association: Perceptions of Anti-Immigrant Policy and Health Outcomes
Vargas, Edward & Sanchez, Gabriel & Juárez, Melina. (2017). Fear by Association: Perceptions
of Anti-Immigrant Policy and Health Outcomes. Journal of Health Politics, Policy and
Law. 42. 3802940. 10.1215/03616878-3802940.
Abstract
The United States is experiencing a renewed period of immigration and immigrant policy
activity as well as heightened enforcement of such policies. This intensified activity can affect
various aspects of im ...
Working Together for HealthEfforts to improve public health occ.docxmayank272369
Working Together for Health
Efforts to improve public health occur around the world every day. However, simply attempting to fix a problem without acknowledging, and respecting, the relationship between culture and health is not likely to have long-term success. Successful interventions, such as those in the case studies presented in your resources, demonstrate organizational collaboration. They also highlight the value of cultural relativism to improve population health outcomes. Working for the people (and with the people) can make an important impact on health.
To prepare for this Discussion, review Chapter 2, "Communities Working to Achieve Health Equity," in the Promoting Health Equity document from Week 2. Select one case study to profile in your discussion. How do the key concepts, addressed in this week's Learning Resources, relate to the case study you selected?
1. Briefly describe the population and health issue addressed in the case study.
2. In what way did cultural beliefs and behaviors contribute to the health issue in these case studies?
3. Which public health (or other) groups intervened, and how did they cooperate to improve health for this population?
4. What measures did the organization take to ensure they respected the dignity of the individuals and their culture?
5. How does this case study relate to our class resources addressing culture and collaboration?
Public and Global Health Essentials
· Chapter 11, "Working together to improve global health"
Around the world professionals from numerous organizations rely on others to achieve their public health goals. This chapter stresses global cooperation, partnerships and collaborations vital to addressing health issues
Top of Form
For this discussion, I will access the overall health and identify key issues in Garland County, Arkansas. According to County Health Rankings of 2017, in the area of health outcomes Garland County, Arkansas ranked 44 out of 75 counties. When reviewing national and state results, Arkansas exceeded the U.S. median in all categories of health outcomes. For the health factors summary, they ranked much lower coming in at 28. In the category of health behaviors, 25% of adult Arkansans are smokers and 34% are obese. Both of these percentages are above national averages. Referring back to the topic of my previous discussion, the number of diagnosed sexually transmitted diseases was almost twice as many as the national average and the teen birth rate almost doubled the national average. In the category of clinical care Arkansas is near equal or slightly lower than national averages. Social and economic factors also rank fairly close to the national averages. Overall physical environment factors are no different than the national averages. In my opinion, Arkansas is a fairly clean and comfortable place to live.
After considering these statistics, I can answer the opening question of this discussion. "How healthy is your community?" Not very! As a health ...
Concept and definitions
Health education
Beliefs and approaches in health promotion
Health promotion strategies and priority actions
Public health, social movement, health inequity and millennium goals
Canadian experience in health promotion
Conclusion
Respond to at least two classmates who identified different areas of.docxpeggyd2
Respond to at least two classmates who identified different areas of disparity than your own. Do you agree or disagree with their assessment of the impact of economic policy on the disparity? Does the disparity discussed have a microeconomic or a macroeconomic impact on health care?
Post # 1
Trina Cox
Disparity in healthcare can be defined as, “differences between groups in health insurance coverage, access to and use of care, and quality of care” (Orger & Artiga, 2018). There are various healthcare disparities; however, the key areas of disparity I have chosen to identify and analyze include health insurance coverage, quality of care, and gender. As most people already know, health insurance is a type of insurance coverage that is designed to cover an insured person’s medical expenses (such as hospital, doctor, laboratory and pharmacy services). Although the number of uninsured Americans have decreased drastically since the passing of ACA, disparities in this area still exist. Some individuals’ annual incomes still are not enough to pay the low premiums that may be required of them to have access to health insurance coverage.
Quality of care can be described as, “the degree to which health care services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge” (AHRQ, 2017). Although it is an unethical act displayed by healthcare professionals; in some areas, all patients are not treated equally with regards to quality of care. According to Dr. Ananya Mandal (2019), discrimination occurs when healthcare providers treat individuals from certain population groups differently to other population groups, whether this is done consciously or not. It is common for this to occur when providers have stereotyped impressions of specific racial or ethnic groups.
Gender can play a major role in healthcare disparities among women, specifically, in some of the developed countries. Researchers have reported that determinants of gender differences, like welfare indicators (e.g., education and income), behavioral factors (e.g., smoking and drinking), and social factors (e.g., social support and socioeconomic status) have direct correlations with some of the existing disparities (Hassanzadeh, et al, 2017). Afghanistan is a country that still has a high rate of gender disparities among women, even though some improvements have occurred. In this country, the biggest disparities that I feel still exist are between women in rural versus urban areas, and those with some education, as opposed to those women with none; showing that as education of women increases, so does their health and that of their children because of the education and resources that they have.
I think several economic policies have impacted these disparities and they include differences in income levels, education, and geographic location. A person’s annual income may have a direct effect on his or her ability.
Velasco-Mondragon et al. Public Health Reviews (2016) 3731 .docxjessiehampson
Velasco-Mondragon et al. Public Health Reviews (2016) 37:31
DOI 10.1186/s40985-016-0043-2
REVIEW Open Access
Hispanic health in the USA: a scoping
review of the literature
Eduardo Velasco-Mondragon1* , Angela Jimenez2, Anna G. Palladino-Davis3, Dawn Davis4
and Jose A. Escamilla-Cejudo5
* Correspondence:
[email protected]
1College of Osteopathic Medicine,
Touro University California, 1310
Johnson Lane; H-82, Rm. 213,
Vallejo, CA 94592, USA
Full list of author information is
available at the end of the article
Abstract
Hispanics are the largest minority group in the USA. They contribute to the economy,
cultural diversity, and health of the nation. Assessing their health status and health needs
is key to inform health policy formulation and program implementation. To this end, we
conducted a scoping review of the literature and national statistics on Hispanic health in
the USA using a modified social-ecological framework that includes social determinants
of health, health disparities, risk factors, and health services, as they shape the leading
causes of morbidity and mortality. These social, environmental, and biological forces have
modified the epidemiologic profile of Hispanics in the USA, with cancer being the
leading cause of mortality, followed by cardiovascular diseases and unintentional injuries.
Implementation of the Affordable Care Act has resulted in improved access to health
services for Hispanics, but challenges remain due to limited cultural sensitivity, health
literacy, and a shortage of Hispanic health care providers. Acculturation barriers and
underinsured or uninsured status remain as major obstacles to health care access.
Advantageous health outcomes from the “Hispanic Mortality Paradox” and the “Latina
Birth Outcomes Paradox” persist, but health gains may be offset in the future by
increasing rates of obesity and diabetes. Recommendations focus on the adoption of the
Health in All Policies framework, expanding access to health care, developing cultural
sensitivity in the health care workforce, and generating and disseminating research
findings on Hispanic health.
Keywords: Hispanics, Latinos, Scoping study, Social determinants of health, Health care
inequalities, Health care access
Background
Hispanics are the largest ethnic minority in the USA; in 2014, Hispanics comprised
17.4% of the US population (55.4 million), and this percentage is expected to increase
to 28.6% (119 million) by 2060. Hispanics in the USA include native-born and foreign-
born individuals immigrating from Latin America, the Caribbean, and Spain [1].
Hispanics are disproportionately affected by poor conditions of daily life, shaped by struc-
tural and social position factors (such as macroeconomics, cultural values, income, educa-
tion, occupation, and social support systems, including health services), known as social
determinants of health (SDH). SDH exert health effects on individuals through allostatic
load [2], a phenomenon purported t ...
Public health is defined as “the approach to medicine that is concerned with the health of the community as a whole” ("Definition of Public Health", 2013). Without public health, health care would be in vain. A person could be in perfect health one day, come in contact with a person with a contagious disease, and be dead within twenty-four hours. This paper will discuss the local health department.
CHAPTER 1History of the U.S. Healthcare SystemLEARNING OBJECTI.docxmccormicknadine86
CHAPTER 1
History of the U.S. Healthcare System
LEARNING OBJECTIVES
The student will be able to:
■ Describe five milestones of medicine and medical education and their importance to health care.
■ Discuss five milestones of the hospital system and their importance to health care.
■ Identify five milestones of public health and their importance to health care.
■ Describe five milestones of health insurance and their importance to health care.
■ Explain the difference between primary, secondary, and tertiary prevention.
■ Explain the concept of the iron triangle as it applies to health care.
DID YOU KNOW THAT?
■ When the practice of medicine first began, tradesmen such as barbers practiced medicine. They often used the same razor to cut hair as to perform surgery.
■ In 2014, the United States spent 17.5% of the gross domestic product on healthcare spending, which is the highest in the world.
■ As a result of the Affordable Care Act, the number of uninsured is projected to decline to 23 million by 2023.
■ The Centers for Medicare and Medicaid Services predicts national health expenditures will account for over 19% of the U.S. gross domestic product.
■ The United States is the only major country that does not have universal healthcare coverage.
■ In 2002, the Joint Commission issued hospital standards requiring them to inform their patients if their results were not consistent with typical care results.
▶ Introduction
It is important as a healthcare consumer to understand the history of the U.S. healthcare delivery system, how it operates today, who participates in the system, what legal and ethical issues arise as a result of the system, and what problems continue to plague the healthcare system. We are all consumers of health care. Yet, in many instances, we are ignorant of what we are actually purchasing. If we were going to spend $1,000 on an appliance or a flat-screen television, many of us would research the product to determine if what we are purchasing is the best product for us. This same concept should be applied to purchasing healthcare services.
Increasing healthcare consumer awareness will protect you in both the personal and professional aspects of your life. You may decide to pursue a career in health care either as a provider or as an administrator. You may also decide to manage a business where you will have the responsibility of providing health care to your employees. And last, from a personal standpoint, you should have the knowledge from a consumer point of view so you can make informed decisions about what matters most—your health. The federal government agrees with this philosophy.
As the U.S. population’s life expectancy continues to lengthen—increasing the “graying” of the population—the United States will be confronted with more chronic health issues because, as we age, more chronic health conditions develop. The U.S. healthcare system is one of the most expensive systems in the world. According to 2014 statistics, the ...
55-J-10-2Having reviewed my initial forum post, with minimal c.docxfredharris32
55-J-10-2
Having reviewed my initial forum post, with minimal changes, I uphold my views that health equality and health disparities represent one of the most significant challenges facing the health of the global population given its correlation with good health and well-being (goal 3). With that said, I feel it's important to back away from using the terms health equality and health disparities using instead the term health equity. Notably, this change results from research conducted during module seven in which I happened upon the following quote.
Equity is the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically. Health inequities, therefore, involve more than inequality with respect to health determinants, access to the resources needed to improve and maintain health or health outcomes. They also entail a failure to avoid or overcome inequalities that infringe on fairness and human rights norms. (World Health Organization, 2018, para. 1)
Thus, health inequities and health disparities become interchangeable as forms of unjust health differences, which unfavorably affect groups of people.
As such, "equity is the process and equality is the outcome" ("Equity", 2016, para. 2). In other words, "the route to achieving equity will not be accomplished through treating everyone equally. It will be achieved by treating everyone equitably, or justly according to their circumstances" (Dressel, 2014, para, 2). Notably, sustainable development goals one (poverty) and two (hunger) are linked to good health and well-being (goal 3), which in turn correlates with equity (United Nations, 2015). Thus, it's my view that by addressing equity on a global scale, you begin to break down the exasperating challenges associated with poverty, hunger, and good health and well-being.
With that said, the knowledge obtained throughout this course will prove beneficial as I further carve my career pathway in the areas of both public health and community health education as it relates to HIV/AIDS. The latter has been an area of extreme interest since the beginning of the epidemic back in the early 80s, yet that interest intensified ten-fold when, after 25 years of safely navigating the gay culture, I was diagnosed with HIV at the age of 41. Now ten years later, I stand in amazement that the vulnerabilities that led to my diagnosis persist; thus, continue to place the sexual health of today's youth at an increased risk. Subsequently, having completed this course, I feel more prepared to address the increased incidences of HIV within Phoenix's LGBT community.
In closing, I feel confident in suggesting that each chapter of the course textbook has content that's applicable to my field of work at the community level. Notable chapters that helped develop skills include chapters two (Culture, Behavior, and Health), four (Reproductive Health), five (Infectiou.
Forty years ago, the Region of the Americas played a critical JeanmarieColbert3
Forty years ago, the Region of the Americas played a critical role in the develop-
ment and negotiation of the Alma-Ata Declaration, which identified primary health
care as a central strategy to the goal of health for all and a comprehensive approach to
the organization of health systems. Since then, the values and principles of primary
health care, which include the right to health, equity, solidarity, social justice and par-
ticipation, and multisectoral action, among others, have formed the basis of many
PAHO mandates and have guided health systems transformation in the Region. The
positive impact of primary health care on the reduction of mortality, morbidity, and
inequities in health is well known. (1) What’s more, primary health care consumes less
financial resources than curative approaches and promotes a chain of positive results
from improved health to increased economic output, growth and productivity. (2)
In 2007, PAHO’s position paper on Renewing Primary Health Care in the Americas
included the definition of elements and functions of a primary healthcare-based
health system with the intention of providing guidance to countries as they worked
to transform their systems. (3) In 2014, the 53rd PAHO Directing Council’s resolution
on Universal Access to Health and Universal Health Coverage (4) recognized the
values and principles of Alma-Ata. The resolution urged PAHO Member States to
promote intersectoral action to address social determinants of health and move
toward health systems where all people and communities have access, without any
discrimination, to comprehensive, appropriate and timely, quality health services, as
well as access to safe, effective, and affordable quality medicines, while ensuring that
the use of such services does not expose users to financial difficulties. (4) The Sustai-
nable Health Agenda for the Americas 2018–2030, which represents the commitment
of Member States to the 2030 Agenda for Sustainable Development and unfinished
business from previous engagements, established areas of action that reinforce and
complement the recommendations of the Alma-Ata Declaration. These include stren-
gthening the national health authority; tackling health determinants; increasing so-
cial protection and access to quality health services; diminishing health inequalities
among countries and inequities within them; reducing the risk and burden of disease;
strengthening the management and development of health workers; harnessing
knowledge, science, and technology; and strengthening health security. (5)
In the Region, the lessons that have been learned about the primary health care
approach since Alma-Ata have been overwhelmingly positive. We have seen that
countries that have implemented policies and programs based on primary health
care have registered the lowest levels of infant and maternal mortality. Other achie-
vements include improvement in public spending, increase in primary care s ...
Source: CDC Behavioral Risk Factor Surveillance System.
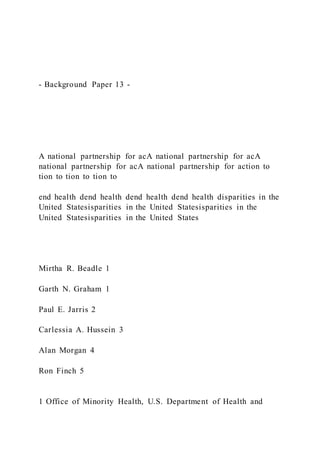
State-specific Prevalence of Obesity Among U.S. Adults, by Race/Ethnicity, 2006-2008
Definitions:Obesity: Body mass index (BMI) of 30 or higher.
Body mass index (BMI): A measure of an adult’s weight in relation to his or her height, specifically the adult’s weight in kilograms divided by the square of his or her height in meters.
Source: CDC Behavioral Risk Factor Surveillance System.
State-specific Prevalence of Obesity Among U.S. Adults, by Race/Ethnicity, 2006-2008
Methods:Behavioral Risk Factor Surveillance System (BRFSS). Self-reported weights and heights.Limited to three years of data and limited to three racial/ethnic populations; non-Hispanic whites, non-Hispanic blacks, and Hispanics.Age-adjusted to the 2000 U.S. standard population.
Source: CDC Behavioral Risk Factor Surveillance System.
(*BMI 30)
Hispanic
State-specific Prevalence of Obesity* Among U.S. Adults, by Race/Ethnicity, 2006-2008
White non-Hispanic
Black non-Hispanic
Source: CDC Behavioral Risk Factor Surveillance System.
(*BMI 30)
White non-Hispanic
State-specific Prevalence of Obesity* Among U.S. Adults, by Race/Ethnicity, 2006-2008
Source: CDC Behavioral Risk Factor Surveillance System.
(*BMI 30)
State-specific Prevalence of Obesity* Among U.S. Adults, by Race/Ethnicity, 2006-2008
Black non-Hispanic
Source: CDC Behavioral Risk Factor Surveillance System.
(*BMI 30)
Hispanic
State-specific Prevalence of Obesity* Among U.S. Adults, by Race/Ethnicity, 2006-2008
Source: CDC Behavioral Risk Factor Surveillance System.
Table. Prevalence of obesity, by region and race/ethnicity, 2006-2008Non-Hispanic whiteNon-Hispanic blackHispanicTotal Both sexes23.735.728.7 Men25.431.627.8 Women21.839.229.4Northeast Both sexes22.631.726.6 Men25.026.526.9 Women20.036.126.0Midwest Both sexes25.436.329.6 Men27.032.129.7 Women23.840.129.2South Both sexes24.436.929.2 Men26.332.628.3 Women22.540.629.7West Both sexes21.033.129.0 Men22.134.127.3 Women19.832.030.4
Source: CDC Behavioral Risk Factor Surveillance System.
SummaryNon-Hispanic blacks had the highest prevalence, followed by Hispanics, and non-Hispanic whites For non-Hispanic blacks
Overall prevalence of obesity—35.7%
Higher prevalences were found in the Midwest and South
Prevalence ranged from 23.0% (New Hampshire) to 45.1% (Maine)
40 states had a prevalence of ≥ 30%
5 states (Alabama, Maine, Mississippi, Ohio, and Oregon) had a prevalence of ≥ 40%
*
Compared to non-Hispanic whites, non-Hispanic blacks had about 50% higher prevalence of obesity, and Hispanics had about 20% higher prevalence
Source: CDC Behavioral Risk Factor Surveillance System.
Summary (Cont’d) For Hispanics
Overall prevalence of obesity—28.7%
Lower prevalence was observed in the Northeast
Prevalence ranged from 21.0% (Maryland) to 36.7% (Tennessee)
11 states had a prevalence of ≥ 30%For non-Hispanic whites
Ove.
1 Evidence-Based Practices to Guide ClinicaSilvaGraf83
1
Evidence-Based Practices to Guide Clinical Practices
Marilaura Mieres
Miami Regional University
Dr.Mercedes
03/28/2021
Evidence-Based Practices to Guide Clinical Practices
2
Introduction
Evidence best practices is an approach that translates excellent scientific research
evidence to enhanced practical decisions aiming at improving health. EBP involves using
research findings obtained from systematic data collection that is achieved through observations
and analyzed experiments. The connection of research, theory, and EBP are interlinked in that
the delivery of one results in another aspect's discovery. Through research findings, a theory is
discovered, and through various experiments and observations, evidence-based practices are
identified.
Interrelationship Between the Theory, Research, and EBP.
According to Cannon & Boswell (2016), health professionals require standards to analyze
behavioral treatments in the behavioral sciences. Through complete incorporation and
implementation processes, health professionals must value EBP processes, health theories, and
research. Through experience, health practitioners must learn to integrate research results to
determine the best treatment plans suitable for patients. Through this research results,
experiments, and evidence, health practitioners with academicians ally to discover a theory. The
treatments are offered according to patients' values, interests, and preferences (Cannon &
Boswell 2016). The values increase practitioners' skills and knowledge to analyze research
outcomes effectively. Nurses are expected to think critically after being taught and encouraged,
which corresponds with evidence-based practices. Nurses' critical thinking skills require a
foundation on which proven research and tested data can be based. The proven research,
evidence-based practices, and a good foundation all connect to form a theory that research can
rely on and nurses can use to prove their practices.
3
Additionally, health professionals at all levels must identify challenges and arising
questions to address patients' needs and offer quality practices to discover appropriate
interventions suitable for every challenge. Health professionals are directly involved in research
projects that allow them to understand the best methods to publish for evidence-based practices.
Through different researches and publications, health professionals like advanced practice nurses
use research to solve health dilemmas. Nurses find platforms centered on tested clarifications
through nursing practices and methodical examinations from research to build a base for
procedures and care.
Moreover, research is a scientific procedure that anticipates outcomes through the use of
fundamental expertise. Research processes enhance the capacity of discipline through clarity and
visualized aspects. The discipline's ability to put i ...
1 Green Book Film Analysis Sugiarto MuljSilvaGraf83
1
Green Book Film Analysis
Sugiarto Muljadi
CSUN
COMS 321
Prof. Darla Anderson
12th May 2021
2
Green Book Analysis
Social stratification exists in almost every place that human’s dwell. Nonetheless, race
remains one of the most controversial elements of social stratification. The film Green Book
wants the audience to learn that there are no differences between humans regardless of their
race. While watching it, I was concerned that the script might have glossed over Shirley and
other African-Americans face. The newfound abundance of clean, inexpensive cars in the
1930s was more than a matter of convenience for middle-class Americans (IMDb, 2020). It
opened up new opportunities, giving them the freedom to fly across the world at their own
pace without having to rely on anyone. Also, in a constitutionally segregated world in some
areas and functionally segregated almost everywhere else, this was so for African Americans
(Lemire, 2018). However, while white travelers could travel with relative ease, stopping at
restaurants, bars, entertainment venues, and places to stay as they wished, African Americans
faced greater challenges. Staying in the wrong hotel or attempting to eat at the wrong
restaurant could result in you being ejected or worse.
The Negro Motorist Green Book was not the only travel guide for African-Americans,
but it was the most popular. Victor Hugo Green, an African-American mail carrier from
Harlem who served in Hackensack, New Jersey, designed it. Green worked on the effort for
almost three decades, from 1936 to 1966, soon after the Civil Rights Act was signed into law,
including a four-year pause during WWII (Diamond, 2018). The Green Book quickly
established itself as the most important document for black travelers in America, outlining
where they could eat, drink, and sleep without being abused or worse. Green Book depicts
various discriminatory prejudices that permeated American life in the early and mid-
twentieth centuries, ranging from snide remarks and racial epithets to outright hatred.
3
References
Diamond, A. (2018, November 20). The true story of the 'Green book' movie. Smithsonian
Magazine. https://www.smithsonianmag.com/arts-culture/true-story-green-book-
movie-180970728/
IMDb. (2020). Green book (2018). https://www.imdb.com/title/tt6966692/plotsummary
Lemire, C. (2018). Green book movie review & film summary (2018). Movie Reviews and
Ratings by Film Critic Roger Ebert | Roger Ebert.
https://www.rogerebert.com/reviews/green-book-2018
Week # 3 Case Study: Late and Later Documentation
Case Study: Late and Later Documentation
Based on the case study, critique the documentation presented by the healthcare provider and provide examples of whether the nurse follows or did not follow documentation requisites.
State what errors you found in the documentation and if you think the nurse followed the appropriate procedure ...
More Related Content
Similar to - Background Paper 13 - A national partnership f
Working Together for HealthEfforts to improve public health occ.docxmayank272369
Working Together for Health
Efforts to improve public health occur around the world every day. However, simply attempting to fix a problem without acknowledging, and respecting, the relationship between culture and health is not likely to have long-term success. Successful interventions, such as those in the case studies presented in your resources, demonstrate organizational collaboration. They also highlight the value of cultural relativism to improve population health outcomes. Working for the people (and with the people) can make an important impact on health.
To prepare for this Discussion, review Chapter 2, "Communities Working to Achieve Health Equity," in the Promoting Health Equity document from Week 2. Select one case study to profile in your discussion. How do the key concepts, addressed in this week's Learning Resources, relate to the case study you selected?
1. Briefly describe the population and health issue addressed in the case study.
2. In what way did cultural beliefs and behaviors contribute to the health issue in these case studies?
3. Which public health (or other) groups intervened, and how did they cooperate to improve health for this population?
4. What measures did the organization take to ensure they respected the dignity of the individuals and their culture?
5. How does this case study relate to our class resources addressing culture and collaboration?
Public and Global Health Essentials
· Chapter 11, "Working together to improve global health"
Around the world professionals from numerous organizations rely on others to achieve their public health goals. This chapter stresses global cooperation, partnerships and collaborations vital to addressing health issues
Top of Form
For this discussion, I will access the overall health and identify key issues in Garland County, Arkansas. According to County Health Rankings of 2017, in the area of health outcomes Garland County, Arkansas ranked 44 out of 75 counties. When reviewing national and state results, Arkansas exceeded the U.S. median in all categories of health outcomes. For the health factors summary, they ranked much lower coming in at 28. In the category of health behaviors, 25% of adult Arkansans are smokers and 34% are obese. Both of these percentages are above national averages. Referring back to the topic of my previous discussion, the number of diagnosed sexually transmitted diseases was almost twice as many as the national average and the teen birth rate almost doubled the national average. In the category of clinical care Arkansas is near equal or slightly lower than national averages. Social and economic factors also rank fairly close to the national averages. Overall physical environment factors are no different than the national averages. In my opinion, Arkansas is a fairly clean and comfortable place to live.
After considering these statistics, I can answer the opening question of this discussion. "How healthy is your community?" Not very! As a health ...
Concept and definitions
Health education
Beliefs and approaches in health promotion
Health promotion strategies and priority actions
Public health, social movement, health inequity and millennium goals
Canadian experience in health promotion
Conclusion
Respond to at least two classmates who identified different areas of.docxpeggyd2
Respond to at least two classmates who identified different areas of disparity than your own. Do you agree or disagree with their assessment of the impact of economic policy on the disparity? Does the disparity discussed have a microeconomic or a macroeconomic impact on health care?
Post # 1
Trina Cox
Disparity in healthcare can be defined as, “differences between groups in health insurance coverage, access to and use of care, and quality of care” (Orger & Artiga, 2018). There are various healthcare disparities; however, the key areas of disparity I have chosen to identify and analyze include health insurance coverage, quality of care, and gender. As most people already know, health insurance is a type of insurance coverage that is designed to cover an insured person’s medical expenses (such as hospital, doctor, laboratory and pharmacy services). Although the number of uninsured Americans have decreased drastically since the passing of ACA, disparities in this area still exist. Some individuals’ annual incomes still are not enough to pay the low premiums that may be required of them to have access to health insurance coverage.
Quality of care can be described as, “the degree to which health care services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge” (AHRQ, 2017). Although it is an unethical act displayed by healthcare professionals; in some areas, all patients are not treated equally with regards to quality of care. According to Dr. Ananya Mandal (2019), discrimination occurs when healthcare providers treat individuals from certain population groups differently to other population groups, whether this is done consciously or not. It is common for this to occur when providers have stereotyped impressions of specific racial or ethnic groups.
Gender can play a major role in healthcare disparities among women, specifically, in some of the developed countries. Researchers have reported that determinants of gender differences, like welfare indicators (e.g., education and income), behavioral factors (e.g., smoking and drinking), and social factors (e.g., social support and socioeconomic status) have direct correlations with some of the existing disparities (Hassanzadeh, et al, 2017). Afghanistan is a country that still has a high rate of gender disparities among women, even though some improvements have occurred. In this country, the biggest disparities that I feel still exist are between women in rural versus urban areas, and those with some education, as opposed to those women with none; showing that as education of women increases, so does their health and that of their children because of the education and resources that they have.
I think several economic policies have impacted these disparities and they include differences in income levels, education, and geographic location. A person’s annual income may have a direct effect on his or her ability.
Velasco-Mondragon et al. Public Health Reviews (2016) 3731 .docxjessiehampson
Velasco-Mondragon et al. Public Health Reviews (2016) 37:31
DOI 10.1186/s40985-016-0043-2
REVIEW Open Access
Hispanic health in the USA: a scoping
review of the literature
Eduardo Velasco-Mondragon1* , Angela Jimenez2, Anna G. Palladino-Davis3, Dawn Davis4
and Jose A. Escamilla-Cejudo5
* Correspondence:
[email protected]
1College of Osteopathic Medicine,
Touro University California, 1310
Johnson Lane; H-82, Rm. 213,
Vallejo, CA 94592, USA
Full list of author information is
available at the end of the article
Abstract
Hispanics are the largest minority group in the USA. They contribute to the economy,
cultural diversity, and health of the nation. Assessing their health status and health needs
is key to inform health policy formulation and program implementation. To this end, we
conducted a scoping review of the literature and national statistics on Hispanic health in
the USA using a modified social-ecological framework that includes social determinants
of health, health disparities, risk factors, and health services, as they shape the leading
causes of morbidity and mortality. These social, environmental, and biological forces have
modified the epidemiologic profile of Hispanics in the USA, with cancer being the
leading cause of mortality, followed by cardiovascular diseases and unintentional injuries.
Implementation of the Affordable Care Act has resulted in improved access to health
services for Hispanics, but challenges remain due to limited cultural sensitivity, health
literacy, and a shortage of Hispanic health care providers. Acculturation barriers and
underinsured or uninsured status remain as major obstacles to health care access.
Advantageous health outcomes from the “Hispanic Mortality Paradox” and the “Latina
Birth Outcomes Paradox” persist, but health gains may be offset in the future by
increasing rates of obesity and diabetes. Recommendations focus on the adoption of the
Health in All Policies framework, expanding access to health care, developing cultural
sensitivity in the health care workforce, and generating and disseminating research
findings on Hispanic health.
Keywords: Hispanics, Latinos, Scoping study, Social determinants of health, Health care
inequalities, Health care access
Background
Hispanics are the largest ethnic minority in the USA; in 2014, Hispanics comprised
17.4% of the US population (55.4 million), and this percentage is expected to increase
to 28.6% (119 million) by 2060. Hispanics in the USA include native-born and foreign-
born individuals immigrating from Latin America, the Caribbean, and Spain [1].
Hispanics are disproportionately affected by poor conditions of daily life, shaped by struc-
tural and social position factors (such as macroeconomics, cultural values, income, educa-
tion, occupation, and social support systems, including health services), known as social
determinants of health (SDH). SDH exert health effects on individuals through allostatic
load [2], a phenomenon purported t ...
Public health is defined as “the approach to medicine that is concerned with the health of the community as a whole” ("Definition of Public Health", 2013). Without public health, health care would be in vain. A person could be in perfect health one day, come in contact with a person with a contagious disease, and be dead within twenty-four hours. This paper will discuss the local health department.
CHAPTER 1History of the U.S. Healthcare SystemLEARNING OBJECTI.docxmccormicknadine86
CHAPTER 1
History of the U.S. Healthcare System
LEARNING OBJECTIVES
The student will be able to:
■ Describe five milestones of medicine and medical education and their importance to health care.
■ Discuss five milestones of the hospital system and their importance to health care.
■ Identify five milestones of public health and their importance to health care.
■ Describe five milestones of health insurance and their importance to health care.
■ Explain the difference between primary, secondary, and tertiary prevention.
■ Explain the concept of the iron triangle as it applies to health care.
DID YOU KNOW THAT?
■ When the practice of medicine first began, tradesmen such as barbers practiced medicine. They often used the same razor to cut hair as to perform surgery.
■ In 2014, the United States spent 17.5% of the gross domestic product on healthcare spending, which is the highest in the world.
■ As a result of the Affordable Care Act, the number of uninsured is projected to decline to 23 million by 2023.
■ The Centers for Medicare and Medicaid Services predicts national health expenditures will account for over 19% of the U.S. gross domestic product.
■ The United States is the only major country that does not have universal healthcare coverage.
■ In 2002, the Joint Commission issued hospital standards requiring them to inform their patients if their results were not consistent with typical care results.
▶ Introduction
It is important as a healthcare consumer to understand the history of the U.S. healthcare delivery system, how it operates today, who participates in the system, what legal and ethical issues arise as a result of the system, and what problems continue to plague the healthcare system. We are all consumers of health care. Yet, in many instances, we are ignorant of what we are actually purchasing. If we were going to spend $1,000 on an appliance or a flat-screen television, many of us would research the product to determine if what we are purchasing is the best product for us. This same concept should be applied to purchasing healthcare services.
Increasing healthcare consumer awareness will protect you in both the personal and professional aspects of your life. You may decide to pursue a career in health care either as a provider or as an administrator. You may also decide to manage a business where you will have the responsibility of providing health care to your employees. And last, from a personal standpoint, you should have the knowledge from a consumer point of view so you can make informed decisions about what matters most—your health. The federal government agrees with this philosophy.
As the U.S. population’s life expectancy continues to lengthen—increasing the “graying” of the population—the United States will be confronted with more chronic health issues because, as we age, more chronic health conditions develop. The U.S. healthcare system is one of the most expensive systems in the world. According to 2014 statistics, the ...
55-J-10-2Having reviewed my initial forum post, with minimal c.docxfredharris32
55-J-10-2
Having reviewed my initial forum post, with minimal changes, I uphold my views that health equality and health disparities represent one of the most significant challenges facing the health of the global population given its correlation with good health and well-being (goal 3). With that said, I feel it's important to back away from using the terms health equality and health disparities using instead the term health equity. Notably, this change results from research conducted during module seven in which I happened upon the following quote.
Equity is the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically. Health inequities, therefore, involve more than inequality with respect to health determinants, access to the resources needed to improve and maintain health or health outcomes. They also entail a failure to avoid or overcome inequalities that infringe on fairness and human rights norms. (World Health Organization, 2018, para. 1)
Thus, health inequities and health disparities become interchangeable as forms of unjust health differences, which unfavorably affect groups of people.
As such, "equity is the process and equality is the outcome" ("Equity", 2016, para. 2). In other words, "the route to achieving equity will not be accomplished through treating everyone equally. It will be achieved by treating everyone equitably, or justly according to their circumstances" (Dressel, 2014, para, 2). Notably, sustainable development goals one (poverty) and two (hunger) are linked to good health and well-being (goal 3), which in turn correlates with equity (United Nations, 2015). Thus, it's my view that by addressing equity on a global scale, you begin to break down the exasperating challenges associated with poverty, hunger, and good health and well-being.
With that said, the knowledge obtained throughout this course will prove beneficial as I further carve my career pathway in the areas of both public health and community health education as it relates to HIV/AIDS. The latter has been an area of extreme interest since the beginning of the epidemic back in the early 80s, yet that interest intensified ten-fold when, after 25 years of safely navigating the gay culture, I was diagnosed with HIV at the age of 41. Now ten years later, I stand in amazement that the vulnerabilities that led to my diagnosis persist; thus, continue to place the sexual health of today's youth at an increased risk. Subsequently, having completed this course, I feel more prepared to address the increased incidences of HIV within Phoenix's LGBT community.
In closing, I feel confident in suggesting that each chapter of the course textbook has content that's applicable to my field of work at the community level. Notable chapters that helped develop skills include chapters two (Culture, Behavior, and Health), four (Reproductive Health), five (Infectiou.
Forty years ago, the Region of the Americas played a critical JeanmarieColbert3
Forty years ago, the Region of the Americas played a critical role in the develop-
ment and negotiation of the Alma-Ata Declaration, which identified primary health
care as a central strategy to the goal of health for all and a comprehensive approach to
the organization of health systems. Since then, the values and principles of primary
health care, which include the right to health, equity, solidarity, social justice and par-
ticipation, and multisectoral action, among others, have formed the basis of many
PAHO mandates and have guided health systems transformation in the Region. The
positive impact of primary health care on the reduction of mortality, morbidity, and
inequities in health is well known. (1) What’s more, primary health care consumes less
financial resources than curative approaches and promotes a chain of positive results
from improved health to increased economic output, growth and productivity. (2)
In 2007, PAHO’s position paper on Renewing Primary Health Care in the Americas
included the definition of elements and functions of a primary healthcare-based
health system with the intention of providing guidance to countries as they worked
to transform their systems. (3) In 2014, the 53rd PAHO Directing Council’s resolution
on Universal Access to Health and Universal Health Coverage (4) recognized the
values and principles of Alma-Ata. The resolution urged PAHO Member States to
promote intersectoral action to address social determinants of health and move
toward health systems where all people and communities have access, without any
discrimination, to comprehensive, appropriate and timely, quality health services, as
well as access to safe, effective, and affordable quality medicines, while ensuring that
the use of such services does not expose users to financial difficulties. (4) The Sustai-
nable Health Agenda for the Americas 2018–2030, which represents the commitment
of Member States to the 2030 Agenda for Sustainable Development and unfinished
business from previous engagements, established areas of action that reinforce and
complement the recommendations of the Alma-Ata Declaration. These include stren-
gthening the national health authority; tackling health determinants; increasing so-
cial protection and access to quality health services; diminishing health inequalities
among countries and inequities within them; reducing the risk and burden of disease;
strengthening the management and development of health workers; harnessing
knowledge, science, and technology; and strengthening health security. (5)
In the Region, the lessons that have been learned about the primary health care
approach since Alma-Ata have been overwhelmingly positive. We have seen that
countries that have implemented policies and programs based on primary health
care have registered the lowest levels of infant and maternal mortality. Other achie-
vements include improvement in public spending, increase in primary care s ...
Source: CDC Behavioral Risk Factor Surveillance System.
State-specific Prevalence of Obesity Among U.S. Adults, by Race/Ethnicity, 2006-2008
Definitions:Obesity: Body mass index (BMI) of 30 or higher.
Body mass index (BMI): A measure of an adult’s weight in relation to his or her height, specifically the adult’s weight in kilograms divided by the square of his or her height in meters.
Source: CDC Behavioral Risk Factor Surveillance System.
State-specific Prevalence of Obesity Among U.S. Adults, by Race/Ethnicity, 2006-2008
Methods:Behavioral Risk Factor Surveillance System (BRFSS). Self-reported weights and heights.Limited to three years of data and limited to three racial/ethnic populations; non-Hispanic whites, non-Hispanic blacks, and Hispanics.Age-adjusted to the 2000 U.S. standard population.
Source: CDC Behavioral Risk Factor Surveillance System.
(*BMI 30)
Hispanic
State-specific Prevalence of Obesity* Among U.S. Adults, by Race/Ethnicity, 2006-2008
White non-Hispanic
Black non-Hispanic
Source: CDC Behavioral Risk Factor Surveillance System.
(*BMI 30)
White non-Hispanic
State-specific Prevalence of Obesity* Among U.S. Adults, by Race/Ethnicity, 2006-2008
Source: CDC Behavioral Risk Factor Surveillance System.
(*BMI 30)
State-specific Prevalence of Obesity* Among U.S. Adults, by Race/Ethnicity, 2006-2008
Black non-Hispanic
Source: CDC Behavioral Risk Factor Surveillance System.
(*BMI 30)
Hispanic
State-specific Prevalence of Obesity* Among U.S. Adults, by Race/Ethnicity, 2006-2008
Source: CDC Behavioral Risk Factor Surveillance System.
Table. Prevalence of obesity, by region and race/ethnicity, 2006-2008Non-Hispanic whiteNon-Hispanic blackHispanicTotal Both sexes23.735.728.7 Men25.431.627.8 Women21.839.229.4Northeast Both sexes22.631.726.6 Men25.026.526.9 Women20.036.126.0Midwest Both sexes25.436.329.6 Men27.032.129.7 Women23.840.129.2South Both sexes24.436.929.2 Men26.332.628.3 Women22.540.629.7West Both sexes21.033.129.0 Men22.134.127.3 Women19.832.030.4
Source: CDC Behavioral Risk Factor Surveillance System.
SummaryNon-Hispanic blacks had the highest prevalence, followed by Hispanics, and non-Hispanic whites For non-Hispanic blacks
Overall prevalence of obesity—35.7%
Higher prevalences were found in the Midwest and South
Prevalence ranged from 23.0% (New Hampshire) to 45.1% (Maine)
40 states had a prevalence of ≥ 30%
5 states (Alabama, Maine, Mississippi, Ohio, and Oregon) had a prevalence of ≥ 40%
*
Compared to non-Hispanic whites, non-Hispanic blacks had about 50% higher prevalence of obesity, and Hispanics had about 20% higher prevalence
Source: CDC Behavioral Risk Factor Surveillance System.
Summary (Cont’d) For Hispanics
Overall prevalence of obesity—28.7%
Lower prevalence was observed in the Northeast
Prevalence ranged from 21.0% (Maryland) to 36.7% (Tennessee)
11 states had a prevalence of ≥ 30%For non-Hispanic whites
Ove.
1 Evidence-Based Practices to Guide ClinicaSilvaGraf83
1
Evidence-Based Practices to Guide Clinical Practices
Marilaura Mieres
Miami Regional University
Dr.Mercedes
03/28/2021
Evidence-Based Practices to Guide Clinical Practices
2
Introduction
Evidence best practices is an approach that translates excellent scientific research
evidence to enhanced practical decisions aiming at improving health. EBP involves using
research findings obtained from systematic data collection that is achieved through observations
and analyzed experiments. The connection of research, theory, and EBP are interlinked in that
the delivery of one results in another aspect's discovery. Through research findings, a theory is
discovered, and through various experiments and observations, evidence-based practices are
identified.
Interrelationship Between the Theory, Research, and EBP.
According to Cannon & Boswell (2016), health professionals require standards to analyze
behavioral treatments in the behavioral sciences. Through complete incorporation and
implementation processes, health professionals must value EBP processes, health theories, and
research. Through experience, health practitioners must learn to integrate research results to
determine the best treatment plans suitable for patients. Through this research results,
experiments, and evidence, health practitioners with academicians ally to discover a theory. The
treatments are offered according to patients' values, interests, and preferences (Cannon &
Boswell 2016). The values increase practitioners' skills and knowledge to analyze research
outcomes effectively. Nurses are expected to think critically after being taught and encouraged,
which corresponds with evidence-based practices. Nurses' critical thinking skills require a
foundation on which proven research and tested data can be based. The proven research,
evidence-based practices, and a good foundation all connect to form a theory that research can
rely on and nurses can use to prove their practices.
3
Additionally, health professionals at all levels must identify challenges and arising
questions to address patients' needs and offer quality practices to discover appropriate
interventions suitable for every challenge. Health professionals are directly involved in research
projects that allow them to understand the best methods to publish for evidence-based practices.
Through different researches and publications, health professionals like advanced practice nurses
use research to solve health dilemmas. Nurses find platforms centered on tested clarifications
through nursing practices and methodical examinations from research to build a base for
procedures and care.
Moreover, research is a scientific procedure that anticipates outcomes through the use of
fundamental expertise. Research processes enhance the capacity of discipline through clarity and
visualized aspects. The discipline's ability to put i ...
1 Green Book Film Analysis Sugiarto MuljSilvaGraf83
1
Green Book Film Analysis
Sugiarto Muljadi
CSUN
COMS 321
Prof. Darla Anderson
12th May 2021
2
Green Book Analysis
Social stratification exists in almost every place that human’s dwell. Nonetheless, race
remains one of the most controversial elements of social stratification. The film Green Book
wants the audience to learn that there are no differences between humans regardless of their
race. While watching it, I was concerned that the script might have glossed over Shirley and
other African-Americans face. The newfound abundance of clean, inexpensive cars in the
1930s was more than a matter of convenience for middle-class Americans (IMDb, 2020). It
opened up new opportunities, giving them the freedom to fly across the world at their own
pace without having to rely on anyone. Also, in a constitutionally segregated world in some
areas and functionally segregated almost everywhere else, this was so for African Americans
(Lemire, 2018). However, while white travelers could travel with relative ease, stopping at
restaurants, bars, entertainment venues, and places to stay as they wished, African Americans
faced greater challenges. Staying in the wrong hotel or attempting to eat at the wrong
restaurant could result in you being ejected or worse.
The Negro Motorist Green Book was not the only travel guide for African-Americans,
but it was the most popular. Victor Hugo Green, an African-American mail carrier from
Harlem who served in Hackensack, New Jersey, designed it. Green worked on the effort for
almost three decades, from 1936 to 1966, soon after the Civil Rights Act was signed into law,
including a four-year pause during WWII (Diamond, 2018). The Green Book quickly
established itself as the most important document for black travelers in America, outlining
where they could eat, drink, and sleep without being abused or worse. Green Book depicts
various discriminatory prejudices that permeated American life in the early and mid-
twentieth centuries, ranging from snide remarks and racial epithets to outright hatred.
3
References
Diamond, A. (2018, November 20). The true story of the 'Green book' movie. Smithsonian
Magazine. https://www.smithsonianmag.com/arts-culture/true-story-green-book-
movie-180970728/
IMDb. (2020). Green book (2018). https://www.imdb.com/title/tt6966692/plotsummary
Lemire, C. (2018). Green book movie review & film summary (2018). Movie Reviews and
Ratings by Film Critic Roger Ebert | Roger Ebert.
https://www.rogerebert.com/reviews/green-book-2018
Week # 3 Case Study: Late and Later Documentation
Case Study: Late and Later Documentation
Based on the case study, critique the documentation presented by the healthcare provider and provide examples of whether the nurse follows or did not follow documentation requisites.
State what errors you found in the documentation and if you think the nurse followed the appropriate procedure ...
1
Film Essay 1
Film from 1940-1970
Garrett Lollis
ARTH 334
Professor Tom Fallows
April 04, 2021
2
Part 1
The film I chose was Ben-Hur (1959), which is an adventure/historical film by director
William Wyler. The film is a work of fiction based on the 1880 book Ben-Hur: A Tale of the
Christ by author Lee Wallace and is the third film adaption of multiple films based upon the
story of the fictional character Ben-Hur (Brayson, 2016). I personally enjoyed this 3 hour and
42-minute film due to the directors’ masterful work even though the film was made in 1959.
William Wyler utilized different cinematography and editing tools such as D.W.
Griffiths intercutting, panning, close-up, and dissolve techniques throughout the film to depict
each scene and enhance the quality of the film (Gutmann, 2010). With the use of D.W. Griffiths
cinematography/editing techniques, William Wyler managed to show different angles of a scene
better and pan for more use of the space because of newer technology unlike the straight on view
that had to be used in George Melies’s A Trip To The Moon (1902) due to the technology at
that time. Sound syncing really came a long way from the early 1900’s and this film perfectly
synced the sounds with what was happening in each scene (The History of Sound at the Movies,
2014). There is a scene about an ancient Roman naval battle taking place and I believe all parts
from sound, to editing, and cinematography come together during this battle scene. Before the
battle takes place the Admiral of the ship tests the boat rowers which were slaves by having them
run through different battle speeds of the ship. There is a drummer that helps keep the rowers in
sync, so as the Admiral yelled out “attack speed” the drummer started drumming and you can
hear the multitude of sounds from the music intensifying, the drummer drumming faster to the
changing ship speeds, to the exhaustion of the men as they row throughout this particular scene.
Once the battle begins, the battle music intensifies, and the director used cross-cutting to go
between the battle taking place outside the ship and back to the men under the deck rowing the
3
boat as the battle draws on. The director also used close-up shots to show the different
expressions on a few characters faces during the battle and finishes with the dissolve effect after
the battle is over to transition to Ben-Hur and the Admiral being stranded in the ocean. William
Wyler used the dissolve feature multiple time throughout the film to transition between locations
and nighttime and daytime, I really enjoy this feature because it makes the scenes flow smoothly
instead of just abruptly cutting off. Another interesting thing added into the film is an
intermission because the length of the film, this gives time to get a drink or more popcorn and
something I have only seen down in very few films. The dir ...
1 FIN 2063 INSURANCE FINANCIAL PLANNING Case AsSilvaGraf83
1
FIN 2063
INSURANCE FINANCIAL PLANNING
Case Assignment
Due Dates: Part I - Week 10 Part II - Week 12
Value: Part 1 – 10% Part II – 10% Total - 20% of final grade
1. This assignment represents a real client scenario. Create a report.
a. Read the case, the requirements and the marking rubric.
2. Your report must be typed, double-spaced in Times New Roman 12 or Arial/Calibri 11.
On the title page, include your name and student number.
3. As this is project is very similar in nature to a real life insurance planning scenario, present
your report just as you feel you would present a real life insurance planning
recommendation to a real life client.
4. The requirements at the end of the case indicate the expectations for your report, as does
the marking rubric.
Marks will be lost if your recommendations do not adequately meet or are not clearly
aligned with the clients’ goals. If due to lack of clarity or insufficient information you feel it
necessary to make an assumption, state the assumption in your report. That said, do not
assume the case away.
5. Although you may discuss this with other individual in the class, your report must be
unique. Any copying will result in a grade of zero.
2
Client Situation
You are a financial planner with a specialty in risk management. You’ve completed the LLQP and
are licensed to sell insurance products. You love your career and have built a successful practice
based mainly on referrals from your satisfied clients.
Jack, age 49, and Jill, age 48, are one of those referrals. Jack is Vice-President of Marketing at a
mid-sized systems firm. His salary is $190,000 + bonus. Last year his bonus was $40,000. Jill is
an accountant in private practice. She works from home and typically bills $150,000 a year
(roughly $100,000 after expenses). They feel pretty comfortable financially but have asked you to
flag any gaps that you can see in their risk management strategy. They also have specific questions
that they’d like you to address.
Jack and Jill are married with two children who live at home: Tracey, age 22 and Travis, age 17.
Jill’s mother, Lauren age 75, is widowed. Although she is financially independent, she moved in
with Jill and her family after the recent death of her husband. She contributes to the family’s
expenses and is especially devoted to her granddaughter, Tracey.
Tracey, a happy and outgoing woman, was born with Down Syndrome, a common genetic
disorder. Otherwise, Tracey is in good health and could easily live to age 60. Jack and Jill would
like to keep Tracey at home as long as possible but they are concerned about her ability to adapt if
one or both of them dies unexpectedly. As a result, they’re considering moving her into a group
home in their city. The group home provides full support to residents. The fee for this year is
$58,250. Tracey has seen the place and likes it, in no small part b ...
1 Faculty of Science, Engineering and ComputiSilvaGraf83
1
Faculty of Science, Engineering and Computing
CE7011 Management of Project, Risk, Quality and Safety
Reassessment Pack
April 2021
Content
Page No
Teaching Team 2
Assessment Summary 2
Health and Safety and Quality On line Test 3
Project Risk Management (PRM) Coursework 6
Assessment Submission and Feedback Form 12
Group Coursework Grade and Feedback Form 13
Individual Coursework Grade and Feedback Form 14
2
Faculty of Science, Engineering and Computing
Module Assessment Pack 2019/20
CE7011 Management of Project, Risk, Quality and Safety
Teaching Team
Staff Name Room Extension Contact: Email/Office hours
Module
Leader
Lecturer
Behrouz Zafari (BZ)
Diyana Binti Abd Razak (DR)
Illona Kusuma (IK)
Cliff Dansoh (CD)
Hasan Haroglu (HH)
PRMB1044
PRMB1057
PRMB1026
RV MB 212
PRMB1045
64820
[email protected]
Term-time office hours:
Tuesday: 16:00 – 17:30
Thursday: 16:00 – 17:30
[email protected]
[email protected][email protected][email protected]
Assessment Summary
Type Weight Set date Due date
Mark
by
Mark/work
return date
In-course
assessment
Examination
On-line test
(In-class)
30% 19 April
21
19 April
21
BZ 20 working
days after
submission
Written
assignment
70% 9 April 21
26 April
21
BZ 20 working
days after
submission
Examination No examination
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
3
Faculty of Science, Engineering & Computing
School of Natural and Built Environments
Department of Civil Engineering
CE7011 Management of Project, Risk, Quality and Safety
Assessments
Health and Safety and Quality On line Test
The online H&S and Quality test – will be available on Study Space under
assessments.
Date and Time of Test: Monday 19 April 2021, 9.00 am
Learning outcomes covered:
• Understand and contract toe roles of various parties in the successful
collaborative management of health and safety during both design and
construction phases of construction.
• Evaluate likelihood and impact of risk occurrence and procedures to manage
those risks, including health and safety risk.
• Appraise quality management techniques.
Instructions for taking the online test
The test is to be taken individually on-line, as per the timetable in the module
assessment pack. It will be available via Canvas/VLE. Once started, the test has to
be finished at one sitting. The maximum duration of the test is 80 minutes.
The test will be an open book test i.e. you can refer to notes books etc.
If your access to the University computer system is blocked or suspended for any
reason (e.g. financial) during the test tim ...
1
EARLY CHILDHOOD AND
CHILD DEVELOPMENT
Lesson Plan Handbook
Developed by Kristina Bodamer and Jennifer Zaur
September 2014
2
TABLE OF CONTENTS
About This Handbook 3
Lesson Plan Template 4
Goals 5
Objectives 6
Standards 7
Materials 11
Introduction 12
Lesson Development 14
Differentiation 16
Assessment 18
Closing 20
Sample Academic Lesson 21
Sample Developmental Lesson 23
Lesson Planning Resources 25
References 27
3
ABOUT THIS HANDBOOK
Purpose of the Handbook
This handbook was developed to provide Ashford University Early Childhood Education and
Child Development students with a resource to utilize when creating effective lesson plans.
Educators must be able to create an effective lesson plan so they can successfully teach
children the developmental and academic skills they need to grow, develop, and learn. As
Kostelnik, Rupiper, Soderman, & Whiren (2014) explain, “Planning is a mental process, and a
lesson plan is the written record of that process” (p. 81).
Design of the Handbook
“A lesson plan is the instructor’s road map of what students need to learn and how it will be
done effectively” (Milkova, 2014, para. 1). This handbook is your “road map” to creating
effective lesson plans. Each section of the handbook will serve as a different stop along your
journey. With each stop you make, you will gain important information about a component
of a lesson plan: what it is, its purpose, how to effectively develop each section of the lesson
plan, and concrete examples that model the individual sections. By the end of your trip, you
will be able to create effective lesson plans that will allow your students to learn the
developmental and academic skills they need to master. So, pack your bags and come along
for a fun and informative ride.
4
LESSON PLAN TEMPLATE
Content Area or Developmental Focus:
Age/Grade of Children:
Length of Lesson:
Goal
Objective
Standards Included
Materials
Introduction
Lesson Development
Differentiation
Assessment
(Practice/Check for
Understanding)
Closing
5
GOALS
What is a lesson goal?
A lesson goal guides the direction of the lesson. “Goals come from an outside source [such
as] a text, program goals, or state standards”(Kostelnik et al., 2014, p. 85 ). The goal is a
broad, general statement that tells you what you want your students to do when the lesson
is complete. Think of the goal of the lesson as a target that you are trying to reach. The goal
of the lesson should provide the framework for you to create a more detailed and
measurable learning objective.
Why are lesson goals important?
Lesson goals are important for s ...
1 Case Grading Procedure Your grade from each case SilvaGraf83
1
Case Grading Procedure
Your grade from each case analysis is determined using the following assessment rubrics:
Ethical Decision-Making Rubric - EDR
School of Business Writing Assessment Rubric – WAR
Review each of the rubrics below to see what is expected of you.
Your grade will be calculated as follows:
𝑃𝑒𝑟𝑐𝑒𝑛𝑡 𝐺𝑟𝑎𝑑𝑒 = 0.85 (
𝑃𝑜𝑖𝑛𝑡𝑠 𝑒𝑎𝑟𝑛𝑒𝑑 𝑜𝑛 𝑡ℎ𝑒 𝐸𝐷𝑅
50
) + 0.15 (
𝑃𝑜𝑖𝑛𝑡𝑠 𝑒𝑎𝑟𝑛𝑒𝑑 𝑜𝑛 𝑡ℎ𝑒 𝑊𝐴𝑅
70
)
The total case grade will be out of 50 points.
𝑇𝑜𝑡𝑎𝑙 𝑃𝑜𝑖𝑛𝑡𝑠 𝑜𝑛 𝐴𝑠𝑠𝑖𝑔𝑛𝑚𝑒𝑛𝑡 = 𝑃𝑒𝑟𝑐𝑒𝑛𝑡 𝐺𝑟𝑎𝑑𝑒 × 50
2
Ethical Decision-Making Rubric
Evaluators are encouraged to assign a zero to any work sample or collection of work that does not meet minimum performance levels.
Case Analysis Steps Standards Points
Ethical Issues:
Issue Identification All ethical issues are
properly identified (4
points)
Most ethical issues are
properly identified (3
points)
Some ethical issues are
properly identified (2 – 1
points)
No ethical issue is
properly identified (0
points)
Issue Definitions/Descriptions
and Factual Support
Of those ethical issues
identified, all are
adequately defined/
described and supported
by case facts (6 points)
Of those ethical issues
identified, most issues
identified are adequately
defined/ described and
supported by case facts (5
– 4 points)
Of those ethical issues
identified, some issues
identified are adequately
defined/ described and
supported by case facts (3
– 1 points)
No issue identified is
adequately
defined/described and
supported by case facts (0
points)
Stakeholder Analysis:
Stakeholder Identification All key stakeholders are
properly identified (6
points)
Most key stakeholders are
properly identified (5 – 4
points)
Some key stakeholders are
properly identified (3 – 1
points)
No key stakeholder is
properly identified (0
points)
Identification of Stakes Of those stakeholders
identified, all important
stakes are properly listed
(4 points)
Of those stakeholders
identified, most important
stakes are properly listed
(3 points)
Of those stakeholders
identified, some important
stakes are properly listed
(2 – 1 points)
Of those stakeholders
identified, no important
stakes are properly listed
(0 point)
Ethical Decisions
All short- and long-term
ethical issues are resolved
through the use of ethical
decisions (10 points)
Most short- and/or long-
term ethical issues are
resolved through the use
of ethical decisions (9 – 6
points)
Some short- and/or long-
term ethical issues are
resolved through the use
of ethical decisions (5 – 1
points)
Alternate decisions or
unethical decisions are
used to attempt to resolve
the ethical issues
identified (0 points)
Nonconsequentialist Analysis:
Subcharacteristic Identification
and Definition
Four of t
1 Kilimanjaro is a snow-covered mountain 19,710 feet hiSilvaGraf83
1
Kilimanjaro is a snow-covered mountain 19,710 feet high, and is said to be the highest mountain in Africa.
Its western summit is called the Masai "Ngaje Ngai," the House of God. Close to the western summit there
is the dried and frozen carcass of a leopard. No one has explained what the leopard was seeking at that
altitude.
The Snows of Kilimanjaro
By Ernest Hemingway, 1938
THE MARVELLOUS THING IS THAT IT S painless," he said. "Tha 's ho o kno
when it starts."
"Is it really?"
"Absolutely. I'm awfully sorry about the odor though. That must bother you."
"Don't! Please don't."
"Look at them," he said. "Now is it sight or is it scent that brings them like that?"
The cot the man lay on was in the wide shade of a mimosa tree and as he looked out past
the shade onto the glare of the plain there were three of the big birds squatted obscenely,
while in the sky a dozen more sailed, making quick-moving shadows as they passed.
"They've been there since the day the truck broke down," he said. "Today's the first time
any have lit on the ground. I watched the way they sailed very carefully at first in case I
ever wanted to use them in a story. That's funny now.""I wish you wouldn't," she said.
"I'm only talking," he said. "It's much easier if I talk. But I don't want to bother you."
"You know it doesn't bother me," she said. "It's that I've gotten so very nervous not being
able to do anything. I think we might make it as easy as we can until the plane comes."
"Or until the plane doesn't come."
"Please tell me what I can do. There must be something I can do.
"You can take the leg off and that might stop it, though I doubt it. Or you can shoot me.
You're a good shot now. I taught you to shoot, didn't I?"
"Please don't talk that way. Couldn't I read to you?"
2
"Read what?"
"Anything in the book that we haven't read."
"I can't listen to it," he said." Talking is the easiest. We quarrel and that makes the time
pass."
"I don't quarrel. I never want to quarrel. Let's not quarrel any more. No matter how
nervous we get. Maybe they will be back with another truck today. Maybe the plane will
come."
"I don't want to move," the man said. "There is no sense in moving now except to make it
easier for you."
"That's cowardly."
"Can't you let a man die as comfortably as he can without calling him names? What's the
use of clanging me?"
"You're not going to die."
"Don't be silly. I'm dying now. Ask those bastards." He looked over to where the huge,
filthy birds sat, their naked heads sunk in the hunched feathers. A fourth planed down, to
run quick-legged and then waddle slowly toward the others.
"They are around every camp. You never notice them. You can't die if you don't give up."
"Where did you read that? You're such a bloody fool."
"You might think about some one else."
"For Christ's sake," he said, "that's been my trade."
He lay then and was quiet for a while and looked across the ...
1
Assignment 2 Winter 2022
Problem 1
Assume you have the option to buy one of three bonds. All have the same degree of default risk
and mature in 15 years. The first is a zero-coupon bond that pays $1,000 at maturity. The
second has a 7 percent coupon rate and pays the $70 coupon once per year. The third has a 9
percent coupon rate and pays the $90 coupon once per year.
a. If all three bonds are now priced to yield 8 percent to maturity, what are their prices?
b. If you expect their yields to maturity to be 8 percent at the beginning of next year, what will
their prices be then? What is your before-tax holding period return on each bond? If your tax
bracket is 30 percent on ordinary income and 20 percent on capital gains income, what will
your after-tax rate of return be on each? Assume you do not sell the bonds.
c. Recalculate your answer to (b) under the assumption that you expect the yields to maturity on
each bond to be 7 percent at the beginning of next year.
d. Re-do the calculations in parts b and c above, assuming you will sell the bonds at the end of the
year.
Problem 2
A University endowment fund has sought your advice on its fixed-income portfolio strategy.
The characteristics of the portfolios current holdings are listed below:
Market
Credit Maturity Coupon Modified Value of
Bond Rating (yrs.) Rate (%) Duration Convexity Position
A Cnd. Govt. 3 0 2.727 9.9 $30,000
B A1 10 8 6.404 56.1 $30,000
C Aa2 5 12 3.704 18.7 $30,000
D Agency 7 10 4.868 32.1 $30,000
E Aa3 12 0 10.909 128.9 $30,000
$150,000
a) Calculate the modified duration for this portfolio.
b) Suppose you learn that the modified duration of the endowment’s liabilities is 6.5 years.
Identify whether the bond portfolio is: i) immunized against interest rate risk, ii) exposed to net
price risk, or iii) exposed to net re-investment risk. Briefly explain what will happen to the net
position of the endowment fund if in the future there is a significant parallel upward shift in the
yield curve.
c) Your current active view for the fixed income market over the coming months is that Treasury
yields will decline and corporate credit spreads will also decrease. Briefly discuss how you
could restructure the existing portfolio to take advantage of this view.
2
Problem 3
A 20-year maturity bond with a 10% coupon rate (paid annually) currently sells at a yield to
maturity of 9%. A portfolio manager with a 2-year horizon needs to forecast the total return on
the bond over the coming 2 years. In 2 years, the bond will have an 18-year maturity. The analyst
forecasts that 2 years from now, 18-year bonds will sell at yield to maturity of 8%, and that
coupon payments can be reinvested in short-term securities over the coming 2 years at a rate of
7%.
a) What is the 2-year return on the bond
b) What will be the rate of return the manager forecasts that in 2 years the yiel ...
1
COU 680 Adult Psychosocial Assessment Sabrina
Date of appointment: Today Time of appointment: 5:00 pm
Client Name: Sabrina Hinajosa Age: 29 DOB: 3/23/89
Gender: Male Female Transgender Preferred Name/Nickname: N/A
Ethnicity: Hispanic Non‐Hispanic Race: Caucasian
Current Marital/Relationship Status: Single Married Divorced Widowed Domestic Partnership
Name of Person completing form: Sabrina Relationship to client: Self
PRESENTING PROBLEM (Briefly describe the issues/problems which led to your decision to seek therapy services):
I recently lost my mother-in-law to a sudden heart attack immediately prior to the recent hurricane. Within a matter
of a single day I lost the mother figure in my life, was evacuated from my home, and had a hurricane destroy parts
of my house. I’m completely overwhelmed, sad, and angry at the world.
How severe, on a scale of 1‐10 (with 1 being the most severe), do you rate your presenting problems?
MOST SEVERE 1 2 3 4 5 6 7 8 9 10 LEAST SEVERE
PRESENTING PROBLEM CATEGORIZATION: (Please check all the apply and circle the description of symptom)
Symptoms causing concern, distress or impairment:
Change in sleep patterns (please circle): sleeping more sleeping less difficulty falling asleep
difficulty staying asleep difficulty waking up difficulty staying awake
Concentration: Decreased concentration Increased or excessive concentration
Change in appetite: Increased appetite Decreased appetite
Increased Anxiety (describe): I have a lot of fear of the unknown. Everything feels out of my control.
Mood Swings (describe): I’m irritable all of the time. I go back and forth between extreme bouts of sadness
and complete anger and rage at the situation. The only place I feel calm is with my kids
and only because I really focus on making sure they are ok.
Behavioral Problems/Changes (describe): I struggle to stay focused on anything other than taking care of
my kids. I feel aimless and purposeless and have stopped putting forth much effort at work or in our home.
Everything just seems both overwhelming and pointless.
Victimization (please circle): Physical abuse Sexual abuse Elder abuse Adult molested as child
Robbery victim Assault victim Dating violence Domestic Violence
Human trafficking DUI/DWI crash Survivors of homicide victims
Other:
2
Other (Please describe other concerns):
How long has this problem been causing you distress? (please circle)
One week One month 1 – 6 Months 6 Months – 1 Year Longer than one year
How do you rate your current level of coping on a scale of 1 – 10 (with 1 being unable to cope)?
UNABLE TO COPE 1 2 3 4 5 6 7 8 9 10 ABLE TO COPE
EMPLOYMENT:
Currently Employed? Yes No If employed, what is your occupation? Bank teller
Where are you working? XYZ Bank
How long? 3 Days/Months/Years
Do you enjoy your current job? Yes No What do you like/ ...
1 Literature Review on How Biofilm Affect theSilvaGraf83
1
Literature Review on How Biofilm Affect the Patient Recovery at the Hospital
Student’s Name
Professor’s Name
Course Name
Date
2
Introduction
Regulating biofilms for injury and insertion can have a variety of adverse effects on
patient well-being, including delayed recovery and implant evacuation. Biofilm drugs currently
do not completely destroy or prevent microbial colonization, indicating the need for further
research. The final review of drugs for biofilms focuses on components of nanotechnology-based
drug delivery, combination therapy, and coupling repair. Ultrasonic cleaning and hydrogels, as
well as recent improvements in incorporation, have great potential for use in discrete trauma and
medicine applications. This study reviews various literatures on the development of
microorganisms in biofilms and how it affects patient recovery at the hospital.
Patients with biofilms wounds excrete various microbes from their own skin and current
state, and if they receive hospitalization for treatment, they are likely to receive MRE and HAI
from surfaces, patients, staff, and emergency department equipment (Wu et al., 2018). This
literature states that such patients have high levels of biofilm contamination for biofilm reduction
applications in consuming patients include silver and various metals. Other elements indicating
this condition include disinfectants, hydrogels, light and sonic treatments to initiate atomic
sensitization to deliver dynamic oxygen (Wu et al., 2018). Small particles of these contaminants
allow penetration into the dividing layer of cells, glycans, lactobacilli and treatment with phages.
Other scholars such as Muhammad et al. (2020) and Barzegari et al. (2020) assert that the
accumulation of microorganisms can be immobile and live and attached to the surface. The
regimen of this group of people is not the same as that of planktonic development, where
microorganisms are isolated and flexible in environment (Muhammad et al., 2020). Cecillus cells
differ from planktonic cells in their morphology, physiology and qualitative articulation. The
ability to adhere to and thrive on surfaces such as biofilms is a gradual survival process that
3
allows microorganisms to colonize the zone (Muhammad et al., 2020). Microbes are constantly
changing from planktonic aggregates to sedentary ones. This variety of conditions is key for cells
as they allow rapid changes in their natural state.
Wound swelling can be characterized as the ability of microorganisms to thrive when
antimicrobial compounds are present in the climate. The obstructive component is hereditary and
prevents the antitoxin from working for its purpose (Barzegari et al., 2020). This literature
indicates that the term resistance should be used for microbes that may be caused by high-class
antibiotics but whose development is delayed. This element, which explicitly describes the life ...
1
Canterbury Tales
(c. 12th century)
What do I need to read?
“The Canterbury Tales General Prologue”
“The Miller’s Prologue and Tale”
“The Wife of Bath’s Prologue and Tale”
“The Pardoner’s Prologue and Tale”
Who is the author?
Geoffrey Chaucer (1343 – 1400). Called the Father of the English Language as well
as the Morning Star of Song, Geoffrey Chaucer, after six centuries, has retained
his status as one of the three or four greatest English poets. He was first to
commit to lines of universal and enduring appeal a vivid interest in nature, books,
and people.
As many-sided as Shakespeare, he did for English narrative what Shakespeare did
for drama. If he lacks the profundity of Shakespeare, he excels in playfulness of
2
mood and simplicity of expression. Though his language often seems quaint, he was
essentially modern. Familiarity with the language and with the literature of his
contemporaries persuades the most skeptical that he is nearer to the present than
many writers born long after he died.
---Courtesy of Compton’s Learning Company
Background Lecture
Chaucer’s father, an influential wine merchant, was able to secure Geoffrey a
position as a page in a household connected to King Edward III. Chaucer’s duties as
a page were humble, but they allowed him the opportunity to view the ruling
aristocracy, thus broadening his knowledge of the various classes of society. While
serving in the English army, Chaucer was captured and held prisoner in France.
After his release, he held a number of government positions.
While in his twenties, Chaucer began writing poetry, and he continued to write
throughout his life. Over the years, his writing showed increasing sophistication
and depth, and it is recognized as presenting penetrating insights into human
character. In The Canterbury Tales, critics say that the author shows an absolute
mastery of the art of storytelling.
The Canterbury Tales are also said to present “a cavalcade of fourteenth-century
English life” because on this pilgrimage to Canterbury the reader gets to meet a
cross-section of the people from Chaucer’s time.
Canterbury, located about fifty miles southeast of London, was a favorite
destination for pilgrims. In fact, Chaucer himself made a pilgrimage there. While
he did not set out on the pilgrimage looking for material to use in his writing, he
was so impressed by the mix of company that he had met at the Tabard Inn that
he was inspired to write what was to become his masterpiece.
3
Selected Canterbury Tales Terms and Definitions
Allegory - a story that represents abstract ideas or moral qualities. As such, an
allegory has both a literal level and a symbolic level of meaning. Example: Gulliver’s
Travels.
Allusion - a reference to a person, place, poem, book, or movie outside of the story
that the author expects the reader will recognize.
Fable - ...
1 Math 140 Exam 2 COC Spring 2022 150 Points SilvaGraf83
1
Math 140 Exam 2
COC Spring 2022
150 Points
Question 1 (30 points)
Match the following vocabulary words in the table below with the corresponding definitions.
Confidence Interval Hypothesis Test Standard Error Alternative Hypothesis
Randomized Simulation Random Sample Random Assignment Random Chance
Population Sampling Variability Significance Level Type II Error
One-Population Mean
T-Test Statistic
Quantitative Data One-Population
Proportion Z-Test
Statistic
Categorical Data
Critical Value Statistic Parameter Census
Type I Error Bootstrap Distribution Margin of Error Beta Level
Bootstrapping Null Hypothesis P-value Point Estimate
a. A number we compare our test statistic to in order to determine significance. In a sampling
distribution or a theoretical distribution approximating the sampling distribution, the critical
value shows us where the tail or tails are. The test statistic must fall in the tail to be significant.
b. Also called the Alpha Level. If the P-value is lower than this number, then the sample data
significantly disagrees with the null hypothesis and is unlikely to have happened by random
chance. This is also the probability of making a type 1 error.
c. A statement about the population that does not involve equality. It is often a statement about a
“significant difference”, “significant change”, “relationship” or “effect”.
d. The collection of all people or objects you want to study.
e. A number calculated from sample data in order to understand the characteristics of the data.
f. When biased sample data leads you to support the alternative hypothesis when the alternative
hypothesis is actually wrong in the population.
g. Another word for sampling variability. The principle that random samples from the same
population will usually be different and give very different statistics.
h. Data in the form of numbers that measure or count something. They usually have units and
taking an average makes sense.
i. Taking many random samples values from one original real random sample with replacement.
j. Collecting data from everyone in a population.
2
k. Collecting data from a population in such a way that every person in the population has an
approximately equal chance of being chosen. This technique tends to give us data with less
sampling bias.
l. The probability of getting the sample data or more extreme because of sampling variability (by
random chance) if the null hypothesis is true.
m. The sample proportion is this many standard errors above or below the population proportion in
the null hypothesis.
n. Take a group of people or objects and randomly put them into two or more groups. This is a
technique used in experiments to create similar groups. Similar groups help to control
confounding variables so that the scientist can prove cause and effect.
o. Data in the form of labels that tell us something about the people ...
1 Lessons from the past How the deadly second waveSilvaGraf83
1
Lessons from the past: How the deadly
second wave of the 1918 ‘Spanish flu’
caught Dallas and the U.S. by surprise
Health concerns about the 2020 coronavirus pandemic are rooted in the
catastrophic second wave of the 1918 pandemic, which hit between
September and November of that year.
By David Tarrant
9:00 AM on Jul 3, 2020
https://www.dallasnews.com/news/2020/07/03/lessons-from-the-past-how-the-deadly-second-
wave-of-the-1918-spanish-flu-caught-dallas-and-the-us-by-surprise/
Illustration by staff artist Michael Hogue.(Michael Hogue / Michael Hogue illustration)
As August gave way to September of 1918, few people were thinking about the
influenza that would soon sweep across Texas and the rest of the country with the speed and
deadly ferocity of a firestorm.
There had been a relatively mild version of the virus in the spring of that year, mostly
affecting troops mobilizing to go off to World War I over in Europe. But by summer the disease
known at the time as the Spanish flu had been largely forgotten.
The front pages of The Dallas Morning News were dominated by news of American troops
pouring into Europe for what would come to be known as World War I.
But that would quickly change. By the end of September, a second wave of the flu, far
deadlier, would sweep across the country, hitting Dallas and other large cities hard.
When health experts worry about the course of the 2020 coronavirus pandemic, they
often look back at the second wave of the 1918 pandemic, between September and November,
https://www.dallasnews.com/author/david-tarrant
2
when influenza cases overwhelmed hospitals and medical staffs across the country and the dead
piled up faster than they could be buried.
In Dallas that year, the city’s chief health officer, A.W. Carnes, waved off the fast-
approaching pandemic as not much more than the common cold. In a major blunder, he permitted
a patriotic parade in late September that attracted a cheering crowd of thousands jammed
together downtown.
Cases of influenza promptly spiked.
The second wave would produce most of the deaths of the pandemic, which experts now
estimate at 50 million to 100 million worldwide. In the United States, 675,000 people died from
the virus.
The Dallas Morning News on Sept. 27, 1918, reported the rapid spread of the Spanish flu. Despite the worsening
conditions, Dallas medical officials hesitated to impose restrictions on public gatherings for more than two weeks.
As it did then, the world is struggling with a virus for which there is no vaccine. COVID-19,
the sickness caused by the new coronavirus, has advanced unabated around the world since it first
appeared in China late last year. By the end of June, the number of deaths worldwide exceeded
500,000.
Like the Spanish flu in 1918, the new coronavirus isn’t showing signs of fading away
anytime soon. Texas ended June with alarm lights flashing as new COVID-19 cases set records
daily ...
1 Lockheed Martin Corporation Abdussamet Akca SilvaGraf83
1
Lockheed Martin Corporation
Abdussamet Akca
Lockheed Martin Corporation
To: Jack Harris
From: vice president governmental affairs
Date:15 February 2021
Sub: under Lockheed Martin Corporation (overview)
2
I am here to state that this is the overview of Lockheed Martin Corporation and Jack
Harris is the CEO of the consulting firm consulted by the CEO of Lockheed Martin Corporation,
crisis consulting.
Business profile
In the contemporary world, there are many challenges facing companies in different
industries in both developed countries and undeveloped countries. There is a great need to
understand the potential risks that may face the business to take care of the shareholder interests,
meet the legitimate consistency, and secure the required resources such as human resources
scholarly and reputational resources. Customers are helped with data by the shareholder value-
added. It also helps in another backup and preparation so that people in the organization are
ready to distinguish risk and so that they can quickly react to crisis consulting (Dove et al.,
2018). The SVAs problem consulting can work with customer administration to identify the
potential turmoil that Lockheed martin corporation is likely to face. The understanding of using
fitting systems and methodologies and the advancement of the same make it possible to oversee
and relieve emergencies through computerized systems. It is possible to utilize and outline
recreations by testing setups and arrangements. Through the operational reviews and the
preparation of potential crises in the Lockheed Martin Corporation, one’s status is also protected.
If the problem exceeds, then the SVAs group can react to the expansive scope of the crisis to
develop the best action to solve these crises.
Crisis consulting international has supplied security and crisis administration to different
organizations such as the Christian evangelist. The concern consulting international has been
helping these groups evaluate risk, improve policy creations, site overviews, and arrange training
staff, crisis administration group, meetings management of occasions, among others. Other
3
activities include risk assessment, prioritization of risks, evaluation, and comprehension of
corporate risk profile. Crisis consulting international uses scientific procedures to prepare
customers in perceiving and measuring risks to understand the effect of these risks so that they
can use the available methodologies to oversee risk and avoid it (Davies, 2019). SVA is used in
the business impact assessment process to break down the business with the end goal in mind.
That builds up top to bottom comprehension of recognizing the primary regions primarily
dependent on the company. This audit aims to establish more extensive deterrent ways of risk
arrangements and prepare programs. SVA can also be incorporated with working wit ...
1 Lab 9 Comparison of Two Field Methods in a ScienSilvaGraf83
1
Lab 9: Comparison of Two Field Methods in a
Scientific Report/Paper Format
Minimum Content of the Scientific Report
Title
The title should be a brief summary statement about your paper. Your title will be what
is most commonly cited and will be the “target” of topical searches via the internet.
Choose your words carefully. As short and as concise a title as possible is best.
Each student will come up with the title! You might consider waiting until after
completing the report to finalize the title.
Abstract
Think of the abstract as a short summary of your paper that could stand-alone as a
publication. The abstract should include, in order: a summary of the introduction,
methods, results, and discussion. However, you may include only key results and key
discussion points in the abstract. Do not include reference to figures and tables, and
don’t use abbreviations. Don’t include references in the abstract. This is the hardest
section of the paper to write, and should be written after you complete the other
sections.
Minimum of 200 and maximum of 300 words in a single-paragraph format.
Introduction
The introduction should include a detailed explanation about why you are doing the
study, i.e., the basis for your study.
This section should include observations or results from previous studies that support
the basis for your study, but not the results or discussion or conclusions drawn from the
results of your project.
Follow these observations or results from previous studies with the questions or
hypotheses of your study.
The introduction should end with a brief paragraph that summarizes the setting, scope,
and justification or importance of the study. This is a lead-in paragraph to the rest of the
paper.
Minimum of 1/2 page of text in length with one or more paragraphs.
2
Methods
Write the methods in the past tense.
This should be a detailed, step-by-step, description of how you did the study.
Include details on the equipment and materials used (see list below).
Include the approach to data analysis and cite any statistical or other applications used
to input, manage, graph, or analyze the data.
Include citations for any standard or previously published methods used.
Write this section with enough detail that someone else could duplicate your study or
conduct a similar study with only your methods section available.
Include a map showing the location, sampling area, and plot and belt transect in the
sampling area.
Minimum of one page of text in length with multiple paragraphs.
Results
This the “what you got” section.
Write the results in the past tense.
This sections includes any data or results tables and graphs you have.
This is a summary of your key results from data, graphs, and/or results of statistical
analyses.
You are not required to include a statistical analysis(-es).
You ar ...
1 LAB MODULE 5 GLOBAL TEMPERATURE PATTERNS Note PSilvaGraf83
1
LAB MODULE 5: GLOBAL TEMPERATURE PATTERNS
Note: Please refer to the GETTING STARTED lab module to learn how to maneuver
through and answer the lab questions using the Google Earth ( ) component.
KEY TERMS
You should know and understand the following terms:
Air temperature Heat index Temperature anomalies
Altitude Kelvin (K) Temperature averages
Ambient temperature Latitude Thermopause
Axial Tilt Maritime effect Thermosphere
Celsius (C) Mesopause Tropopause
Continentality, or
Continental effect
Mesosphere Troposphere
Stratopause Urban heat island
Environmental Lapse Rate Stratosphere Urban heat island effect
Exosphere Structure of the atmosphere Wind chill
Fahrenheit (F) Surface temperature
LAB MODULE LEARNING OBJECTIVES
After successfully completing this module, you should be able to the following
tasks:
Describe the differences between air and surface temperature
Explain heat index and wind chill
Explain the urban heat island effect
Describe the structure of the atmosphere
Describe large scale factors influencing temperature
Describe local factors influencing temperature
2
INTRODUCTION
This lab module explores the global surface and air temperatures of Earth and
Earth’s atmosphere. Topics include the structure of the atmosphere, local and
global factors influencing temperature, and temperature anomalies. The modules
start with four opening topics, or vignettes, which are found in the accompanying
Google Earth file. These vignettes introduce basic concepts of the internal structure
of the Earth. Some of the vignettes have animations, videos, or short articles that
will provide another perspective or visual explanation for the topic at hand. After
reading the vignette and associated links, answer the following questions. Please
note that some links might take a while to download based on your Internet speed.
Expand the INTRODUCTION folder.
Read Topic 1: Surface and Air Temperature
Question 1: How do the surface temperatures of the countries in the
northern latitudes (for example, Canada, Iceland, Norway, and Russia)
compare to those of northern Africa (for example, Algeria, Egypt, Libya,
Morocco, and Sudan)?
A. The temperatures are higher in the northern latitudes during summer
months when net radiation is higher.
B. The temperatures are lower in north Africa during the summer months
when net radiation is higher in northern latitudes.
C. Temperatures are lower in northern latitudes year-round.
D. Temperatures are only lower in the northern latitudes during winter
months.
Read Topic 2: Measuring Temperature
Question 2: Considering water freezes (or alternatively, melts) at 0˚C,
determine from the map which countries or landmasses have an annual
mean temperature around 0˚C.
A. Canada and Norway
B. The United States and the United Kingdom
C. Greenland and Antarctica
D. Russia and Antarctica
3
...
1 Instructions for Coming of Age in Mississippi SilvaGraf83
1
Instructions for Coming of
Age in Mississippi
Due Sunday, April 25th, 2021
Late papers will be penalized. Failure to turn in this assignment will result in
the automatic failure of the class.
Anne Moody’s Coming of Age in Mississippi is an autobiographical presentation of
her life and experiences in the segregationist South during the middle third of the
20th Century. Although Moody was intensively involved in the civil rights
movement of the 1950’s and 1960’s, the real value of her autobiography is that she
describes what it was like to grow up in Mississippi long before she became a civil
rights activist.
Your book essay for Coming of Age in Mississippi should explore and discuss the
following topics and questions:
1. Begin with a brief overview of the book: in general, what is it about, who wrote
it, etc.
2. Moody’s decision to become engaged in the political activism central to the
Civil Rights Movement was a result of her experiences at both work and play
growing up in Mississippi. What kinds of incidents from her life led Moody to
become politically active in the movement? For example, what does she notice
about how she is treated as a black person in Southern white society?
3. Women played an important role in Moody’s life. Using examples from her
autobiography, discuss what Moody learned about race, class and sexual
orientation from the women around her. Who were the most important women in
her life? Discuss each and explain why that person was so important.
4. Moody was a participant and observer of some of the most important historical
events of the 1950’s and 1960’s. How did she view and describe these events – for
example, the murder of Emmitt Till, the sit-in protests, the voter registration drive
in Mississippi, Ku Klux Klan activities and the assassination of Medgar Evars and
2
others? In general, what do her descriptions tell you about the struggle for civil
rights?
5. What did you think of this book? Did you like it/ not like it? Explain why.
Writing Instructions:
1. Use the above questions/topics as your paper outline and answer them in the
order they are presented.
2. Use some common sense in how much you write on each topic. The general
overview of the book, for example, can be covered in one relatively brief
paragraph. Other topics may require more extensive coverage. The main body of
your paper should focus on topics 2-4. You should explore those thoroughly and
back up any general comments with specific details that illustrate and support
them. Topics 1 and 5 should be about a paragraph in length.
3. Although I don’t grade in terms of the length of the paper, under most
circumstances I would expect a paper somewhere within the range of 4-5 pages.
As a general rule, it’s better to write more than less.
4. The paper must be typed using a standard word processing program, double-
spaced using norm ...
1
Institutional Assessment Report
2012-13
The primary purpose for assessment is the assurance and improvement of student learning and
development; results are intended to inform decisions about course and program content, delivery,
and pedagogy. The Institutional Assessment Report summarizes annual assessment processes,
results and success indicators at the program, co-curricular, core and institutional levels.
I. Program assessment
A total of 117 degree and certificate programs and 13 co-curricular units assessed student learning
in 2012-13. Assessment reports reside in the Assessment Reporting Management System (ARMS).
Most programs measured multiple learning outcomes and used multiple measures. Direct measures
examine or observe student knowledge, skills, attitudes or behaviors. The most frequently used
direct measures in undergraduate programs are written assignments and locally developed exams,
tests or quizzes. Commonly used direct measures in graduate programs include oral presentations
or exhibition, research papers/projects, and locally-developed exams, tests or quizzes (Table 1).
Table 1: Percent of Academic Programs Reporting Direct Measures in ARMS
Undergraduate Graduate
N = 52 N = 65 (3 certificate)
Standardized instruments 29% 14%
Locally-developed
exam/test/quiz
40% 40%
Essay question on exam 29% 17%
Pre- and post-measures 10% 3%
Written assignment 42% 32%
Portfolio 4% 12%
In-class discussions 10% 11%
Oral presentation or
exhibition
23% 51%
Thesis / Dissertation 32%
Simulations 4% 2%
Formal evaluation of practical
skills
12% 22%
Research paper/project 25% 40%
Final Project 29% 14%
Other 17% 14%
2
Indirect measures evaluate perceived learning, and may be used to supplement direct measures.
Surveys are commonly used indirect measures; in graduate education, student self-assessments are
most frequently used (Table 2).
Table 2: Percent of Academic Programs Reporting Indirect Measures in ARMS
Undergraduate Graduate
Surveys 17% 11%
Interviews or focus groups 2% 2%
Data indicators (job
placement, admission to
graduate education)
4% 9%
Comparisons with peers 4% 3%
Student Self-Assessment 2% 15%
Other 4% 8%
Co-curricular programs, especially those in the Division of Student Affairs, are more likely to
assess student learning and development through self-report (surveys and student self-assessments)
than through direct measures (Tables 3 and 4).
Table 3: Percent of Co-curricular Units1 Reporting Direct Measures in ARMS
(N = 13)
Reflection 15%
Academic written assignment/Research
questions
23%
Exam 8%
Oral presentation 8%
Observations 23%
Supervisor ratings 15%
Performance reviews 8%
Other 31%
Table 4: Percent of Co-curricular Units1 Reporting Indirect Measures in ARMS
Surveys 69%
Student Self-Assessment 62%
Data Indicators 8%
Benchmarks/Compa ...
Read| The latest issue of The Challenger is here! We are thrilled to announce that our school paper has qualified for the NATIONAL SCHOOLS PRESS CONFERENCE (NSPC) 2024. Thank you for your unwavering support and trust. Dive into the stories that made us stand out!
Welcome to TechSoup New Member Orientation and Q&A (May 2024).pdfTechSoup
In this webinar you will learn how your organization can access TechSoup's wide variety of product discount and donation programs. From hardware to software, we'll give you a tour of the tools available to help your nonprofit with productivity, collaboration, financial management, donor tracking, security, and more.
The Indian economy is classified into different sectors to simplify the analysis and understanding of economic activities. For Class 10, it's essential to grasp the sectors of the Indian economy, understand their characteristics, and recognize their importance. This guide will provide detailed notes on the Sectors of the Indian Economy Class 10, using specific long-tail keywords to enhance comprehension.
For more information, visit-www.vavaclasses.com
We all have good and bad thoughts from time to time and situation to situation. We are bombarded daily with spiraling thoughts(both negative and positive) creating all-consuming feel , making us difficult to manage with associated suffering. Good thoughts are like our Mob Signal (Positive thought) amidst noise(negative thought) in the atmosphere. Negative thoughts like noise outweigh positive thoughts. These thoughts often create unwanted confusion, trouble, stress and frustration in our mind as well as chaos in our physical world. Negative thoughts are also known as “distorted thinking”.
How to Make a Field invisible in Odoo 17Celine George
It is possible to hide or invisible some fields in odoo. Commonly using “invisible” attribute in the field definition to invisible the fields. This slide will show how to make a field invisible in odoo 17.
Synthetic Fiber Construction in lab .pptxPavel ( NSTU)
Synthetic fiber production is a fascinating and complex field that blends chemistry, engineering, and environmental science. By understanding these aspects, students can gain a comprehensive view of synthetic fiber production, its impact on society and the environment, and the potential for future innovations. Synthetic fibers play a crucial role in modern society, impacting various aspects of daily life, industry, and the environment. ynthetic fibers are integral to modern life, offering a range of benefits from cost-effectiveness and versatility to innovative applications and performance characteristics. While they pose environmental challenges, ongoing research and development aim to create more sustainable and eco-friendly alternatives. Understanding the importance of synthetic fibers helps in appreciating their role in the economy, industry, and daily life, while also emphasizing the need for sustainable practices and innovation.
MARUTI SUZUKI- A Successful Joint Venture in India.pptx
- Background Paper 13 - A national partnership f
1. - Background Paper 13 -
A national partnership for acA national partnership for acA
national partnership for acA national partnership for action to
tion to tion to tion to
end health dend health dend health dend health disparities in the
United Statesisparities in the United Statesisparities in the
United Statesisparities in the United States
Mirtha R. Beadle 1
Garth N. Graham 1
Paul E. Jarris 2
Carlessia A. Hussein 3
Alan Morgan 4
Ron Finch 5
1 Office of Minority Health, U.S. Department of Health and
2. Human Services
2 Association of State and Territorial Health Officials; USA
3 National Association of State Offices of Minority Health;
USA
4 National Rural Health Association; USA
5 National Business Group on Health; USA
- Draft Background Paper 13 -
Disclaimer
WCSDH/BCKGRT/13/2011
3. This draft background paper is one of several in a series
commissioned by the World Health Organization for the
World Conference on Social Determinants of Health, held 19-21
October 2011, in Rio de Janeiro, Brazil. The goal
of these papers is to highlight country experiences on
implementing action on social determinants of health.
Copyright on these papers remains with the authors and/or the
Regional Office of the World Health Organization
from which they have been sourced. All rights reserved. The
findings, interpretations and conclusions expressed in
this paper are entirely those of the author(s) and should not be
attributed in any manner whatsoever to the World
Health Organization.
All papers are available at the symposium website at
www.who.int/sdhconference. Correspondence for the authors
can be sent by email to [email protected]
The designations employed and the presentation of the material
in this publication do not imply the expression of
any opinion whatsoever on the part of the World Health
Organization concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the
delimitation of its frontiers or boundaries. Dotted lines
on maps represent approximate border lines for which there may
not yet be full agreement. The mention of specific
4. companies or of certain manufacturers' products does not imply
that they are endorsed or recommended by the
World Health Organization in preference to others of a similar
nature that are not mentioned. Errors and omissions
excepted, the names of proprietary products are distinguished
by initial capital letters. The published material is
being distributed without warranty of any kind, either expressed
or implied. The responsibility for the interpretation
and use of the material lies with the reader. In no event shall the
World Health Organization be liable for damages
arising from its use.
- Draft Background Paper 13 -
1
Executive Summary
In its effort to achieve health equity, the United States joins
other countries that are also confronting
the problem of ending health disparities. Health equity is
attainment of the highest level of health for
all people. Achieving health equity requires valuing everyone
5. equally with focused and ongoing
societal efforts to address avoidable inequalities, historical and
contemporary injustices, and the
elimination of health and healthcare disparities.
Health disparities are persistent and pervasive in America,
affecting its racial and ethnic minorities,
other at-risk populations, and those of low socioeconomic and
educational status. The vision for a
healthier America was the force that brought together thousands
of community and government
leaders to develop the National Partnership for Action to End
Health Disparities (NPA). Although
efforts to address health equity began prior to the NPA, those
efforts were carried by specific
organizations and sectors (e.g., local health departments,
universities, health systems, philanthropy,
etc.).
Efforts to end health disparities are inherently a comprehensive
community and systems change
effort. The NPA is about change: why there should be change,
who should effect the change, and the
strategies that can be applied to implement change. The changes
needed to achieve health equity in
6. the United States can take place only with the cooperative effort
of individuals at all levels of public
and private enterprise. The NPA is the first national, multi -
sector, community- and partnership-driven
effort on behalf of health equity—with government leading the
way.
The development of the NPA was sponsored by the U.S.
Department of Health and Human Services
and its Office of Minority Health through a sequence of
activities that included regional meetings for
community and stakeholder leaders throughout the country, a
national public commentary period,
and numerous levels of review, analysis, and content refinement
by a range of experts. More than
2000 individuals participated on behalf of community- and
faith-based organizations; businesses;
healthcare and insurance industries; academia; city/county,
state, tribal, and federal governments;
and other sectors.
The NPA’s prime product, the National Stakeholder Strategy for
Achieving Health Equity, offers a set
of 20 community-driven strategies to end health disparities in
the United States and to achieve
7. - Draft Background Paper 13 -
2
health equity though collaboration and synergy. It was released
nationally on 8 April 2011
simultaneously with the HHS Action Plan to Reduce Racial and
Ethnic Health Disparities (represents
the federal commitment for health equity and a response to the
strategies recommended in the
National Stakeholder Strategy for Achieving Health Equity).
Together the two documents offer new
strategies and a mechanism for new partnerships aimed at
closing the health gap for the nation’s
racial, ethnic, and underserved communities.
Comprehensive change takes time, significant resources, and the
efforts of many partners. Beyond
financial and human capital, these efforts also require wide-
ranging coordination, transparency, and
commitment. The NPA is forging a new path for which there is
no prior roadmap. Although early in its
implementation, the NPA has already made a difference in the
way partners frame their work,
8. individually and collectively. Partners are beginning to use NPA
goals and, ultimately, these actions
translate into positive opportunities for communities. A key
lesson learned is that the NPA achieves a
momentum for change as it creates a national forum and
strategy for cooperation.
Problem
The United States is among the richest countries in the world,
yet disparities in health and
healthcare continue to exist for many of its vulnerable
populations. These persistent and pervasive
disparities carry a high societal burden in terms of the loss of
valuable resources (e.g., financial
capital, healthy children and families, workforce capacity and
capability, and social compassion).
Throughout its existence America has welcomed people of many
nations and cultures to its shores.
With this rich diversity comes a wide range of experience with
health and healthcare disparities.
Examples of these are outlined in Exhibit 1. These disparities
have been extensively documented
over time, most notably in the 1985 Report of the Secretary's
Task Force on Black and Minority
9. Health (an early and influential federal effort); the 2002
congressionally-mandated report on
healthcare disparities from the Institute of Medicine; the yearly
(since 2003) federal National
Healthcare Disparities Report and National Healthcare Quality
Report; and Healthy People 2020,
America’s master blueprint for health, among other sources.
Federal standards designate racial categories as White; African
American or Black; Asian; American
Indian or Alaska Native; and Native Hawaiian or Pacific
Islander; and ethnic categories as Hispanic
and non-Hispanic. However, these represent broad categories.
Statistically significant data are often
- Draft Background Paper 13 -
3
not available for the diversity of smaller subpopulations in the
United States. Grouping of data can
mask and significantly underestimate the health and healthcare
disparities that exist for
subpopulations. Underestimates of health or socioeconomic
10. status adversely affects awareness of
health disparities—with a corresponding lost opportunity to
focus on prevention, healthcare,
research, and other efforts. As a result, the populations affected
by inadequate or inaccurate data
collection continue to suffer from poorer health outcomes. It is
not only racial and ethnic minorities
that suffer from health-related disparities, but also other
underserved populations, such as those in
certain geographic areas, individuals with disabilities, LGBT
populations, and those of low
socioeconomic and educational status (see Exhibit 1).
The U.S. Department of Health and Human Services (HHS), the
public health system, the medical
care system, and the community of stakeholders have struggled
with the problem of health and
healthcare disparities for many years, in spite of their many
successes. New strategies for change
were needed and the climate for change was right. In particular:
Awareness continues to grow that
health disparities are a significant component of healthcare
costs. For example, the direct and
indirect costs of health inequalities and premature death were
estimated at $1.24 trillion between
11. 2003 and 2006. Addressing health disparities is an obvious
point of intervention that can provide
both financial and ethical payoffs. Minority populations are
increasing in number faster than the non-
Hispanic White population and are expected to comprise 40
percent of the population by the year
2030. The adverse economic and social impact of not addressing
health inequities for minorities
costs the loss of economic and human capital. There is a
growing constituency for change as
awareness increases concerning the social determinants of
health; the lack of improvement in
health status for minorities and underserved populations; and
the financial and social consequences
of health disparities. With awareness there has grown a body of
health equity stakeholders across all
sectors (federal, state, tribal, local, community, faith-based,
non-profit, private, academic, and
business) that support appropriate policies and actions. Ongoing
advances in technology provide a
favorable climate for change. For example, many public and
private agencies are able to collect,
analyze, store, and allow public access to massive amounts of
health-related data. The expanding
12. adoption of social networking technology across all sectors of
American society offers new
opportunities for promoting awareness of disease prevention
and health equity messages. In 2010
President Obama signed the Patient Protection and Affordable
Care Act, which enacted
comprehensive health insurance reforms and which, among
other requirements, contains provisions
- Draft Background Paper 13 -
4
to improve the federal infrastructure for addressing minority
health concerns, the diversity of the
healthcare workforce, and others that contribute to health
equity. The 2009 Health Information
Technology for Economic and Clinical Health Act mandates
comprehensive adoption of electronic
health records.
Exhibit 1: An Overview of Exhibit 1: An Overview of Exhibit 1:
An Overview of Exhibit 1: An Overview of Health Disparities
in the United StatesHealth Disparities in the United
13. StatesHealth Disparities in the United StatesHealth Disparities
in the United States
Examples of Populations Experiencing DisparitiesExamples of
Populations Experiencing DisparitiesExamples of Populations
Experiencing DisparitiesExamples of Populations Experiencing
Disparities
Racial/EthnicRacial/EthnicRacial/EthnicRacial/Ethnic
African American; Asian; American
Indian or Alaska Native; Native
Hawaiian or Pacific Islander;
Hispanic
AtAtAtAt----Risk PopulationsRisk PopulationsRisk
PopulationsRisk Populations
women, infants, children,
adolescents, elderly, people with
disabilities, rural and urban
populations, low literacy individuals,
LGBT populations
Social Social Social Social Determinants Determinants
Determinants Determinants
FactorsFactorsFactorsFactors
14. low socioeconomic status;
low educational attainment
Examples of WellExamples of WellExamples of WellExamples
of Well----documented and Prominent Disparitidocumented and
Prominent Disparitidocumented and Prominent
Disparitidocumented and Prominent Disparitieseseses
GeneralGeneralGeneralGeneral
SpecificSpecificSpecificSpecific1111
1Except as noted, data are from sources reported in the National
Stakeholder Strategy
Disparities in HealthDisparities in HealthDisparities in
HealthDisparities in Health
infant mortality
maternal mortality
cardiovascular disease
cancer
HIV/AIDS
• Black infants die at rates 2.4 times that of White infants.
• The maternal mortality rate for Blacks is 3 times that of
Whites;
15. and is nearly 6 times higher for women over 35 years compared
to those under 20 years of age.
• Compared to Whites, the incidence of HIV/AIDS is higher for
Blacks, Native Hawaiians and Pacific Islanders, and Hispanics
(8.9 times, 4.0 times, 3.4 times, respectively).
• Compared to the general population deaths from tuberculosis,
alcohol, motor vehicle accidents, and diabetes are higher for
- Draft Background Paper 13 -
5
diabetes
chronic lower respiratory
diseases
viral hepatitis
chronic liver disease and
cirrhosis
kidney disease
16. oral health
injury deaths
violence
mental health
substance abuse
other behavioral health disorders
American Indians and Alaska Natives (6 times, 6.1 times, 3.1
times, and 2.8 times, respectively).
• Compared to adults (35 and older), youths ages 18-25 are
more
than 4 times more likely to use illicit drugs and more than 2
times more likely to binge drink alcohol.
• Disabled persons, women, children, the elderly, the homeless,
and minorities disproportionately experience exposure to
violence. Disabled youths ages 12-19 experience violence at
nearly twice the rate as those without a disability.
• The poor are 2.5 times more likely to have untreated tooth
decay
than the not poor.
17. • Asians, Native Hawaiians, and Pacific Islanders account for
over
half of chronic Hepatitis B cases.
• Blacks, Asians, Pacific Islanders, and Hispanics have stomach
cancer mortality rates that are 1.5 times that of Whites. Cancer
is the leading cause of death for Asians and Pacific Islanders.
Disparities in Health CareDisparities in Health CareDisparities
in Health CareDisparities in Health Care2222
ability to access care
ability to obtain quality care
health insurance coverage
2These data are from the 2010
National Healthcare Disparities
Report
• Compared with residents of large city suburbs, residents of
rural
areas had worse care for about 40% of access measures and
30% of quality measures.
• Compared to non-Hispanic Whites, Hispanics had worse care
18. for
83% of access measures and 56% quality measures.
• Compared to high-income individuals, the poor had worse care
for 100% of access measures and 83% quality measures.
• The poor are 4.7 times more likely to not have health
insurance
than are those with high income.
• Although 25% of Americans live in rural areas, only 10% of
doctors practice in those settings.
- Draft Background Paper 13 -
6
HealthcHealthcHealthcHealthcare Workforce Disparitiesare
Workforce Disparitiesare Workforce Disparitiesare Workforce
Disparities
minority representation in the
healthcare workforce;
workforce shortages in
19. geographic locations;
availability of culturally and/or
linguistically competent providers
• Only 21% of medical school graduates plan to practice in
underserved areas.
• Hispanics represent about 15% of the population but comprise
only 5% of physicians, 5-7% of nursing, dental, and medical
school students, and 4% of medical school faculty.
• Blacks represent about 13% of the population but comprise
only
3.5% of physicians, 6-7% of dental and medical school students,
and 3% of medical school faculty.
Disparities in Data CollectionDisparities in Data
CollectionDisparities in Data CollectionDisparities in Data
Collection
inadequate collection of health
and healthcare metrics by race,
ethnicity, and primary language—
especially for population
subcategories and small
20. populations
• Mortality rates for American Indian and Alaska Native
populations have been underestimated due to the miscoding of
race on death certificates.
• U.S.-born African Americans, and Black immigrants from
Sub-
Saharan Africa, South America and the Caribbean may be
grouped together under the category of “Black.”
• Asians, Asian sub-groups, Native Hawaiians, and Pacific
Islanders may be grouped together under the category of
“Asian”
or “Asian/Pacific Islander.”
Examples of Significant U.S. Examples of Significant U.S.
Examples of Significant U.S. Examples of Significant U.S.
Publications that Address Disparities (including those
above)Publications that Address Disparities (including those
above)Publications that Address Disparities (including those
above)Publications that Address Disparities (including those
above)
The 1985 Report of the Secretary's Task Force on Black and
Minority Health, HHS; 2002 report from the
Institute of Medicine: Unequal Treatment: Confronting Racial
and Ethnic Disparities in Health; yearly
21. (since 2003) National Healthcare Disparities Report and
National Healthcare Quality Report from the
Agency for Healthcare Research and Quality, HHS; 2011 report
from the Centers for Disease Control and
Prevention, HHS: Health Disparities and Inequalities; Healthy
People 2020, HHS.
- Draft Background Paper 13 -
1
In order to close the health gap for the nation’s racial, ethnic,
and underserved communities in a climate
that was ripe for change, the federal Office of Minority Health
(OMH) within HHS sponsored the
development of the National Partnership for Action to End
Health Disparities (NPA). Its goal was to
mobilize and connect individuals and organizations from across
the country to create a nation in which
all people have an equal opportunity to reach their full health
potential. Given the broad range of
disparity populations and needs within the United States, it has
become increasingly clear that
22. government agencies and private constituencies working alone
within their own sectors are inadequate
for solving the problem of health disparities. The driving force
of the NPA is the conviction that a
nationally-based strategy is needed—one that relies on multiple
layers of partnerships across sectors in
order to leverage resources and talent. The NPA’s strategic
importance is based on its identity as a
public/private partnership that includes the combined efforts of
governments, academia, institutions,
businesses, humanitarian and faith-based organizations, and
individuals working across the entire
spectrum of public, private, community, and individual
enterprise. The NPA is designed to address a
wide breadth of inequities. However, it does so through a
common set of goals and strategies that all of
its stakeholders can adapt to their specific situations,
partnerships, and resources.
Context
As is common throughout the world, the social determinants
that primarily contribute to America’s
health disparities are poverty; racial/ethnic minority status; and
lack of education, economic
23. opportunity, and access to healthcare resources. These
determinants are often related to patterns of
social disadvantage or exclusion. Thus, the NPA defines health
disparityhealth disparityhealth disparityhealth disparity as a
particular type of health
difference that is closely linked with social or economic
disadvantage. Health disparities adversely
affect groups of people who have systematically experienced
greater social and/or economic obstacles
to health and/or a clean environment based on their racial or
ethnic group; religion; socioeconomic
status; gender; age; mental health; cognitive, sensory, or
physical disability; sexual orientation;
geographic location; or other characteristics historically linked
to discrimination or exclusion. The
primary groups which the NPA focuses on are racial and ethnic
minorities, geographic populations, the
disability community, and LGBT populations —within the
context of the populations and disparities noted
in Exhibit 1. These groups were chosen based on input from the
thousands of individuals that
participated in developing the NPA.
24. - Draft Background Paper 13 -
2
The NPA’s five central goalsNPA’s five central goalsNPA’s
five central goalsNPA’s five central goals are are are are: 1. 1.
1. 1. Increase awarenessawarenessawarenessawareness of the
significance of health disparities, their
impact on the nation, and the actions necessary to improve
health outcomes for racial, ethnic, and
underserved populations; 2. 2. 2. 2. Strengthen and broaden
leadershipleadershipleadershipleadership for addressing health
disparities at all
levels; 3. 3. 3. 3. Improve health and healthcare outcomeshealth
and healthcare outcomeshealth and healthcare outcomeshealth
and healthcare outcomes for racial, ethnic, and underserved
populations; 4. 4. 4. 4.
Improve cultural and linguistic competencycultural and
linguistic competencycultural and linguistic competencycultural
and linguistic competency and the diversity of the health-related
workforce; and 5. 5. 5. 5.
Improve datadatadatadata availability and coordination,
utilization, and diffusion of researchresearchresearchresearch
and evaluationevaluationevaluationevaluation
outcomes. Four crosscutting, fundamental principlesFour
crosscutting, fundamental principlesFour crosscutting,
25. fundamental principlesFour crosscutting, fundamental principles
are central to the NPA: leadership through
community engagementcommunity engagementcommunity
engagementcommunity engagement; the value of working via
partnershipspartnershipspartnershipspartnerships, the necessity
of cultural and lcultural and lcultural and lcultural and
linguistic inguistic inguistic inguistic
competencycompetencycompetencycompetency to meet the
needs of all communities, and the requirement of
nonnonnonnon----
discriminationdiscriminationdiscriminationdiscrimination in
actions,
services, leadership, and partnerships.
The formation of the NPA stands squarely within the context of
the democratic values of the United
States. That is, policies are established and action is taken with
input from public and private
stakeholders. Governments at all levels have a role in working
for the health and well being of its
citizenry; organizations have a role; states and citizens have
rights. In a matter as critical as advancing
health equity, the NPA offers a forum for sharing ideas and
resources, an opportunity for partnerships on
behalf of strategic action, and above all, a collaborative
approach to problem solving.
OMH sponsored the planning and development of the NPA.
26. However, a fundamental value of the NPA is its
lack of dependency on an influx of government spending. The
expectation is that OMH and other
government agencies will act as catalysts for change by
leveraging their existing partnerships and resources.
In this way they act as models for other NPA constituencies and
partners. Partnerships emphasize the
pooling and efficient use of resources, mobilization of talents,
and use of diverse approaches in order to
avoid duplication of efforts and fragmentation of services.
Partnerships promote sharing of human and
material resources, finances, and time in order to strategically
leverage funding and talent in an era of
scarcity and limitation.
Planning
The formation of the NPA was based on the voices of nearly
2,000 leaders who overwhelmingly
supported broadening the national dialogue about health
disparities from the more traditional disease-
focused approach to a more systems-oriented approach that
addresses crosscutting, multilevel issues.
These perspectives were gathered via a multi-year, multi-
layered, community-based process that was
27. - Draft Background Paper 13 -
3
sponsored by OMH. This process emphasized a "bottom up"
approach. The intent was to change the
paradigm of strategy development by vesting individuals—
particularly those at the front line of fighting
health disparities—with identifying and helping to shape core
actions for a coordinated national
response. Thus one of the earliest planning activities was a
series of countrywide regional
conversations, which included “community voices” meetings,
with representatives from minority groups
and organizations, American Indian and Alaska Native tribes,
community organizations, faith-based
organizations, health care providers and organizations, state and
local public health agencies and
organizations, academia and research, and health systems. The
process continued with increasing input
from groups representing policy makers, business, rural and
border health populations and others
28. interested in health equity. This included analysis, input, and
content refinement from a National
Visionary Panel of experts as well as a National Consensus
Meeting for late-stage review and refinement
of content. A Federal Interagency Health Equity Team
(FIHET)Federal Interagency Health Equity Team
(FIHET)Federal Interagency Health Equity Team
(FIHET)Federal Interagency Health Equity Team (FIHET) was
established to provide guidance. Its
members are representatives of HHS and the federal
departments of Agriculture, Commerce, Defense,
Education, Housing and Urban Development, Justice, Labor,
Transportation, and Veterans Affairs, as
well as from the Environmental Protection Agency and the
Consumer Products Safety Commission. The
process also included a six-week national public comment
period.
The NPA planning period culminated with the 8 April 2011
release of the National Stakeholder Strategy
for Achieving Health Equity (“National Stakeholder Strategy”),
which provides a detailed analysis of
health and healthcare disparities and 20 strategies for common
action, each of which aligns with one of
the five NPA goals. Each of the 20 strategies has a
corresponding set of objectives, measures, and
29. potential data sources that, in toto, offer a starting plan of
action that can be adapted to the needs and
resources of any organization or partnership working to reduce
health disparities.
In conjunction with the launch of the National Stakeholder
Strategy, HHS simultaneously released its
first ever HHS Action Plan to Reduce Racial and Ethnic Health
Disparities (“HHS Disparities Plan”),
which will be renewed annually. The HHS Disparities Plan is a
federal response to the National
Stakeholder Strategy and a pledge of the government’s
accountability in supporting health equity. With
it, HHS broadcasts its commitment to integrated approaches,
evidence-based programs, and strong and
visible national direction for leadership among public and
private partners on behalf of health equity.
The 2011 twin launch of these complementary community and
federal documents—and their ongoing
- Draft Background Paper 13 -
4
30. implementation among community stakeholders nationwide and
within HHS—mark the beginning of
widespread public/private cooperation and coordination aimed
at achieving health equity.
The NPA promotes and strengthens collaboration across
multiple sectors, and at federal, regional, state,
and community levels through three components: 1) the
National Stakeholder Strategy and related
documents such as the HHS Disparities Plan; 2) Specific
Blueprints for Action (aligned with the National
Stakeholder Strategy) for selected populations and for each of
10 geographic regions; and 3) targeted
initiatives that will be undertaken by partners across the public
and private sectors in support of the
NPA.
The policy tools and organizations that will move
implementation of the National Stakeholder Strategy
include the legislative mandates of the Affordable Care Act and
other laws; the longstanding relationship
between OMH and the state offices of minority health (SOMH);
the minority health-promoting
mechanisms that already exist throughout HHS and other
government departments; partnerships with
public health entities that facilitate the engagement and
31. education of policymakers at the state level
(e.g., the National Conference of State Legislatures, the
Association of State and Territorial Health
Officials, the National Association of State Offices of Minority
Health); partnerships with entities that
educate the business sector to embrace health equity as a
financially profitable policy (e.g., the National
Business Group on Health); and organizations which work to
improve the health and well-being of
geographic populations (e.g., the National Rural Health
Association).
Implementation
One of the most challenging steps in achieving any significant
goal is to move from ideas to action—from
planning to implementation. Thus, the existence of the NPA
does not in and of itself lead to the
achievement of its intended outcomes. Success will be
dependent upon the ability to implement and
assess progress for the National Stakeholder Strategy; the HHS
Disparities Plan and other related
federal documents; the Blueprints for Action; and the targeted
initiatives that will be undertaken by
partners across the public and private sectors. Implementation
has been a critical concern of the NPA.
32. An initial implementation framework has been developed by a
diverse group of stakeholders and was
refined through the NPA development process previously
described. It is grounded in the key concepts
of leadership, ownership, partnership, capacity, and
communication. Implementation will be
operationalized through voluntary multi-sector, multi-level
councils that provide leadership, ensure
- Draft Background Paper 13 -
5
continued information flow, and galvanize action at the federal,
national, regional, state, tribal, and local
levels.
A communications plan A communications plan A
communications plan A communications plan is a key
component of implementation and evaluation. The NPA
communication
plan focuses on (1) increasing awareness among key audiences
of the significance of health disparities,
their impact on the nation, and the actions necessary to achieve
33. health equity; (2) helping partners
promote and address the goals by making them a priority, and
by sharing information within their
individual networks to broaden diffusion of information; (3)
ensuring cohesion in all communications
and coordination between and among the multi-sector, multi-
level councils and their partners, and
fostering effective communication and sharing of information
by creating dynamic feedback loops
between the councils to share relevant activities, policies,
emerging issues, priorities, and
evaluation/best practices.
NPA implementation is supported in part by OMH and several
contracts managed by OMH to assist with
coordinating, monitoring, and sustaining the NPA. Support
includes assistance with:
•
ImplementationImplementationImplementationImplementation
—coordinating and facilitating council meetings, consulting
with leaders and
experts, engaging communities, developing content for
Blueprints for Action, producing tools and
materials, working with partners to ensure connection and
integration with implementation actions
34. or plans, building partnerships, and providing implementation
capacity building support.
•
CommunicationsCommunicationsCommunicationsCommunicatio
ns—crafting and integrating NPA messages for various
audiences, developing
communication tools, and helping disseminate NPA information
to key audiences in various
formats as a means for sharing knowledge about activities,
emerging issues, priorities, and
evaluation/best practices.
• EvaluationEvaluationEvaluationEvaluation—managing and
monitoring evaluation activities to ensure that partners connect
and
contribute to the NPA evaluation; providing capacity building
support to communities; and
negotiating data use and reporting with agencies who manage
data systems relevant to the NPA.
Initial implementation will roll out in stages. Phase IPhase
IPhase IPhase I involves the activities of the FIHET, FIHET
subcommittees, and National Partners. Phase IIPhase IIPhase
IIPhase II involves the activities of Regional Health Equity
Councils, state offices of minority health, and expanded
national partnerships with businesses and other
communities. Phase IIIPhase IIIPhase IIIPhase III involves
35. targeted multi-agency initiatives to minimize duplication and
increase
effectiveness. Current NPA implementation activities include
the following:
- Draft Background Paper 13 -
6
Phase1Phase1Phase1Phase1––––FIHETFIHETFIHETFIHET
includes representation from 12 federal agencies as described
above. The purpose of
FIHET is to (1) identify opportunities for federal collaboration,
partnership, coordination, and/or action
on efforts that are relevant to the NPA; and (2) provide
leadership and guidance for national, regional,
state, and local efforts that address health equity. The FIHET
played a critical role in providing feedback
on the NPA’s development. Moving into the implementation
phase, FIHET has established five
subcommittees to develop implementation recommendations
linked to the five NPA goals. Each
subcommittee has developed work plans outlining its priorities,
36. associated strategies that connect the
work of federal agencies, action steps; as well as timelines and
intended outcomes for each priority.
Phase1Phase1Phase1Phase1––––National PartnersNational
PartnersNational PartnersNational Partners work with the NPA
to leverage resources, expand its reach and spheres of
influence, infuse NPA goals and strategies into organizational
policies and practices, and share stories
and successes with their broad constituencies. National partners
will include community- and faith-
based organizations, professional societies, government
agencies, national non-profit organizations,
advocacy groups, foundations, corporations, businesses of all
sizes, industry groups, and colleges and
universities. For example,
• The National Conference of State Legislatures (NCSL) The
National Conference of State Legislatures (NCSL) The National
Conference of State Legislatures (NCSL) The National
Conference of State Legislatures (NCSL) is a bipartisan
organization that serves the
legislators and legislative staff of the nation's 50 states, its
commonwealths and territories. NCSL
works with OMH to help state legislators understand issues
related to health disparities and how
37. specific policies either narrow or widen disparities in health
care for racial and ethnic minorities.
• The Association of State and Territorial HeThe Association of
State and Territorial HeThe Association of State and Territorial
HeThe Association of State and Territorial Health Officials
(ASTHO) alth Officials (ASTHO) alth Officials (ASTHO) alth
Officials (ASTHO) recognizes that progress in
improving the health of minority populations will require that
states have access to information on
effective practices as well as resources to assist in the
implementation of effective public health
policies and programs. ASTHO aims to fill these knowledge
gaps, strengthen state leadership, and
improve health disparities efforts through various activities
under the NPA.
• The National Association of State Offices of Minority Health
(NASOMH)The National Association of State Offices of
Minority Health (NASOMH)The National Association of State
Offices of Minority Health (NASOMH)The National
Association of State Offices of Minority Health (NASOMH)
promotes and protects the
health of communities of color, and tribal organizations and
nations. Its NPA activities include
technical assistance for SOMHs in engaging communities on
NPA actions, building awareness, and
incorporating or aligning state health disparity and/or health
equity plans with NPA goals.
38. - Draft Background Paper 13 -
7
• National Business Group on Health (NBGH)National Business
Group on Health (NBGH)National Business Group on Health
(NBGH)National Business Group on Health (NBGH) is a
national, nonprofit devoted exclusively to finding
innovative and forward-thinking business solutions to the
nation’s most important healthcare
challenges. As a NPA partner, NBGH is working to make the
case to employers that addressing
health disparities is a good financial and business decision.
• The The The The National Rural Health AssociationNational
Rural Health AssociationNational Rural Health
AssociationNational Rural Health Association (NRHA) (NRHA)
(NRHA) (NRHA) is a national nonprofit that provides
leadership on
rural health issues. Its role in the NPA is as a bridge connecting
minority and rural health
constituencies and needs, building awareness, and addressing
actions for border populations.
Phase IIPhase IIPhase IIPhase II————10 Regional Health
39. Equity Councils10 Regional Health Equity Councils10 Regional
Health Equity Councils10 Regional Health Equity Councils are
being launched that will focus on groups of states
nationwide. Initial planning meetings were held in four
geographic regions prior to the launch of the NPA.
The councils will address health disparity improvement actions
for their geographic areas and work to
leverage resources, infuse NPA goals and strategies into
policies and practices, and share stories and
successes with broad constituencies. The councils include
individuals from the public, nonprofit, and
private sectors and they represent communities experiencing
health disparities; state and local
government agencies; tribes and tribal organizations; healthcare
providers and systems; health plans;
businesses; academic and research institutions; foundations; and
other organizations who focus on
specific determinants of health (e.g., environmental justice,
housing, transportation, education, etc.).
Phase IIPhase IIPhase IIPhase II————State Offices of
Minority Health (SOMH) State Offices of Minority Health
(SOMH) State Offices of Minority Health (SOMH) State Offices
of Minority Health (SOMH) are actively engaging communities
through periodic
meetings; developing strategic partnerships, mobilizing
networks; improving awareness and
40. communications through different media outlets; and leading
states’ efforts in updating health disparity
or health equity plans so that they align with the NPA. The
SOMHs come together during monthly
conference calls to update each other on progress, address
challenges, share lessons learned, and
consider collective actions.
Evaluation
The NPA Evaluation Plan provides a roadmap for determining
the effectiveness of NPA strategies and
actions. It describes the overall approach, key indicators and
measures, data sources, and potential
data collection methods. The goal of the evaluation is to ensure
the integration and penetration of NPA
efforts across sectors (e.g., education, housing, environmental
health) and across levels (i.e., federal,
national, regional, state, tribal, and community). A logic model
was created by a team of expert advisors
to illustrate the implementation pathway and anticipated
outcomes of the NPA. The model is based on
- Draft Background Paper 13 -
41. 8
the assumption that observable changes in the way public and
private organizations work across sectors
to address the social determinants of health are more likely to
occur initially than are observable
population-level outcomes. Therefore, the initial focus for
evaluation is to determine whether (1)
organizational and structural changes have actually been made
on behalf of health equity; (2) specific
actions have been taken that align with the NPA’s five goals
and 20 strategies; (3) public awareness and
understanding about social determinants has increased; (4)
policy, systems, and other multi-level
changes have been initiated; (5) there is an increase in
communities’ capacities to address health
disparities through the use of data for decisionmaking; and (6)
whether promising practices can be
identified. Evaluations will also consider the feasibility of
developing and using a social determinants
health equity index to assess how well the nation is progressing
towards improved health outcomes.
42. Even with an optimal social determinants index, it will take
several years before observable changes can
be expected.
The evaluation plan has identified initial optimal indicators and
measures. Some of these measures are
already available; others will need to be developed. To the
degree possible, evaluation teams will
coordinate NPA evaluations with those of other federal entities
and with NPA partners in order to
minimize duplication and to build on existing data analyses and
sources. Evaluation teams will work with
OMH leadership to facilitate the development of data-sharing
agreements and protocols. Current
proposed indicators are as follows:
43. - Draft Background Paper 13 -
9
Exhibit 2: Current Proposed Evaluation IndicatorsExhibit 2:
Current Proposed Evaluation IndicatorsExhibit 2: Current
Proposed Evaluation IndicatorsExhibit 2: Current Proposed
Evaluation Indicators
Infrastructure and Partnerships
Productive and effective health equity councils, including the
Federal Interagency Health Equity
Team and the national, regional, state, tribal and community
health equity councils
Productive and effective NPA Partnerships (e.g., Association of
State and Territorial Health Officials,
National Conference of State Legislatures, National Business
Group on Health, National Association
of State Offices of Minority Health)
Vertical (e.g., between state and region) and horizontal (e.g.,
among states or regions) alignment
among national, regional, state, tribal, and local efforts
Actions
Multi-sector and multi-level actions
Goal attainment
44. Alignment between actions and results
Capacity for implementing strategies to end health disparities
Public Awareness and Understanding
Awareness of NPA
Awareness of health disparities and understanding of social
determinants
News coverage from print, broadcast, and internet news sources
on health-related issues affecting
underserved and racial and ethnic communities (including
mainstream and selected racial and
ethnic print news sources)
Policy, Systems, and Other MultiPolicy, Systems, and Other
MultiPolicy, Systems, and Other MultiPolicy, Systems, and
Other Multi----level Changelevel Changelevel Changelevel
Changessss
Influence of NPA on its partners
Inclusion of health disparities or health equity concepts and
language (e.g., social determinants) in
mainstream institutions and among broad leadership
Influence of NPA on local, state, and national healthcare-related
policies
Influence of NPA on local, state, and national policies,
procedures, and practices that address the
social determinants of health
45. - Draft Background Paper 13 -
10
Evaluators will select a final list of indicators and measures, as
well as the sample of regions, states,
and organizations that will be included in the initial evaluation.
In general, data collection activities can
be summarized into the following types:
• Surveys of the FIHET, Regional Health Equity Councils, and
NPA partners;
• Review and analysis of the goals and strategies implemented
by the FIHET, Regional Health
Equity Councils, and NPA partners;
• Content analysis of NPA partners’ programs, agendas,
materials, plans, etc.;
• Interviews with key informants at the federal and national
levels and in the regions, states, and
tribes that are part of the sample.
46. Cross-case study method will be used to analyze the data. This
method allows for comparisons across
and within selected regions, states, and communities, as well as
the combined use of qualitative and
quantitative methods. The findings will be compiled into case
studies. Each case study will tell the story
of what transpired in each of the sample geographic units and
will provide insight into the context and
circumstances under which changes did or did not take place.
Each case study will, in turn, contribute to
a national, in-depth case study on the NPA’s effectiveness.
Time-series presentations of data will also be
conducted in order to show changes.
The evaluation team will submit semiannual reports on its
progress, and annual reports that will
contribute to the OMH reports to the U.S. Congress. Annual
reports will also be provided to the FIHET,
Regional Health Equity Councils, NPA partners, and the
implementation and communications teams.
Reports will be posted on the NPA website and made available
and accessible to the public. The
evaluation team will facilitate a meeting to reflect and discuss
the findings with OMH leadership and
47. staff, the implementation teams, and the communications teams.
Meetings will focus on the lessons
learned and the implications for iterative strategy improvement
and implementation.
Follow-up and lessons learned
Efforts to end health disparities are inherently a comprehensive
community and systems change effort.
The NPA is about change: why there should be change, who
should effect the change, and the strategies
- Draft Background Paper 13 -
11
that can be applied to implement change. The changes needed
can take place only with the cooperative
effort of individuals at all levels of public and private
enterprise.
Managing and coordinating the magnitude of planning and
implementation activities has been one of
the greatest challenges of the NPA. That challenge continues as
the NPA deliberately plans for further
growth with phased and monitored expansion of the number of
48. NPA partners and activities. Past
experiences in driving a health equity agenda underscore the
lesson that comprehensive efforts take
time, significant resources, and the efforts of many partners.
Beyond financial and human capital, these
efforts also require significant coordination, transparency, and
commitment. The growth of the U.S.
knowledge base, constituency, and programs for health equity in
the past few decades has formed the
foundation necessary to initiate and sustain the NPA.
Individuals across sectors have committed to
participate in NPA activities because of their passion and
commitment to its vision and goals.
The NPA represents a grassroots effort to form strategic
partnerships and engage communities and
organizations on behalf of health equity. As a grassroots effort,
all partners have had to “own” the NPA
in order for it to survive and thrive. Continued progress is
dependent on success in transforming the
quality and commitment of stakeholder partnerships. Ideally,
individuals and organizations will expand
their sharing of resources and spheres of cooperation beyond
customary relationships to include
partners that can enhance mission capacity and value in new and
49. effective ways. The holistic approach
of the NPA to integrate implementation, communication and
evaluation activities supports participants
as they unite to prioritize common goals, share successful
strategies, and move from planning to action.
The objective is to advance implementation, communication and
evaluation at a pace that maintains
their coordination and alignment while also maintaining the
engagement of all stakeholders.
The NPA is forging a new path for which there is no prior
roadmap. Lessons are learned as actions are
planned and executed. Partners and experts are continually
encouraged to address new and emerging
opportunities. An important lesson has been that an
understanding of the social determinants of health
does not in itself bring expertise for creating change or forming
new relationships and partnerships.
Thus, capacity-building opportunities and tools (e.g.,
educational webinars, targeted messages, and
access to experts for consultation, etc.) to facilitate effective
participation are being developed.
Although early in its implementation, the NPA has already made
a difference in the way partners frame
their work, individually and collectively. There is evidence that
50. FIHET member agencies are beginning to
- Draft Background Paper 13 -
12
use the NPA goals to develop priorities and scope of activities,
which translates into positive
opportunities for communities. In addition, FIHET members
have consistently engaged and recruited
others to join the NPA. Elsewhere there has been an emerging
pattern among organizations to work
collaboratively and strategically toward common goals. NPA
partners are increasing their knowledge
about disparities, public/private sector infrastructure and
resources for addressing disparities, and how
health equity efforts can and should be integrated into the
broader national dialogue. A key lesson
learned is that the NPA achieves a momentum for change as it
creates a national forum and strategy for
cooperation.
51. - Draft Background Paper 13 -
www.who.int/social_determinants/www.who.int/social_determin
ants/www.who.int/social_determinants/www.who.int/social_det
erminants/