Bronchial Asthma
Asthmais a syndrome characterized by airflow obstruction
that varies markedly, both spontaneously and with
treatment.
Asthmatics harbor a special type of inflammation in the
airways that makes them more responsive than non
asthmatics to a wide range of triggers, leading to excessive
narrowing with consequent reduced airflow and
symptomatic wheezing and dyspnea.
Narrowing of the airways is usually reversible, but in some
patients with chronic asthma there may be an element of
irreversible airflow obstruction.
3.
Cont…
In developingcountries there is a rising prevalence,
which is associated with increased urbanization.
The prevalence of atopy and other allergic diseases
has also increased over the same time, suggesting that
the reasons for the increase are likely to be systemic
rather than confined to the lungs.
Most patients with asthma in affluent countries are
atopic, with allergic sensitization to the house dust mite,
and other environmental allergens, such as animal fur
and pollens.
4.
Cont…
Asthma canpresent at any age, with a peak age of 3
years.
Long-term studies that have followed children until they
reach the age of 40 years suggest that many with
asthma become asymptomatic during adolescence but
that asthma returns in some during adult life, particularly
in those with persistent symptoms and severe asthma.
Adults with asthma, including those with onset during
adulthood, rarely become permanently
asymptomatic.
5.
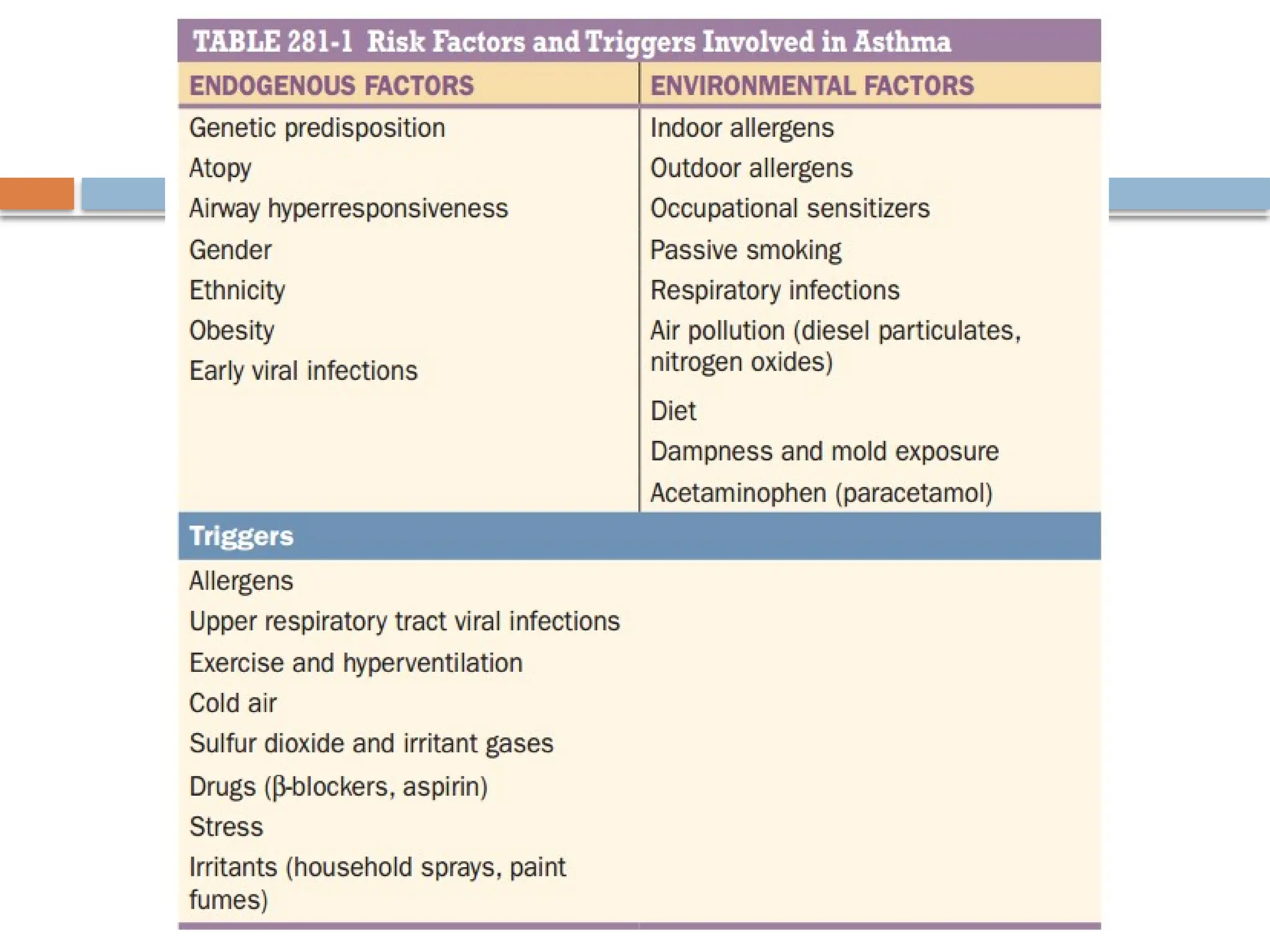
Risk factors andtriggers
Asthma is a heterogeneous disease with interplay
between genetic and environmental factors.
Several risk factors that predispose to asthma have
been identified.
These should be distinguished from triggers, which
are environmental factors that worsen asthma in a
patient with established asthma
7.
Atopy
Atopy isthe major risk factor for asthma, and non-atopic
individuals have a very low risk of developing asthma.
Patients with asthma commonly suffer from other atopic
diseases, particularly allergic rhinitis, which may be found
in >80% of asthmatic patients, and atopic dermatitis
(eczema).
Asthma is associated with a specific chronic inflammation of
the mucosa of the lower airways and obstruction of this air
ways due to constriction.
One of the main aims of treatment is to reduce this
inflammation.
8.
Pathophysiology of Asthma
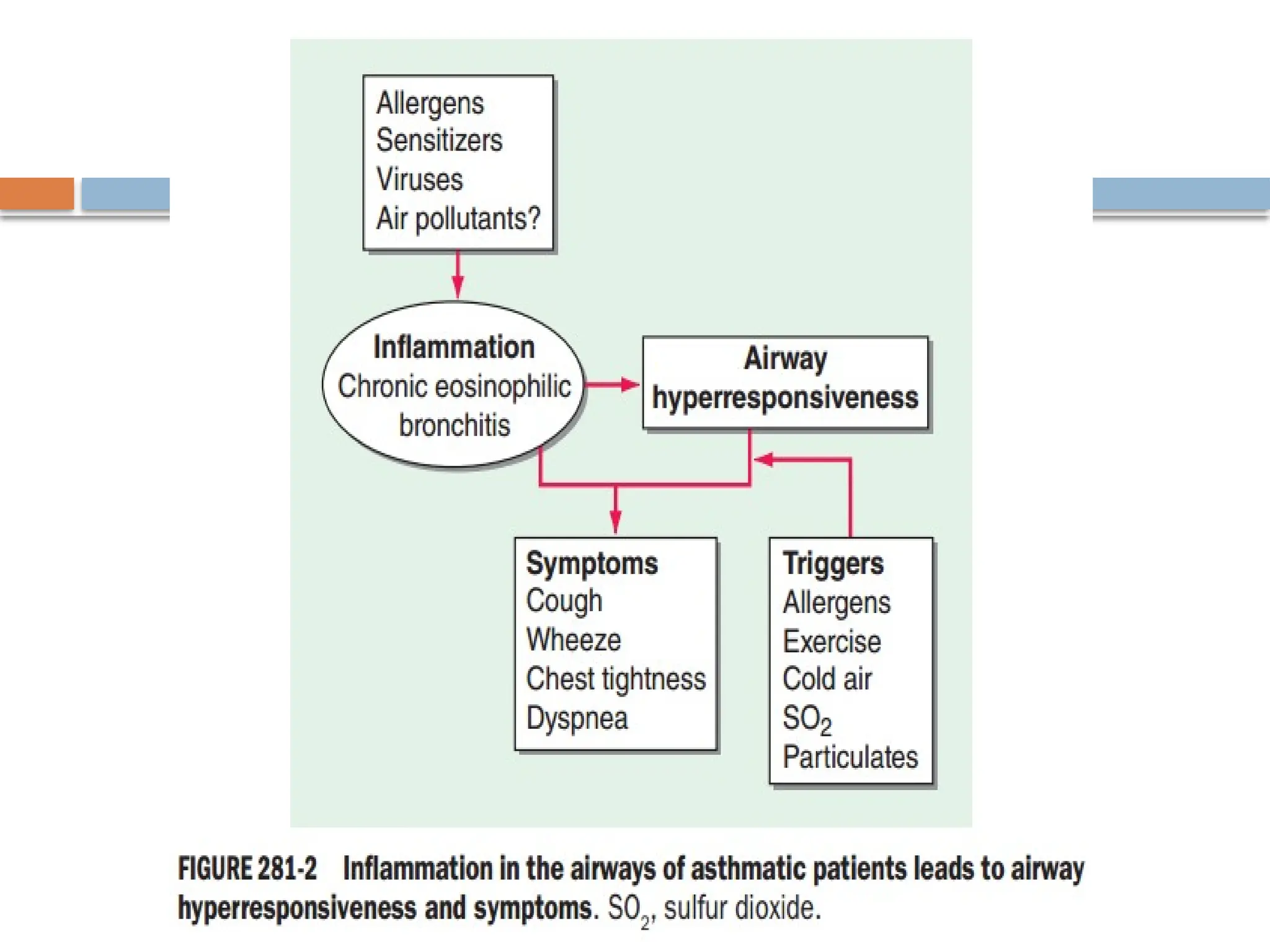
AirwayInflammation
There is inflammation in the respiratory mucosa from the
trachea to terminal bronchioles, but with a predominance in
the bronchi (cartilaginous airways), but it is still uncertain
how inflammatory cells interact and how inflammation
translates into the symptoms of asthma.
There is good evidence that the specific pattern of airway
inflammation in asthma is associated with airway
hyperresponsiveness (AHR), the physiologic abnormality
of asthma, which is correlated with variable airflow
obstruction.
9.
Cont…
Superimposed onthis chronic inflammatory state
are acute inflammatory episodes, which correspond
to exacerbations of asthma.
Although the common pattern of inflammation in
asthma is characterized by eosinophil infiltration,
other inflammatory cells liks mast cells,
macrophages, lymphocytes and dendritic cells
are also isolated.
11.
Cont…
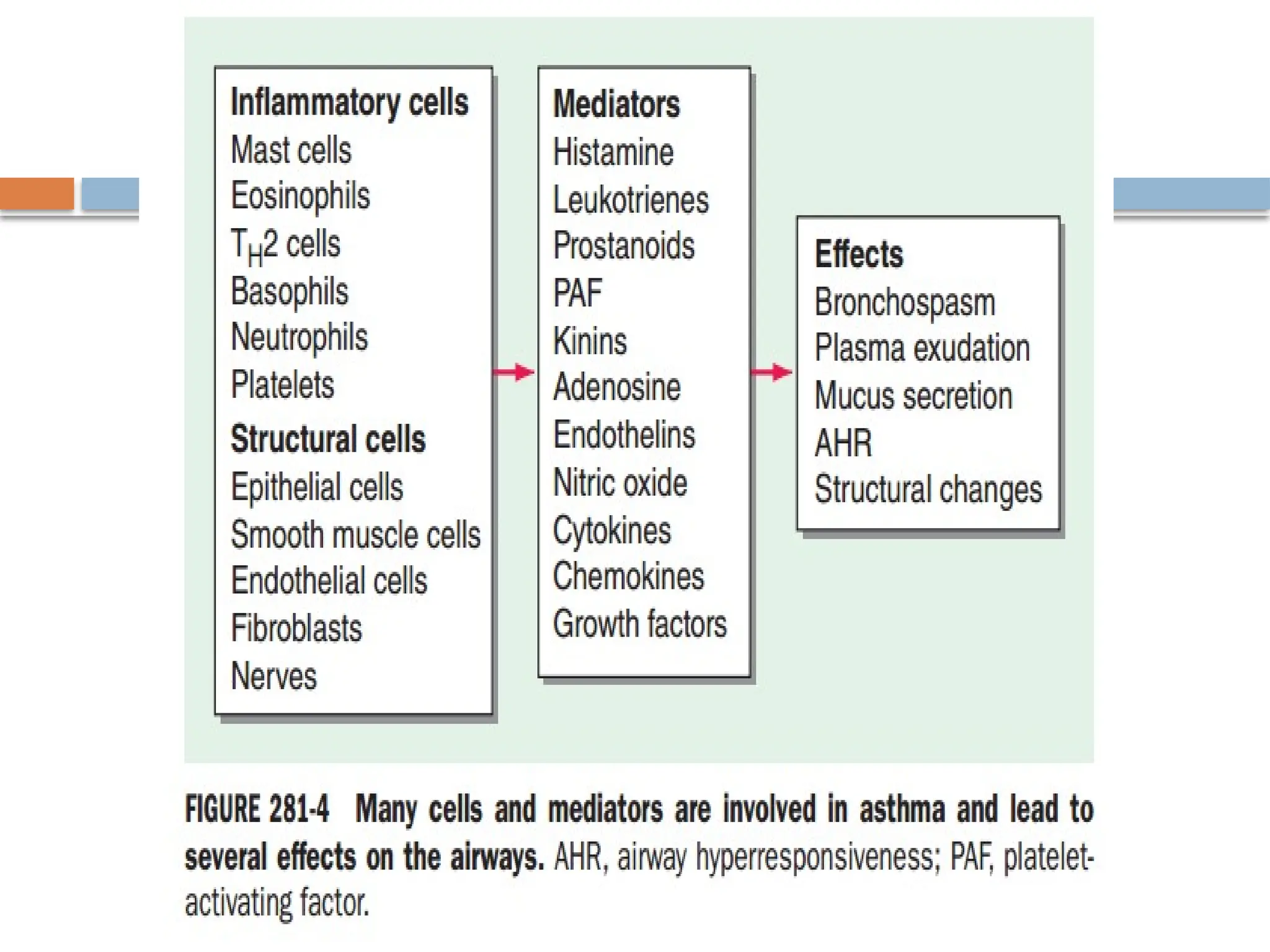
Inflammatory Mediators
Multipleinflammatory mediators have been implicated
in asthma, and they may have a variety of effects on
the airways that account for the pathologic features of
asthma.
Mast cell-derived mediators, such as histamine,
prostaglandin D2, and cysteinyl-leukotrienes,
contract airway smooth muscle, increase microvascular
leakage, increase airway mucus secretion, and attract
other inflammatory cells.
13.
Cont…
Airway Hyperresponsiveness (AHR)
AHR is the characteristic physiologic abnormality of asthma and
describes the excessive bronchoconstrictor response to multiple
inhaled triggers that would have no effect on normal airways.
The increase in AHR is linked to the frequency of asthma
symptoms, and, thus, an important aim of therapy is to reduce
AHR.
Increased bronchoconstrictor responsiveness is seen with direct
bronchoconstrictors such as histamine and methacholine, which
contract airway smooth muscle, but is characteristically also seen
with many indirect stimuli, which release bronchoconstrictors from
mast cells or activate sensory nerves.
14.
Clinical Features
Thecharacteristic symptoms of asthma are wheezing,
dyspnea, and coughing, which are variable, both
spontaneously and with therapy.
Symptoms may be worse at night and patients
typically awake in the early morning hours.
Patients may report difficulty in filling their lungs with
air.
There is increased mucus production in some patients,
with typically tenacious mucus that is difficult to
expectorate.
15.
Cont…
There maybe increased ventilation and use of accessory muscles of
ventilation.
Prodromal symptoms may precede an attack, with itching under
the chin, discomfort between the scapulae, or inexplicable fear
(impending doom).
Typical physical signs are inspiratory, and to a greater extent
expiratory, rhonchi/wheeze throughout the chest, and there may
be hyperinflation.
Some patients, particularly children, may present with a
predominant nonproductive cough (“cough-variant asthma”).
There may be no abnormal physical findings when asthma is under
control.
16.
Exacerbation of AcuteSevere Asthma.
These findings are indicators of Acute severe Asthma.
Tachycardia > 120 beats/min and or tachypnea > 30/min.
Use of accessory muscles of respiration.
Hypotension.
Inability to finish one sentence in one breath.
Silent chest.
Confusion or loss of consciousness.
Hypoxemia ((arterial partial pressure of oxygen [PaO2] <60 mmHg [8
kPa], pulse oxygen saturation [SpO2] <90 percent)
Pulsus Paradoxus ((ie, a fall in systolic blood pressure by at least 10
mmHg during inspiration)
PEF < 50% predicted or personal best.
Diagnosis of Asthma
The diagnosis of asthma is usually apparent from
the clinical symptoms of variable and intermittent
airways obstruction, but must be confirmed by
objective measurements of lung function.
.
19.
Cont…
Lung Function Tests
Simple spirometry confirms airflow limitation with a
reduced FEV1, FEV1/FVC ratio, and PEF.
Reversibility is demonstrated by a >12% and 200-
mL increase in FEV115 min after an inhaled short-
acting 2-agonist (SABA; such as inhaled albuterol
β
400 g) or in some patients by a 2–4 week trial of
μ
oral corticosteroids (OCS) (prednisone or
prednisolone 30–40 mg daily).
20.
Cont…
The levelof reversibility in COPD patients is less
than 12% or 200ml after the above medications
and this is how it is differentiated from Asthma.
Imaging Chest roentgenography is usually normal
but in more severe patients may show
hyperinflated lungs.
In exacerbations, there may be evidence of a
pneumothorax
21.
Treatment of Asthma
The main drugs for asthma can be divided into
bronchodilators, which give rapid relief of
symptoms mainly through relaxation of airway
smooth muscle, and controllers (steroids) which
inhibit the underlying inflammatory process.
22.
Cont…
Bronchodilator therapy.
Bronchodilatorsact primarily on airway smooth muscle to
reverse the bronchoconstriction of asthma.
This gives rapid relief of symptoms but has little or no effect
on the underlying inflammatory process.
Thus, bronchodilators are not sufficient to control asthma in
patients with persistent symptoms.
There are three classes of bronchodilators in current use:
2-adrenergic agonists
β , anticholinergics, and Theophylline.
of these, 2-agonists
β are by far the most effective
23.
Cont…
2-Agonists areusually given by inhalation to reduce
β
side effects.
SABA, such as albuterol and terbutaline, have a duration
of action of 3–6 h.
They have a rapid onset of bronchodilatation and are,
therefore, used as needed for symptom relief (relievers).
Increased use of SABA indicates that asthma is not
controlled.
SABA are used in high doses by nebulizer or via a
metered-dose inhaler (MDI) with a spacer.
24.
Long-acting 2-agonists(LABA
β ) include salmeterol
and formoterol, both of which have a duration of
action over 12 h and are given twice daily by
inhalation; and indacaterol, olodaterol, and
vilanterol, which are given once daily.
LABA have replaced the regular use of SABA, but
LABA should not be given in the absence of ICS
therapy as they do not control the underlying
inflammation.
25.
Cont…
They do,however, improve asthma control and reduce
exacerbations when added to ICS, which allows asthma to be
managed with lower doses of corticosteroids.
This observation has led to the widespread use of fixed
combination inhalers that contain a corticosteroid and a
LABA, which have proved to be highly effective in the control
of asthma and prevention of exacerbations.
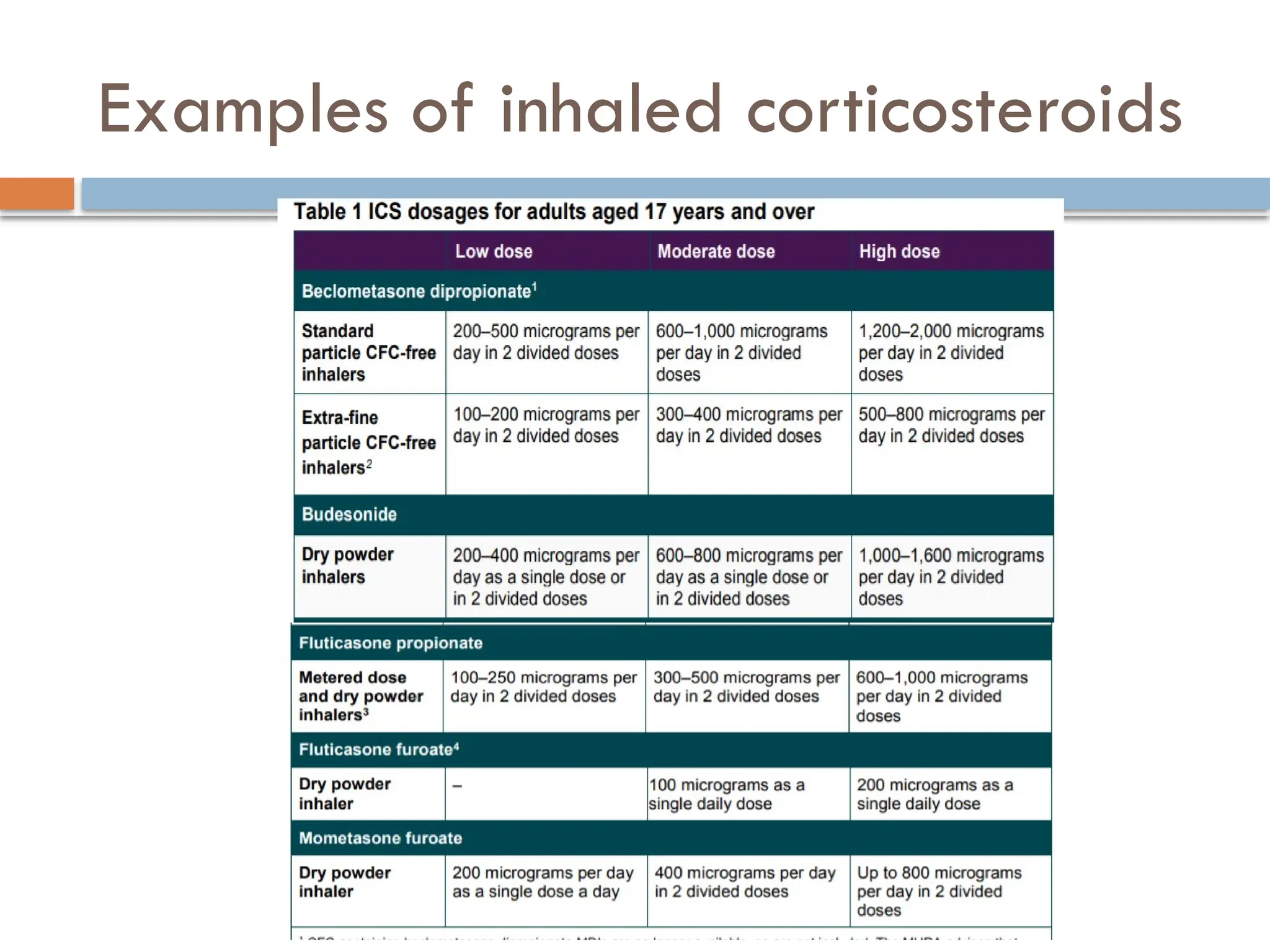
Controller Therapies
Inhaled Corticosteroids (ICS) are by far the most effective
controllers for asthma, and their early use has revolutionized
asthma therapy.
26.
Cont…
ICS areby far the most effective controllers in the management of
asthma and are beneficial in treating asthma of any severity and
age.
ICS are usually given twice daily, but some may be effective
once daily in mildly symptomatic patients.
ICS rapidly improve the symptoms of asthma, and lung function
improves over several days.
They are effective in preventing asthma symptoms, such as EIA and
nocturnal exacerbations, but also prevent severe exacerbations.
ICS reduce AHR, but maximal improvement may take several
months of therapy.
27.
Cont…
Early treatmentwith ICS appears to prevent irreversible
changes in airway function that occur with chronic asthma.
Withdrawal of ICS results in slow deterioration of asthma
control, indicating that they suppress inflammation and
symptoms, but do not cure the underlying condition.
ICS are now given as first-line therapy for patients with
persistent asthma, but if they do not control symptoms at low
doses, it is usual to add a LABA as a next step.
Local side effects include hoarseness (dysphonia) and oral
candidiasis, which may be reduced with the use of a large
volume spacer device mouth gurgle after use.
28.
Cont…
Systemic Corticosteroids
Corticosteroidsare used intravenously (hydrocortisone or
methylprednisolone) for the treatment of acute severe asthma,
although several studies now show that OCS are as effective
and easier to administer.
A course of OCS (usually prednisone or prednisolone 30–45
mg once daily for 5–10 days) is used to treat acute
exacerbations of asthma; no tapering of the dose is needed.
Approximately 1% of asthma patients may require
maintenance treatment with OCS; the lowest dose necessary
to maintain control needs to be determined.
29.
Management of Exacerbationof Acute Severe
Asthma.
The primary goals of therapy for acute severe
asthma are the rapid reversal of airflow limitation
and the correction, if necessary, of hypercapnia or
hypoxemia.
Airflow limitation is most rapidly alleviated by the
combination of repeated administration of inhaled
bronchodilators and early institution of systemic
glucocorticoids.
30.
Cont…
Oxygen
Supplemental oxygenshould be administered to most patients
with a moderate or severe asthma exacerbation, particularly
those who are hypoxemic (SpO2 <90 percent) or for whom
continuous oxygen saturation monitoring is not available.
Inhaled beta agonists
The mainstay of bronchodilator treatment is inhalation of
short-acting beta-2-selective adrenergic agonists (SABA), such
as albuterol (Salbutamol), levalbuterol, or fenoterol.
Only Albuterol(salbutamol) in Ethiopia.
31.
Cont…
Standard nebulization– Albuterol 2.5 to 5 mg by jet (also called
"hand-held" or "updraft") nebulization every 20 minutes for three
doses, then 2.5 mg to 5 mg every one to four hours as needed.
Metered dose inhaler (MDI) – Albuterol by MDI with a spacer or
valved-holding chamber device four to eight puffs every 20
minutes, for the first hour.
Most patients can then transition to dosing every one to four
hours, and rarely require dosing at more frequent intervals.
Continuous nebulization – In the intensive care unit, some
clinicians use a special apparatus to achieve continuous
nebulization, administering 10 to 15 mg over one hour .
32.
Cont…
Standard nebulization– Albuterol 2.5 to 5 mg by jet (also called
"hand-held" or "updraft") nebulization every 20 minutes for three
doses, then 2.5 mg to 5 mg every one to four hours as needed.
Metered dose inhaler (MDI) – Albuterol by MDI with a spacer or
valved-holding chamber device four to eight puffs every 20
minutes, for the first hour.
Most patients can then transition to dosing every one to four
hours, and rarely require dosing at more frequent intervals.
Continuous nebulization – In the intensive care unit, some
clinicians use a special apparatus to achieve continuous
nebulization, administering 10 to 15 mg over one hour .
33.
Cont…
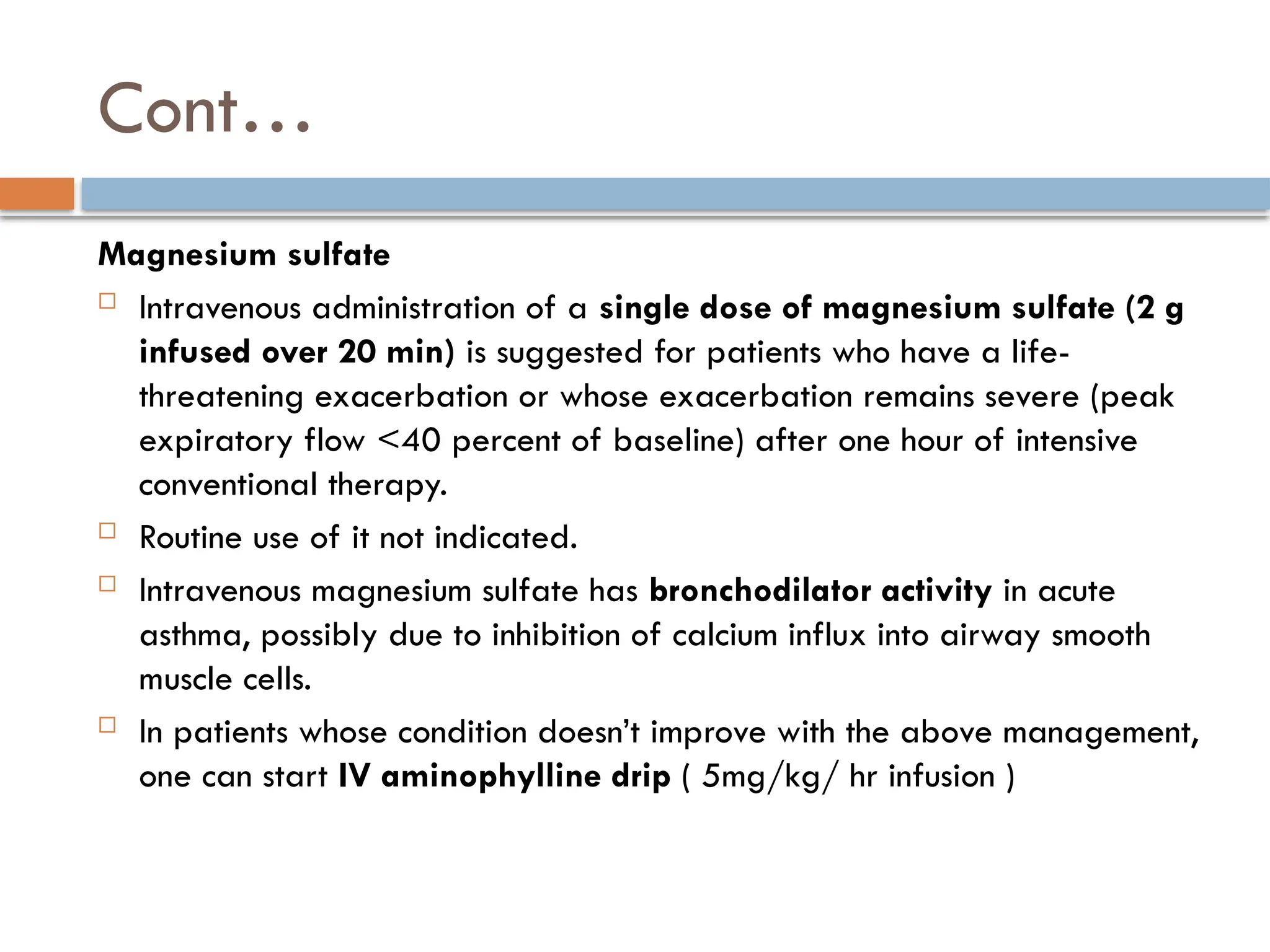
Magnesium sulfate
Intravenousadministration of a single dose of magnesium sulfate (2 g
infused over 20 min) is suggested for patients who have a life-
threatening exacerbation or whose exacerbation remains severe (peak
expiratory flow <40 percent of baseline) after one hour of intensive
conventional therapy.
Routine use of it not indicated.
Intravenous magnesium sulfate has bronchodilator activity in acute
asthma, possibly due to inhibition of calcium influx into airway smooth
muscle cells.
In patients whose condition doesn’t improve with the above management,
one can start IV aminophylline drip ( 5mg/kg/ hr infusion )
34.
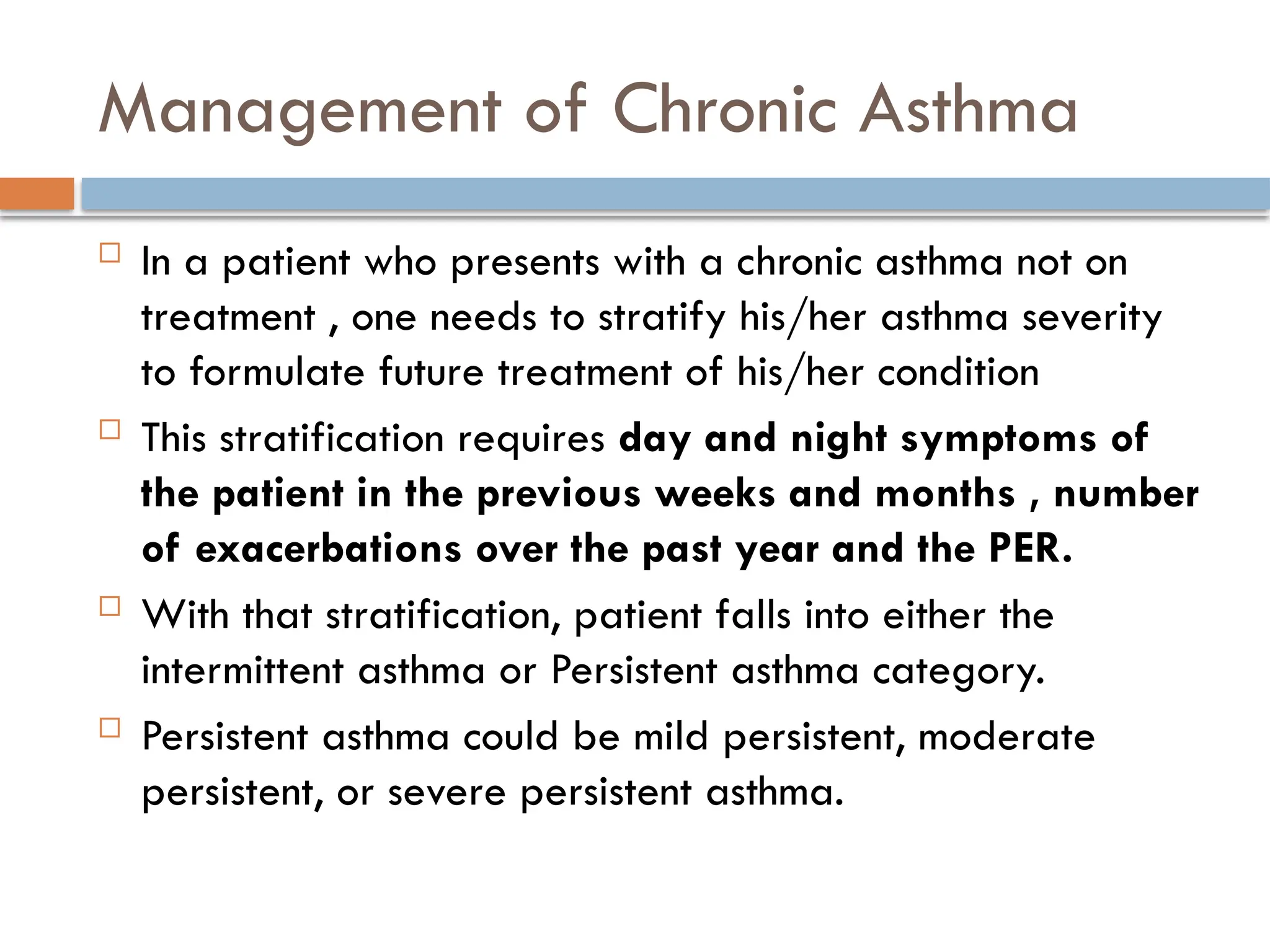
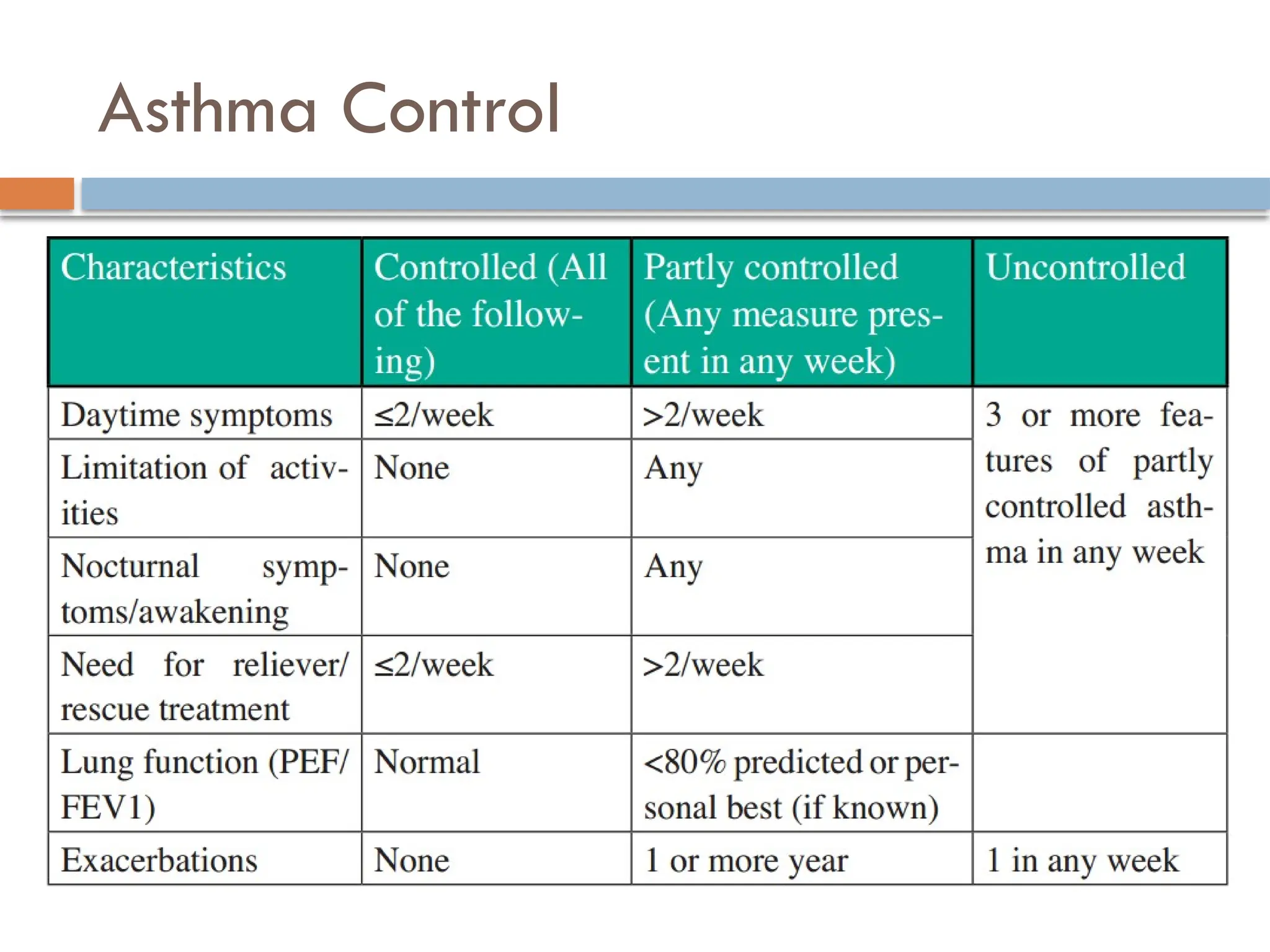
Management of ChronicAsthma
In a patient who presents with a chronic asthma not on
treatment , one needs to stratify his/her asthma severity
to formulate future treatment of his/her condition
This stratification requires day and night symptoms of
the patient in the previous weeks and months , number
of exacerbations over the past year and the PER.
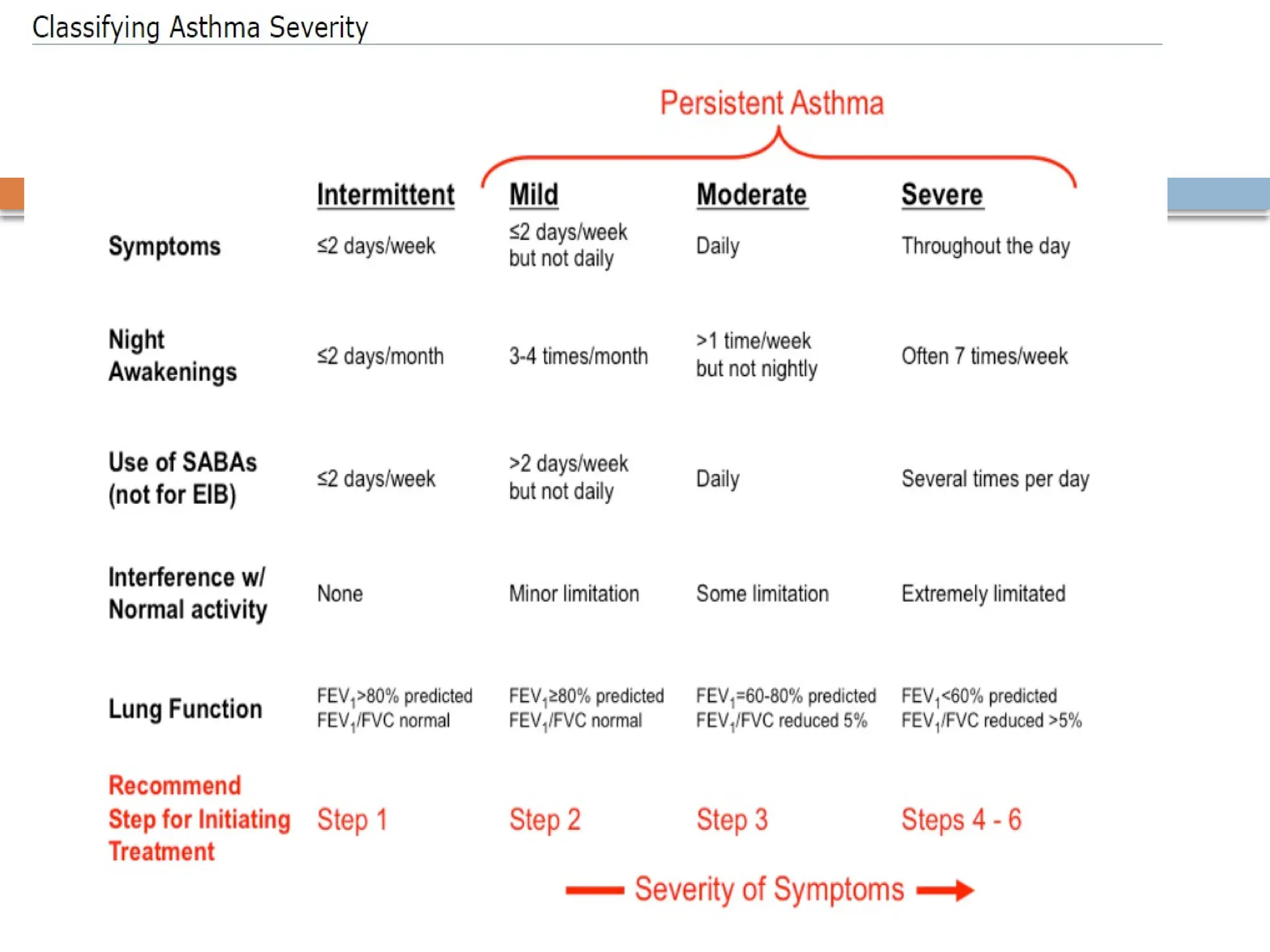
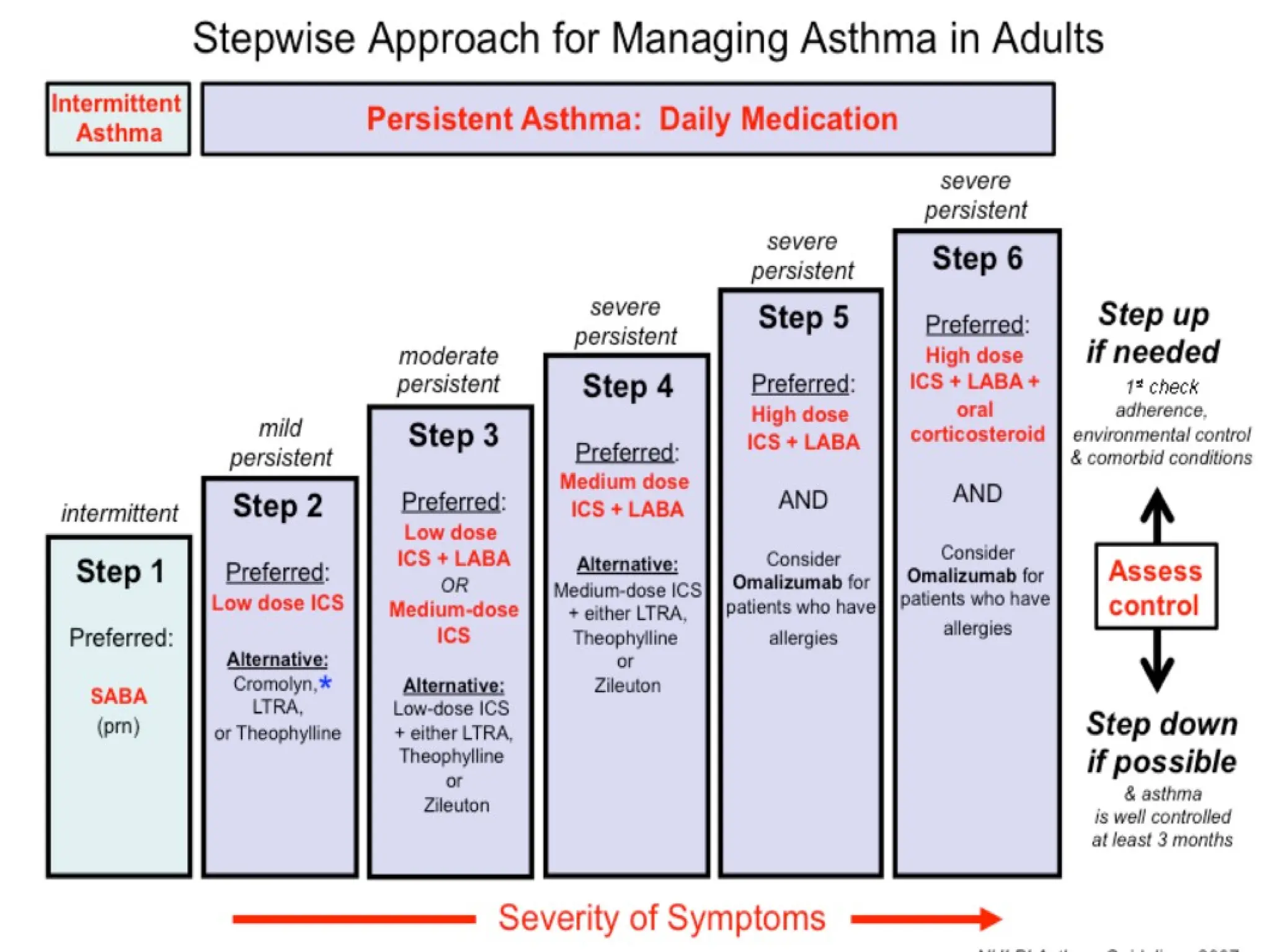
With that stratification, patient falls into either the
intermittent asthma or Persistent asthma category.
Persistent asthma could be mild persistent, moderate
persistent, or severe persistent asthma.
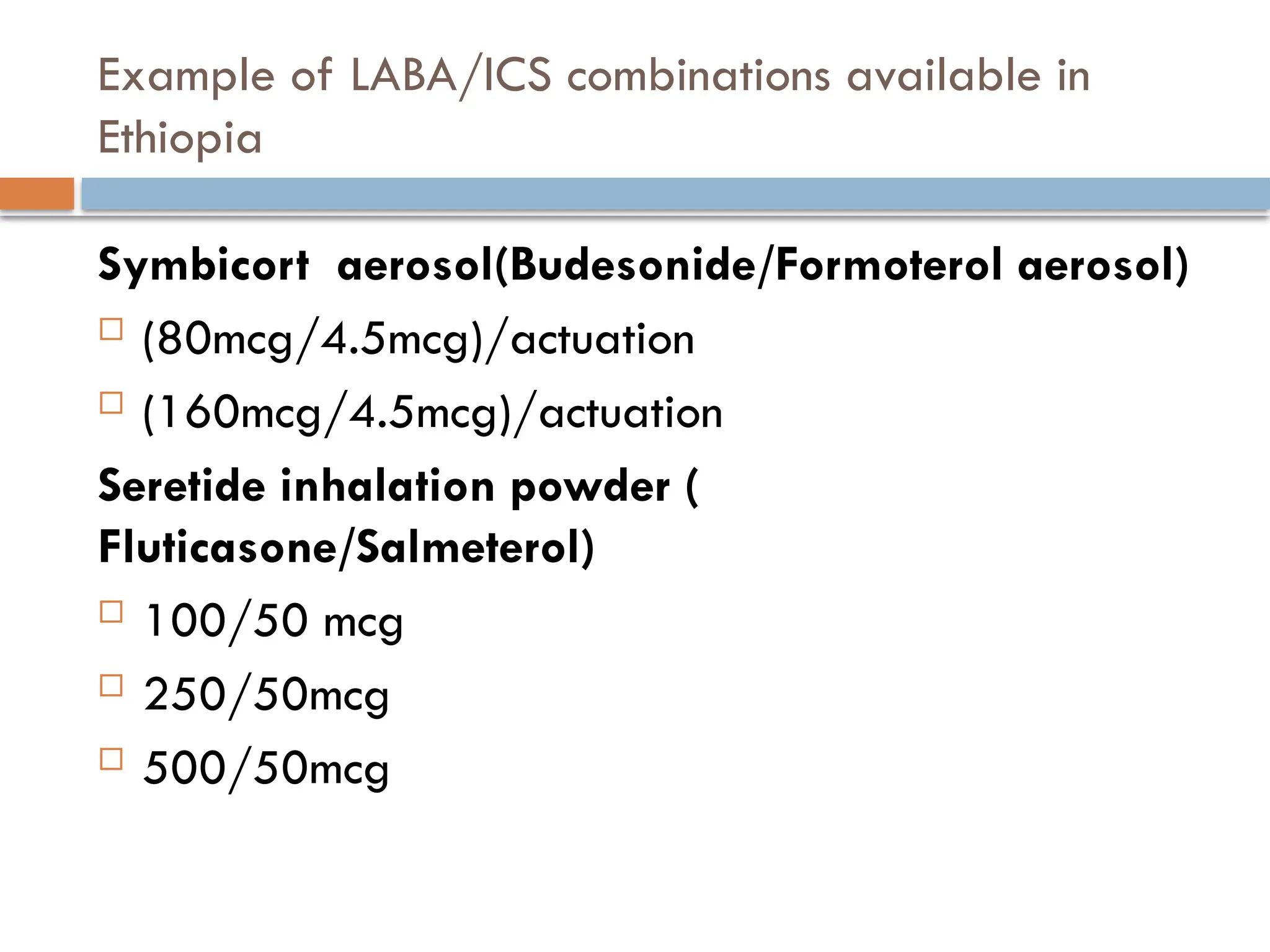
Example of LABA/ICScombinations available in
Ethiopia
Symbicort aerosol(Budesonide/Formoterol aerosol)
(80mcg/4.5mcg)/actuation
(160mcg/4.5mcg)/actuation
Seretide inhalation powder (
Fluticasone/Salmeterol)
100/50 mcg
250/50mcg
500/50mcg
![Exacerbation of Acute Severe Asthma.
These findings are indicators of Acute severe Asthma.
Tachycardia > 120 beats/min and or tachypnea > 30/min.
Use of accessory muscles of respiration.
Hypotension.
Inability to finish one sentence in one breath.
Silent chest.
Confusion or loss of consciousness.
Hypoxemia ((arterial partial pressure of oxygen [PaO2] <60 mmHg [8
kPa], pulse oxygen saturation [SpO2] <90 percent)
Pulsus Paradoxus ((ie, a fall in systolic blood pressure by at least 10
mmHg during inspiration)
PEF < 50% predicted or personal best.](https://image.slidesharecdn.com/asthma-250907091838-a613318b/75/Asthma-pptx-read-on-it-from-definition-to-managent-16-2048.jpg)