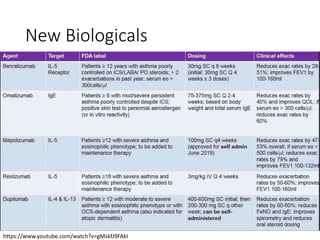
This document discusses asthma, including its definition, diagnosis, updates from GINA 2019, and exacerbation management. Asthma is a chronic inflammatory disease of the airways characterized by variable respiratory symptoms and airflow limitation. Diagnosis involves assessing symptoms and lung function tests. GINA 2019 focuses on personalized treatment plans. Exacerbations are acute worsening of symptoms and are managed with SABAs, corticosteroids, and new biological treatments targeting inflammatory proteins like IL-5. Proper inhaler technique and adherence to treatment are important to control asthma and prevent exacerbations.

![Status asthmaticus
• SABA: Salbutamol 2.5mg Q20min for 60 min then
Q1H, given with 0.25 to 0.5mg of ipratropium
improve FEV1
• Corticosteroids: IV methylprednisolone 60-125mg
Q6H for 24 hours
• MagSulf: 2gm IV over 20 minutes
• NOT RECOMMENDED: IV aminophylline
• Use of NIV not established as in COPD
Chakraborty RK, Basnet S. Status Asthmaticus. [Updated 2019 Nov 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls
Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526070/](https://image.slidesharecdn.com/asthma-200313065840/85/Asthma-GINA-2019-17-320.jpg)
![Reference
• © Global Initiative for Asthma, www.ginasthma.org
• Chakraborty RK, Basnet S. Status Asthmaticus.
[Updated 2019 Nov 29]. In: StatPearls [Internet].
Treasure Island (FL): StatPearls Publishing; 2019
Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK526070/](https://image.slidesharecdn.com/asthma-200313065840/85/Asthma-GINA-2019-20-320.jpg)






































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

