Download as PDF, PPTX

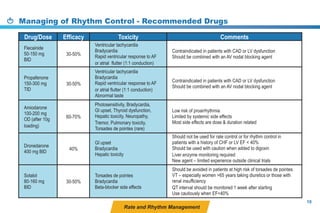

This document provides a summary of the CCS AF guidelines from 2010 to present. It includes diagnostic and treatment recommendations for atrial fibrillation management. The recommendations are intended to provide a practical clinical approach but are not a substitute for clinical judgment. Adherence to the guidelines will not necessarily produce successful outcomes in every case.

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





