Introduction
• Surgical procedures
•interfere with the normal protective skin barrier
• expose the patient to microorganisms from both
endogenous and exogenous sources
• Prevention of surgical site infections (SSIs)
• primary concern to surgeons
• must be addressed in the planning of any
operation
4.
…Cont’d
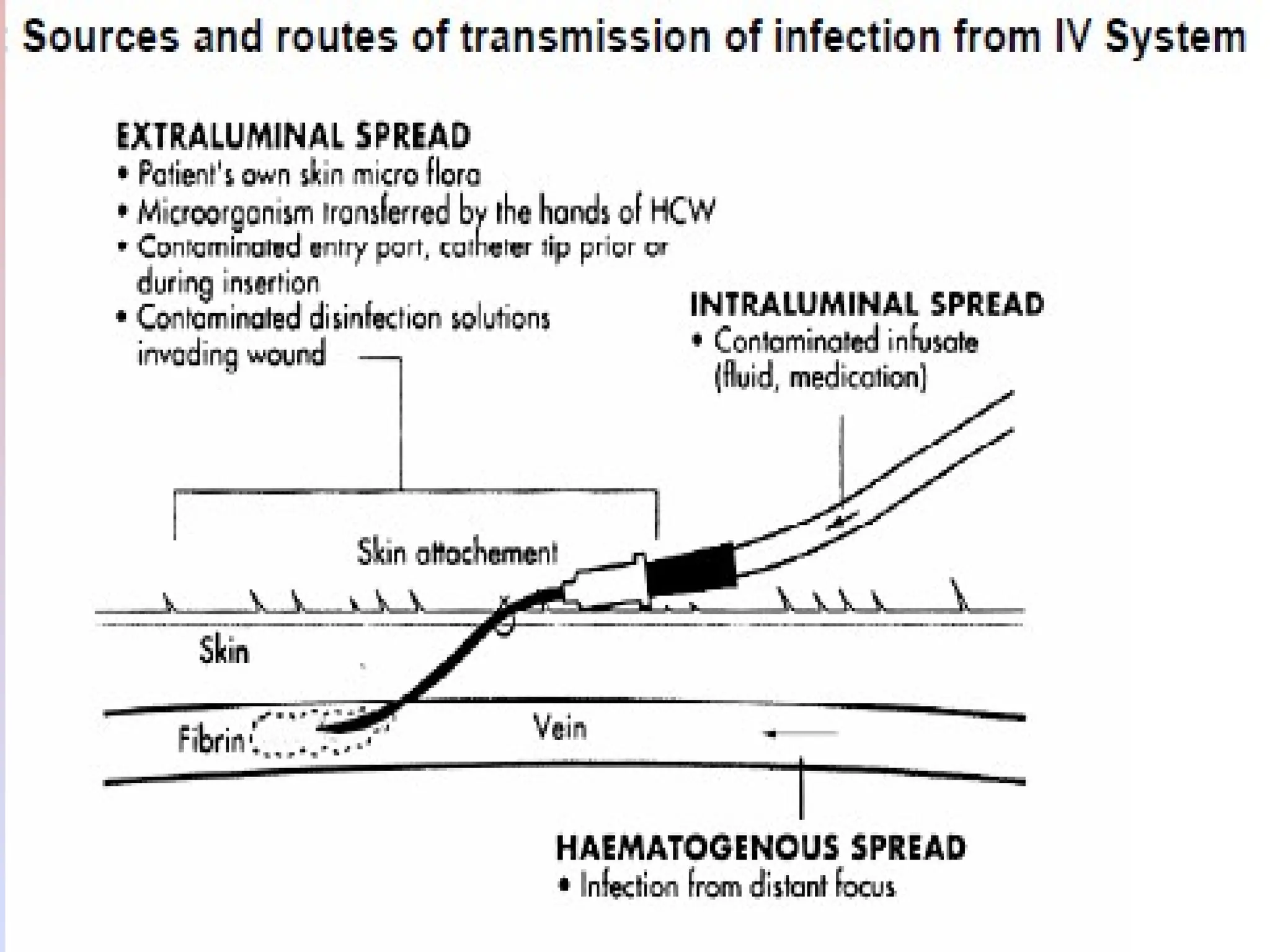
• Most diseasetransmissions occur due to actions of
health care personnel that ignore basic concepts of
aseptic techniques
• Reuse of syringes/ needles
• Touching of a sterile device on to a non-sterile surface
• Entering of a sterile solution without adequate
decontamination of the portal of entry…
5.
Surgical site infections(SSI)
Def:(CDC)
– an incisional SSI is an infection that occurs at the
incision site within 30 days after surgery or within 1
year if a prosthetic implant is in place
– Surgical site infection (SSI) is a major cause of patient
morbidity, mortality, and health care costs
• Factors thatcontribute to the development of SSI
(1) those arising from the patient's health status
(2) those related to the physical environment where
surgical care is provided, and
(3) those resulting from clinical interventions that
increase the patient's inherent risk
Asepsis
• Def:
–Reducing thenumber of microbes to an
irreducible number
• The purposeful prevention of the transfer of microbes
from one person to another
• Sum total of the effort to keep the pt’s env’t free from
contamination and the pt free from colonization
10.
…Cont’d
• Aseptic techniques
–is a general term involving practices that minimize the
introduction of microorganisms to pts during pt care
– used to reduce the risk of post-procedure infections and
to minimize the exposure of health care providers to
potentially infectious microorganisms
– include practices performed just before, during or
after any invasive procedures
11.
• Poor adherenceto aseptic techniques results in considerable
morbidity and mortality*
• Health care personnel should be trained in aseptic
technique and demonstrate competency
• Impt to all health care facilities to establish policies
regarding procedures that require aseptic techniques
• Supervision and monitoring of infection control
activities is a critical element of infection control
12.
Antiseptics
• Antisepsis
– preventionof sepsis by inhibition or destruction of
causative agents
• Antiseptic agents
• Chemicals applied to the skin or other living tissue
to inhibit or kill microorganisms ( both transient &
resident) thereby reducing the total bacterial counts
13.
Characteristics of Antiseptics
•Rapid reduction of flora
• Wide-range of killing power
• Absence of absorption across skin/ mucous membranes
• bactericides or bacteriostatics
** Know the appropriate dilution
14.
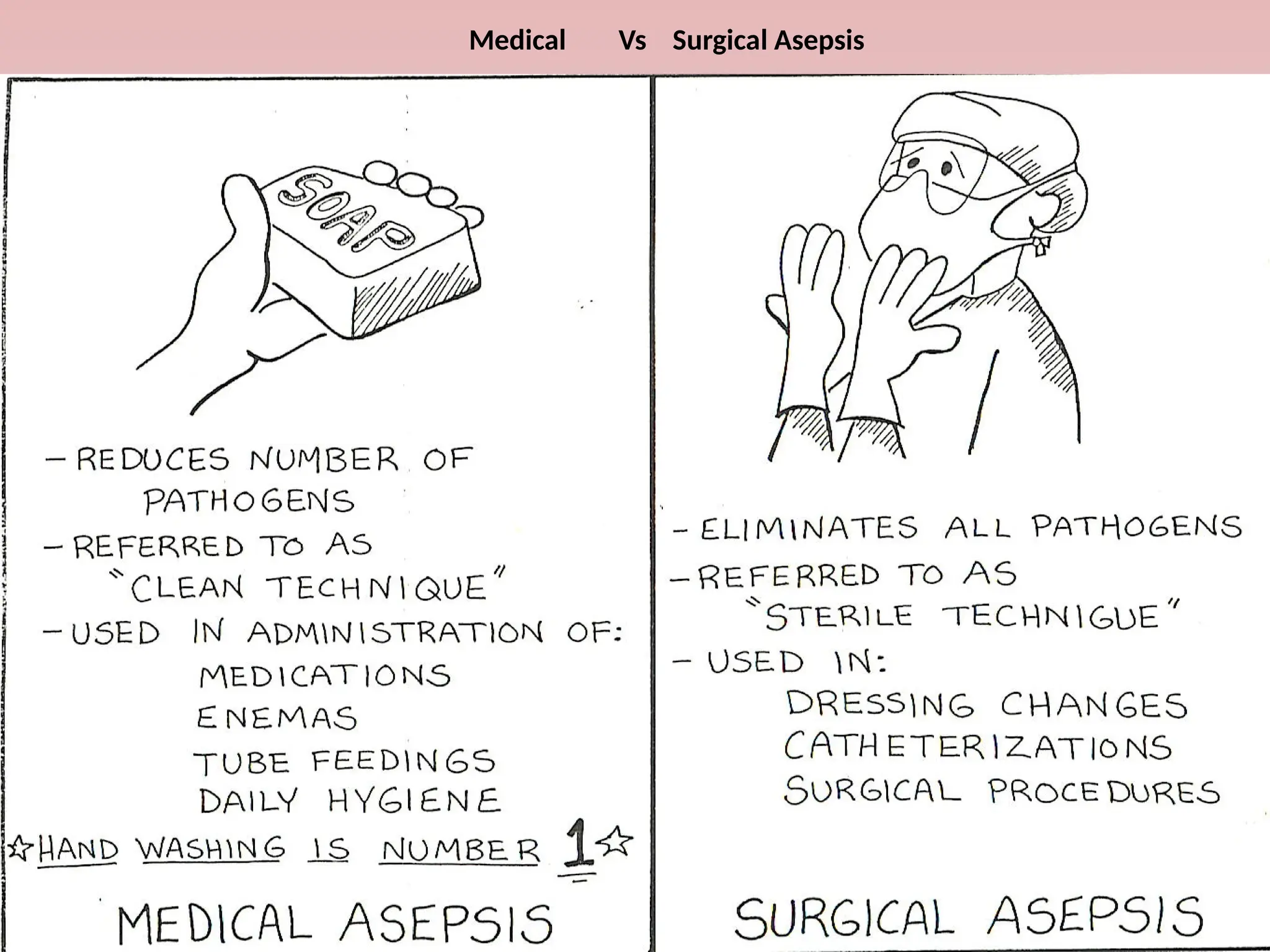
Antiseptics Vs Disinfectants
•Antiseptics
– Are cleaning solutions that inhibit and destroy
microorganisms on the living tissue (skin ,…
• Eg. Isopropyl alcohol, betadine
• Disinfectants
– Are cleaning solutions that inhibit and destroy
microorganisms on environmental surfaces
• Eg. Bleach solutions
15.
Classification
• Two categoriesof asepsis
General asepsis
• w/h applies to pt care procedures outside the OR*
Surgical asepsis
• Relating to procedures /processes designed to prevent
surgical site infection
16.
Principles of medicalasepsis
• When the body is penetrated ,and natural barriers such
as the skin is bypassed ,the pt is susceptible to any
microbes that might enter
• Even though intact skin is a good barrier against
microbial contamination, a pt can become colonized
with microbes if appropriate precautions are not taken
17.
…Cont’d
• All bodyfluids from any pt is considered contaminated
• The healthcare team and the env’t can be a source of
contamination for the pt
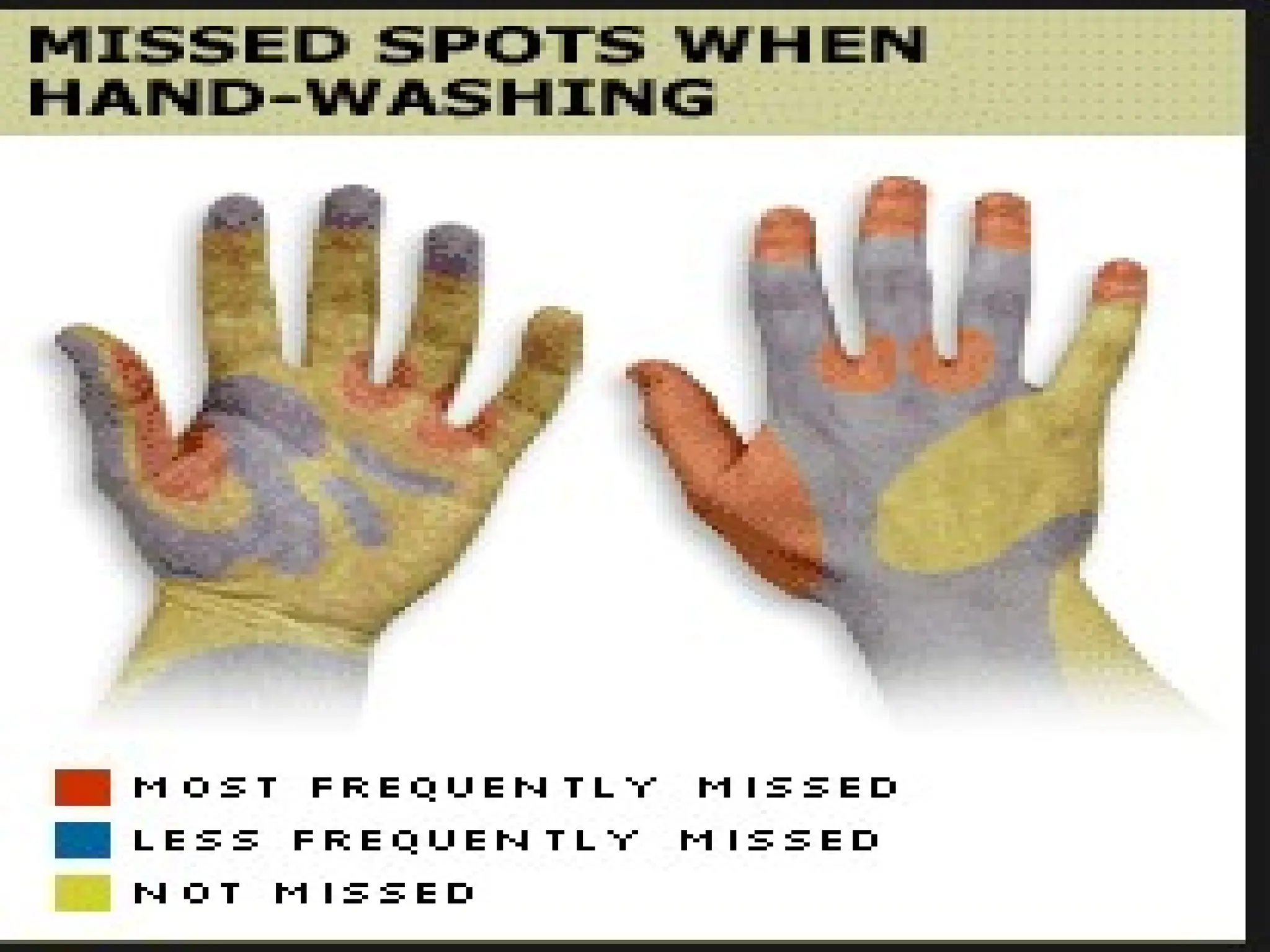
• Hands of health workers are the most common
source of cross-infection
18.
Key processes formedical (non-surgical)
procedures with aseptic techniques
• Hand antisepsis & appropriate use of gloves
• Skin antisepsis of the site of insertion of invasive devices (eg.
Ivs, IM
• Using and maintaining sterile pt care equipment*
• introduction of sterile item into a pt should always be
performed with “no-touch” technique**
(eg. catheterization
20.
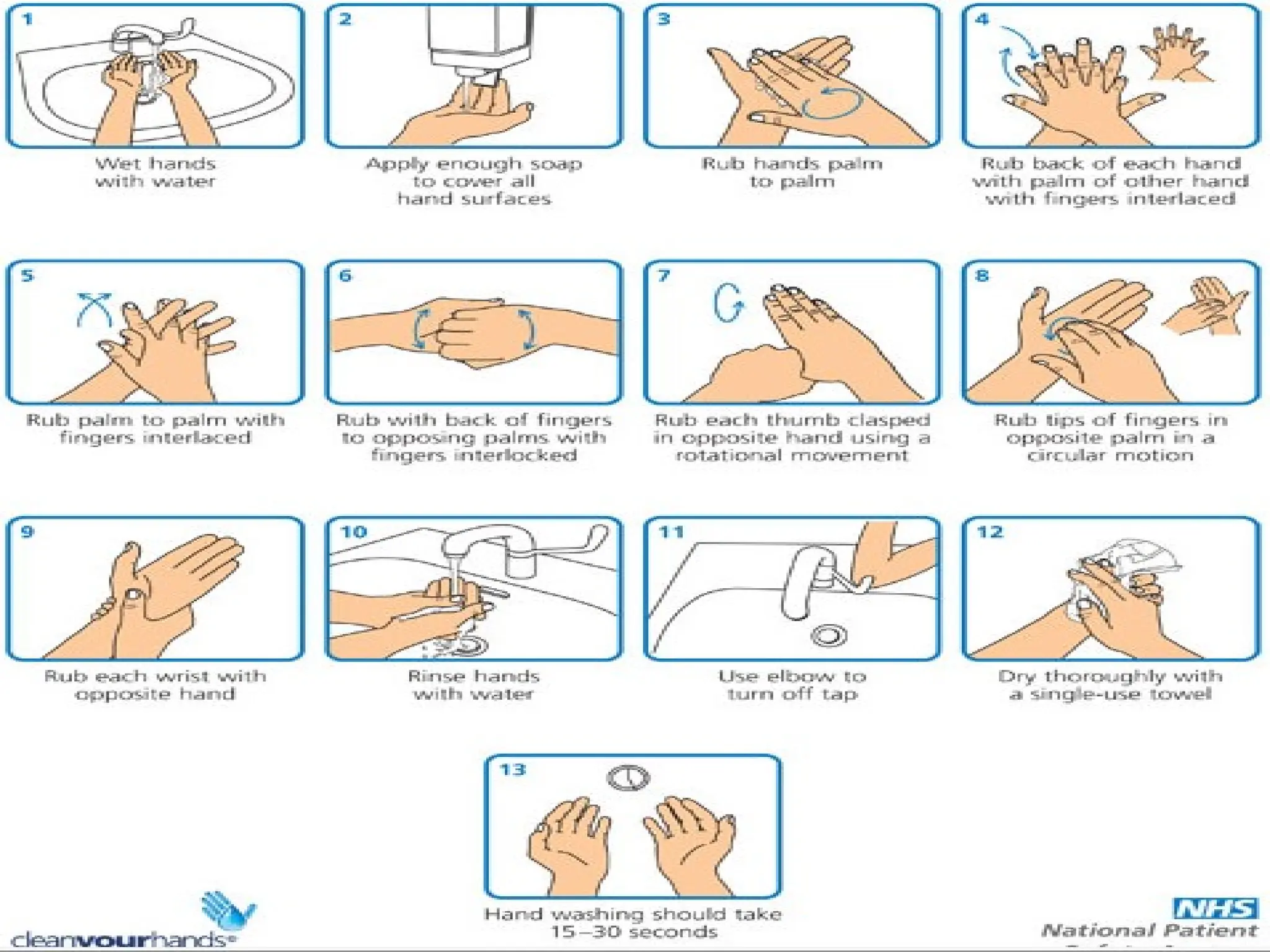
Hand washing
- isthe single most important procedure for preventing
nosocomial infection
• When and how*
• Soap or antiseptics
• the use of gloves
27.
Cornerstones Of MedicalAsepsis
• Know what is dirty
• Know what is clean
• Know what is sterile
• Keep this conditions separate
• Remedy contamination immediately
28.
28
Surgical Asepsis
Keep thesurgical
environment completely free
of all microorganisms
Sterile technique used for
even minor operation or
injections
Object is either sterile or not
sterile; if unsure then it is not
sterile.
29.
Surgical Principles OfAsepsis
• The pt should not be a source of contamination
• The OR team should not be a source of contamination*
• Recognize potential env’tal contamination
– proper room cleaning, doors kept closed, limited traffic
• The surgical scrub must be done meticulously
• Technique of the surgeon of utmost importance
30.
Key Processes OfSurgical Asepsis
• Operation theater
• Should Meet standards of asepsis at all times
• Instruments and equipments
• Disinfected , Sterilized
• Surgical team
• Use of Personal protective equipments (hat, mask, goggle
• Surgical hand scrub
• sterile gloves
• sterile guans
• Safe handling of instruments
• Post-procedure hand washing
31.
…Cont’d
• Patient
• preoperativehospital stay (as short as possible)
• Preparation of operative site ( hygiene, hair removal……
• Remote infections ( treated)
• Prophylactic antibiotics, bowel preparation in colon surgery
• Skin preparation
• Drapes ,…
• Surgeon
• Technique ( dissection, hemostasis, …
• Use of drains, electrocautery,….
• Duration of operation, wound (close/ left open)….
• Wound management
Operation Theatre
• Filteredair
• frequent air change
• laminar flow of air
• limited human trafficking,…
Even the best OR design will not compensate for
improper surgical technique or failure to pay attention
to infection prevention
35.
Instruments and Equipments
•Decontamination
– process of removing or destroying micro-organisms and
organic matter. Making a re-usable item safe for patients
and staff
• Cleaning
– process that physically removes organic matter ( blood,
tissue, body fluids) but does not remove micro-organisms
36.
...cont’d
• Disinfection
• Processthat reduces the number of micro-organisms
to a level that is not harmful at the site of use. Kills or
removes micro-organisms with the exception of
bacterial spores
• Sterilization
• Is the complete elimination or destruction of all
microorganisms , including spores
37.
Methods Of Decontamination
•Disinfection
Physical
• Low temp steam
• Boiling water
• Washer disinfections
Chemical
• Chemical disinfectants
– (Glutareldehdye 2%, Cidex, Miltons, Clearsol, alcohol)
38.
Methods Of Sterilization
•Steam (autoclaving)
• Hot air (ovens)
• Ethylene Oxide
• Low temp steam and formaldehyde
• Gas plasma
• Irradiation
• Sporicidal chemicals
* Autoclaves and sterilization systems should be continuously
monitored with routine testing for efficiency and performance
39.
Patient Preparation
• Preoperativehospital stay
- should be as short as possible to reduce likelihood of being
colonized by nosocomial pathogens or acquire nosocomial
infections
• Remote infections
• Presence of untreated remote infection is associated with
an increased incidence of wound infection
• Should be appropriately treated
40.
Preparation Of Skin
•The sole reason for preparing the pt's skin before an operation is
to reduce the risk of wound infection
• A preoperative antiseptic bath
• not necessary for most surgical pts ( but assess their personal
hygiene)
• Chlorhexidine gluconate is the recommended agent for such
baths(if needed)
• Obvious dirt, grime, and dried blood should be mechanically
cleansed from the operative site by using sufficient friction
41.
Hair Removal
• shouldnot be removed from the operative site unless it
physically interferes with accurate anatomic approximation of the
wound edges
• If hair must be removed, it should be clipped in the OR
• Shaving hair from the operative site, particularly on the evening
before operation or immediately before wound incision in the OR,
increases the risk of wound infection
• Depilatories are not recommended
– serious irritation & rashes (esp. when used near eyes &
genitalia)
Surgical wound classification
•Clean / Class I
– Uninfected operative wound in which no inflammation is
encountered.Respiratory, alimentary and genito-urinary
tracks are not involved
– 1.5%
• Clean-contaminated/ Class II
– Any operative wound in which the respiratory, alimentary or
genito-urinary tracks are opened in a controlled manner
without contamination
– 8%
44.
...cont’d
• Contaminated/ ClassIII
– Open fresh accidental wounds. Operations with major break in
sterile techniques. Gross contamination or major spillage. Non
purulent inflammation
– 10-15%
• Dirty-infected/ Class IV
– Old traumatic wounds with devitalised tissue and those that
involve existing clinical infection or perforated viscera. Organisms
involved were present in the operative field before the operation
– 25%
45.
Prepping (skin preparation)
•Necessary reduction in microorganisms can be achieved
by using
- 70% povidone-iodine (10% available povidone-iodine &
1%
available iodine) or
- 0.5% chlorhexidine gluconate
- 70% isopropyl alcohol
both for mechanical cleansing of the intertriginous folds & the
umbilicus and for painting the operative site
For iodine-sensitive pts, one can use isopropyl or 70% ethyl
alcohol. Apply to the skin with a gauze swab for 3 minutes and
allow to dry before draping
46.
Draping
• Sterile drapeshelps to create sterile surgical
field(s) by delineating the field around the pt
• Sterile drape packs should be opened aseptically
• Contents do not touch non-sterile items
• Drapes should be sterile, dry
– impermeable(if possible)
47.
Surgical Team
• Thesurgical scrub
• Definition
– is the process of removing as many microorganisms as
possible from the hands and forearms by mechanical
washing and chemical antisepsis before participating in a
surgical procedure
• Despite the mechanical action and the chemical
antimicrobial component of the scrub process, skin is never
sterile
• Duration
• Not universally defined
• 5 min scrub before the 1st
case
• 2 - 3 min scrub in between cases
48.
..cont’d
• Technique
– surgicalscrub brush and an antimicrobial soap
solution
– Chlorhexidine containing
– Alcohol based solutions / lotions
49.
There Is NoCompromise with Sterility
It’s Considered Sterile or Unsterile
50.
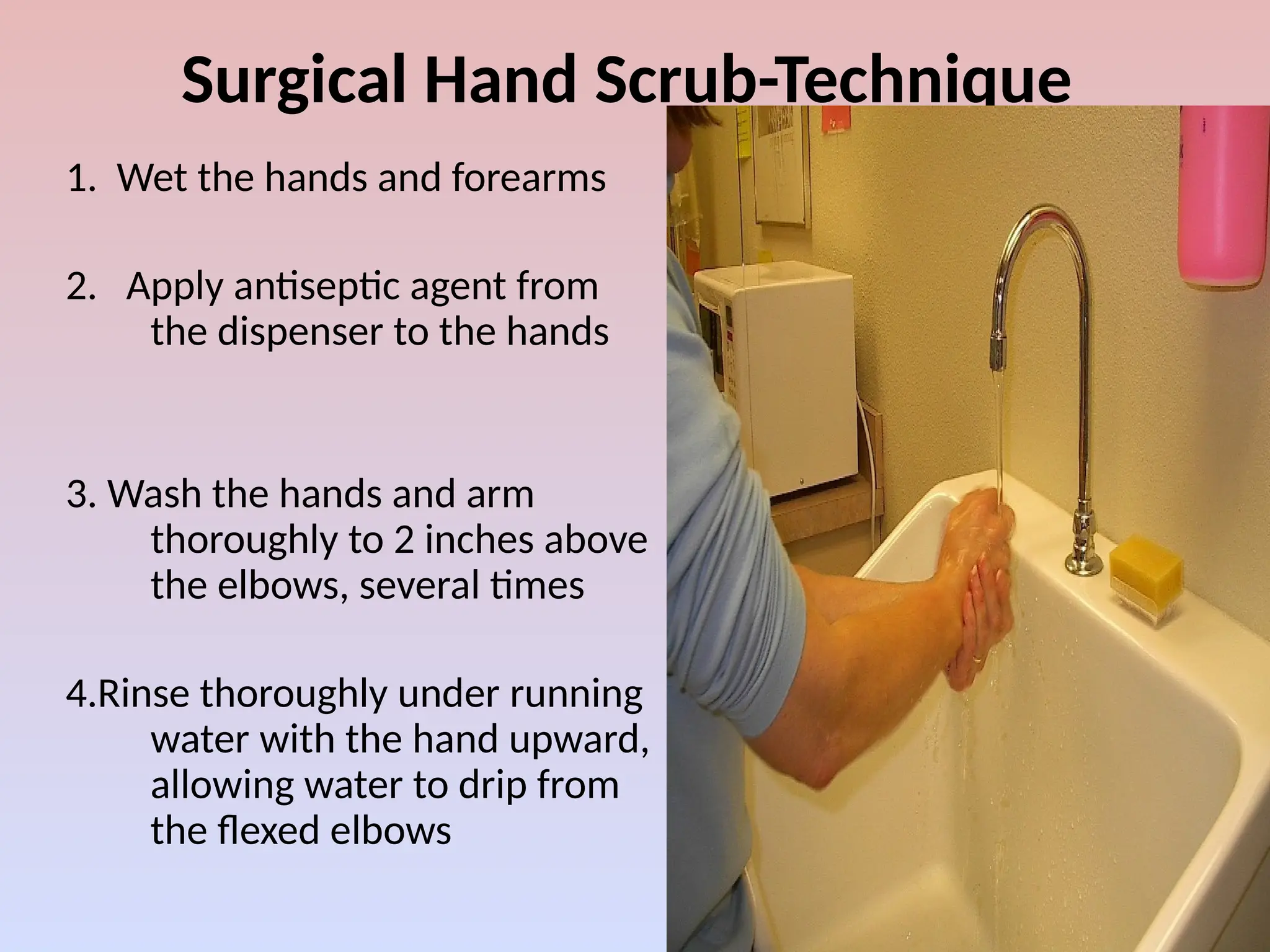
Surgical Hand Scrub-Technique
1.Wet the hands and forearms
2. Apply antiseptic agent from
the dispenser to the hands
3. Wash the hands and arm
thoroughly to 2 inches above
the elbows, several times
4.Rinse thoroughly under running
water with the hand upward,
allowing water to drip from
the flexed elbows
51.
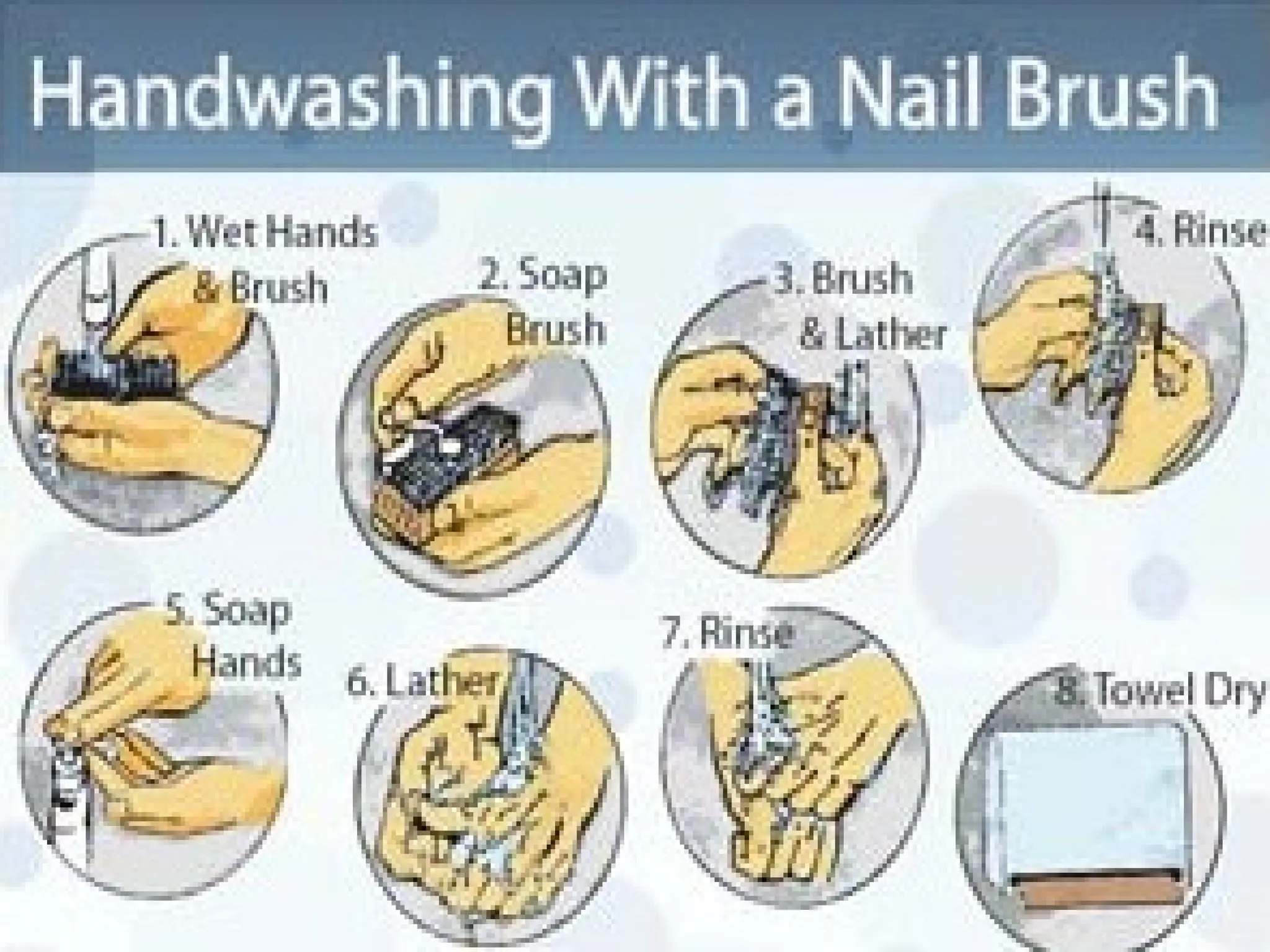
5. Take asterile brush or
sponge (from a package or
dispenser) and apply an
antiseptic agent ( if it is
not impregnated in the
brush)
6. Scrub each individual
finger, including the nails,
and the hands, a half
minute for each hand.
52.
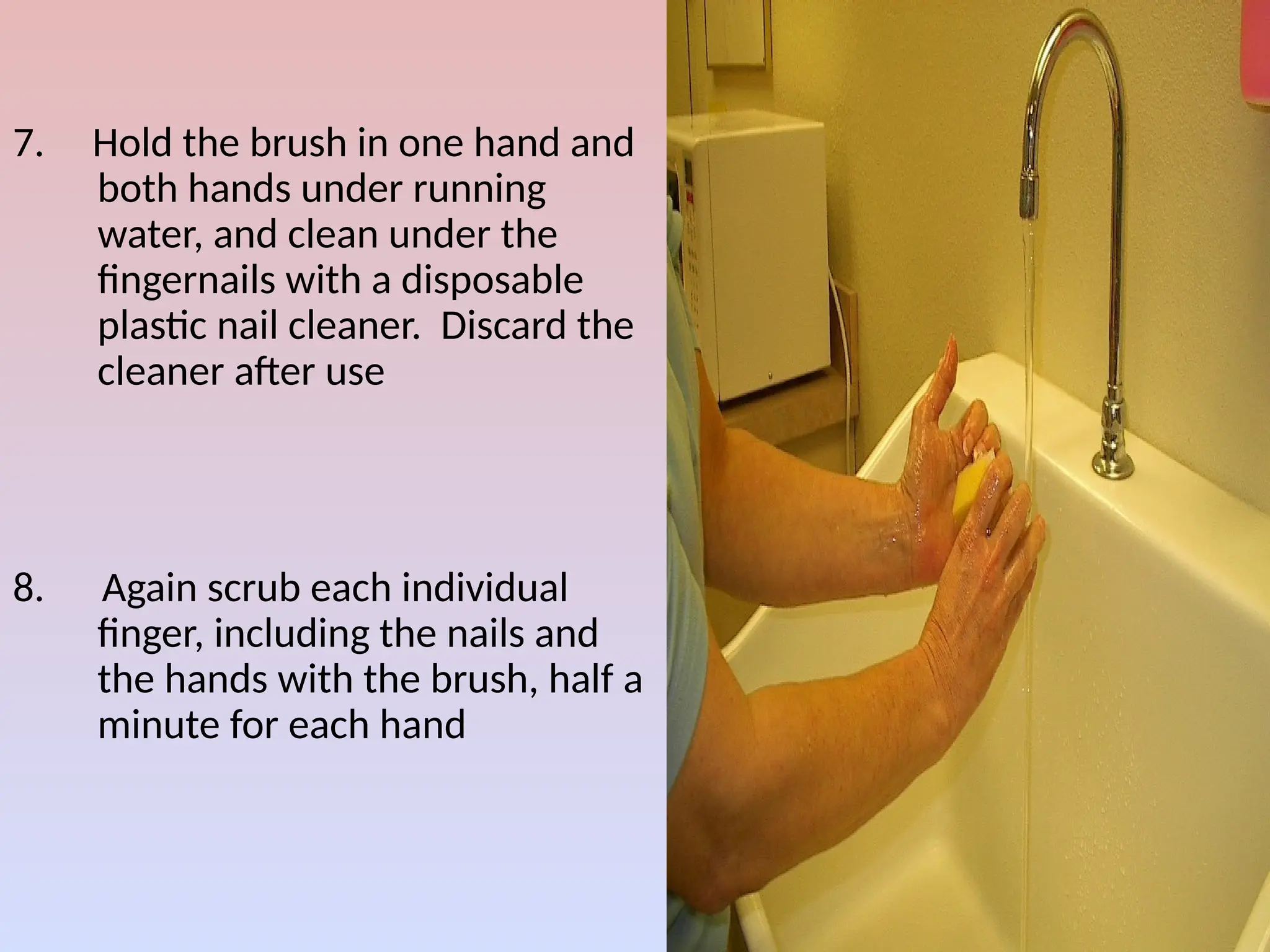
7. Hold thebrush in one hand and
both hands under running
water, and clean under the
fingernails with a disposable
plastic nail cleaner. Discard the
cleaner after use
8. Again scrub each individual
finger, including the nails and
the hands with the brush, half a
minute for each hand
53.
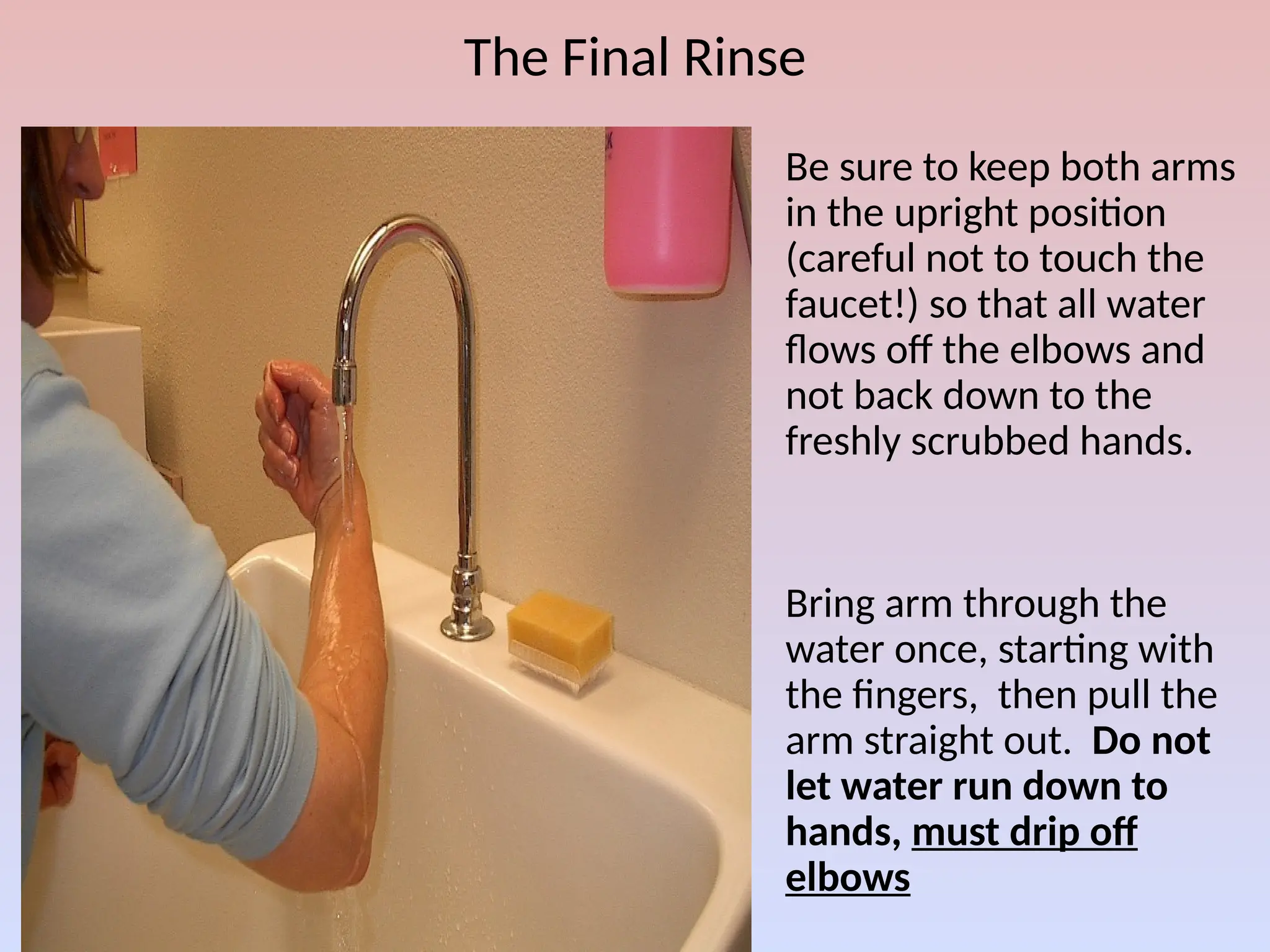
The Final Rinse
1.Be sure to keep both arms
in the upright position
(careful not to touch the
faucet!) so that all water
flows off the elbows and
not back down to the
freshly scrubbed hands.
2. Bring arm through the
water once, starting with
the fingers, then pull the
arm straight out. Do not
let water run down to
hands, must drip off
elbows
54.
9. Rinse thehands and brush, and discard the brush
10. Reapply the antimicrobial agent and wash the hands
and arms, applying friction to the elbows, for 3
minutes. Interlace the fingers to clean between
them
11. Rinse the hands and arms as described in the
previous slide.
55.
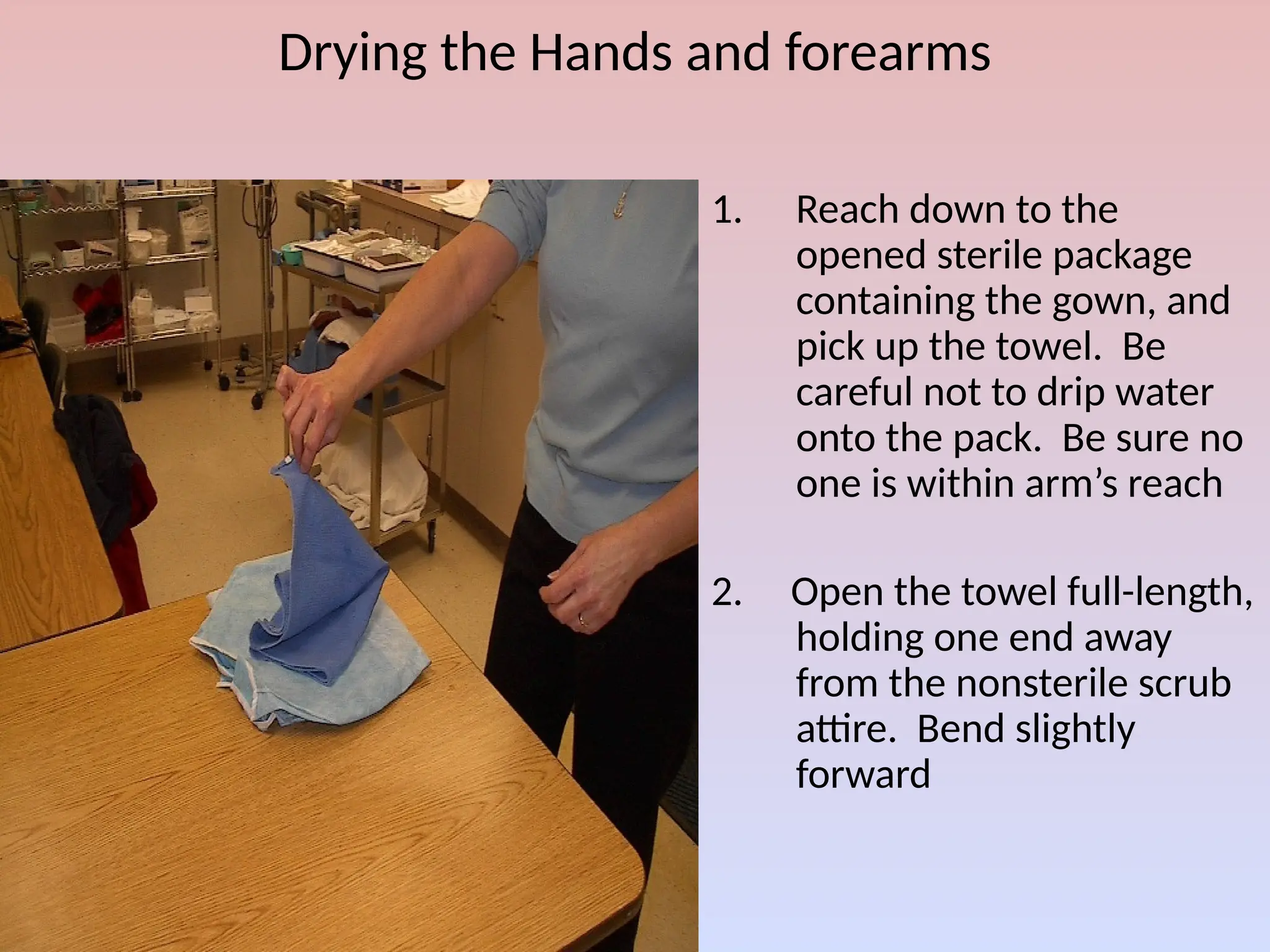
Drying the Handsand forearms
1. Reach down to the
opened sterile package
containing the gown, and
pick up the towel. Be
careful not to drip water
onto the pack. Be sure no
one is within arm’s reach
2. Open the towel full-length,
holding one end away
from the nonsterile scrub
attire. Bend slightly
forward
56.
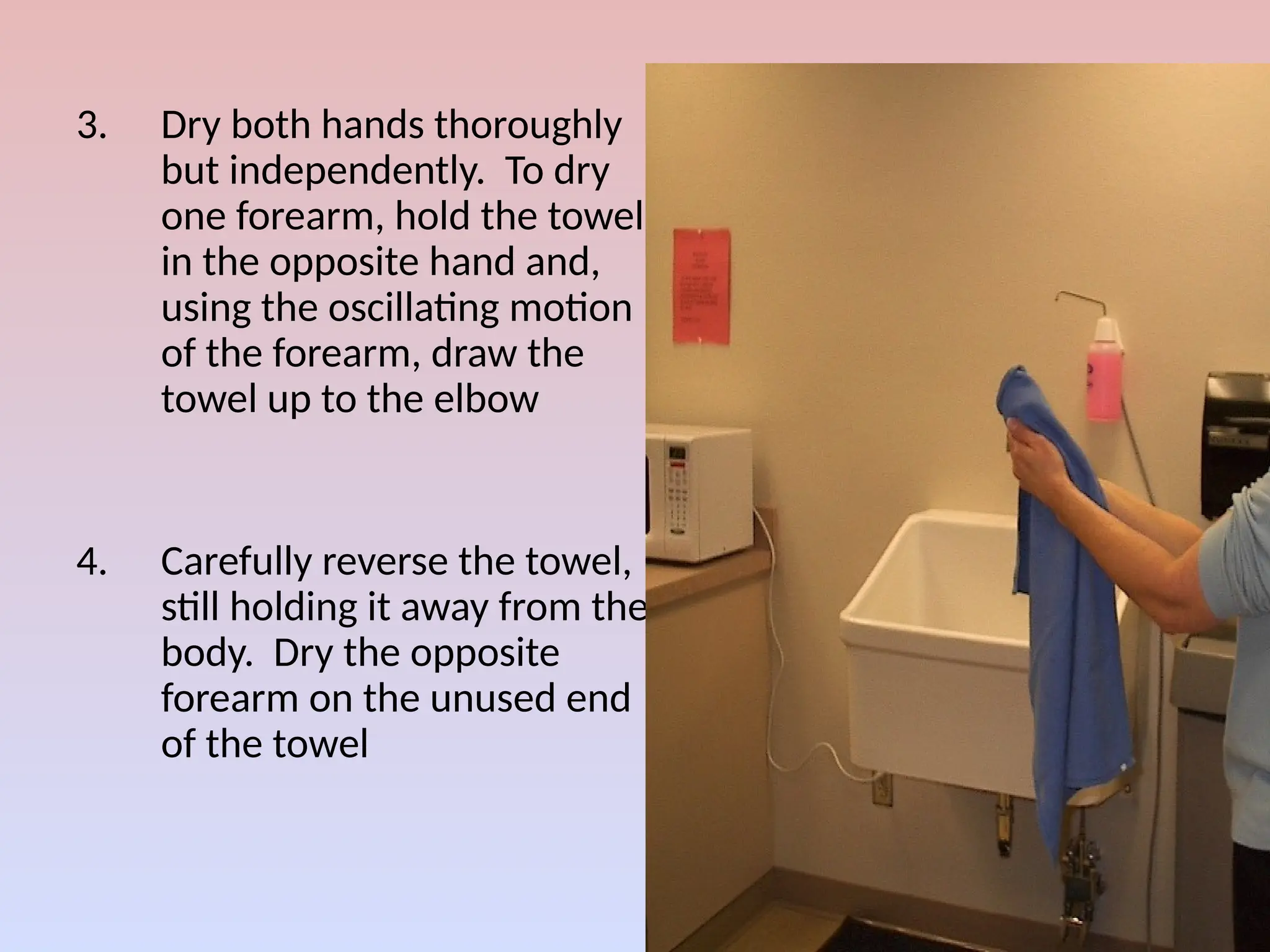
3. Dry bothhands thoroughly
but independently. To dry
one forearm, hold the towel
in the opposite hand and,
using the oscillating motion
of the forearm, draw the
towel up to the elbow
4. Carefully reverse the towel,
still holding it away from the
body. Dry the opposite
forearm on the unused end
of the towel
57.
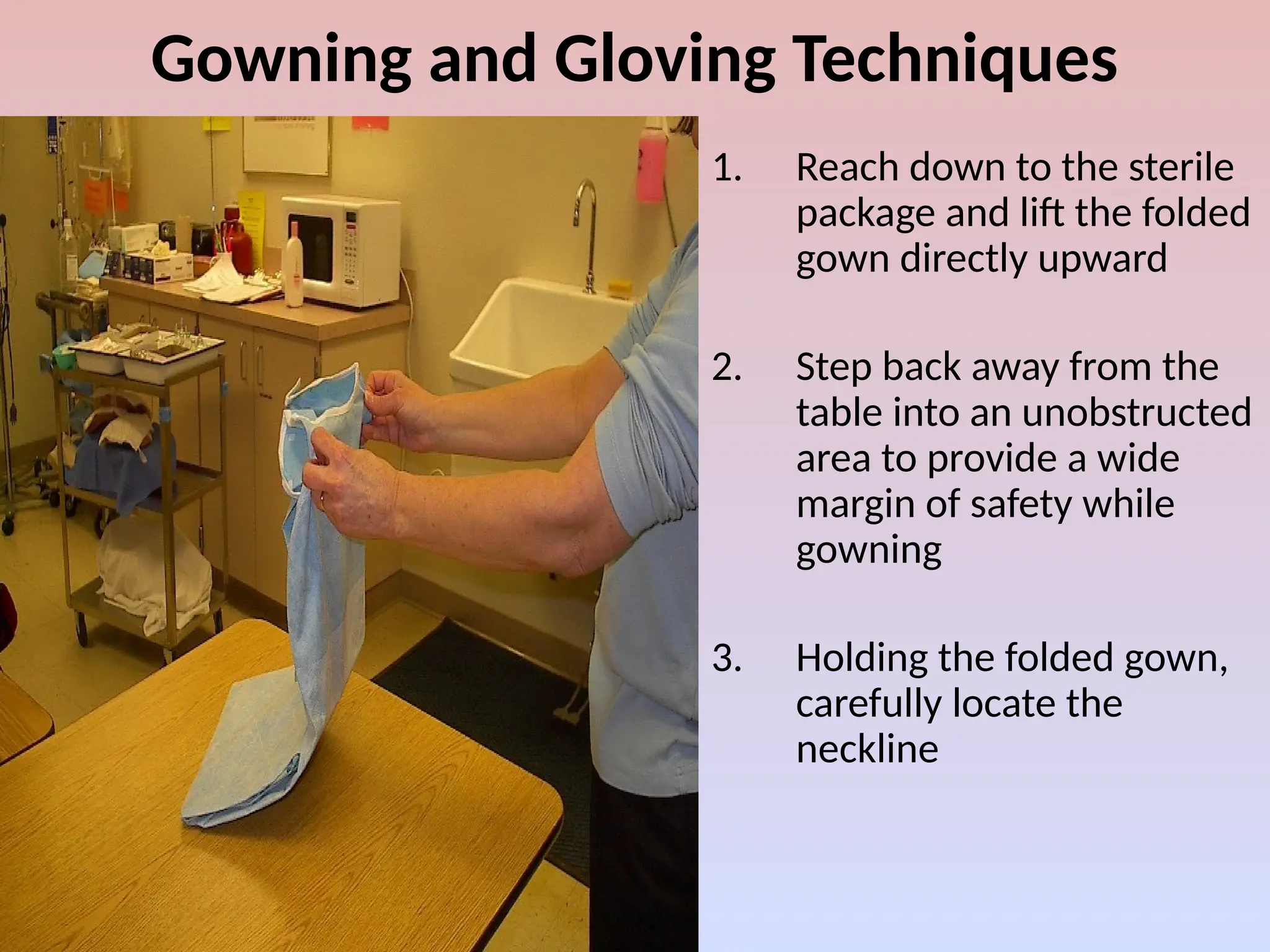
Gowning and GlovingTechniques
1. Reach down to the sterile
package and lift the folded
gown directly upward
2. Step back away from the
table into an unobstructed
area to provide a wide
margin of safety while
gowning
3. Holding the folded gown,
carefully locate the
neckline
58.
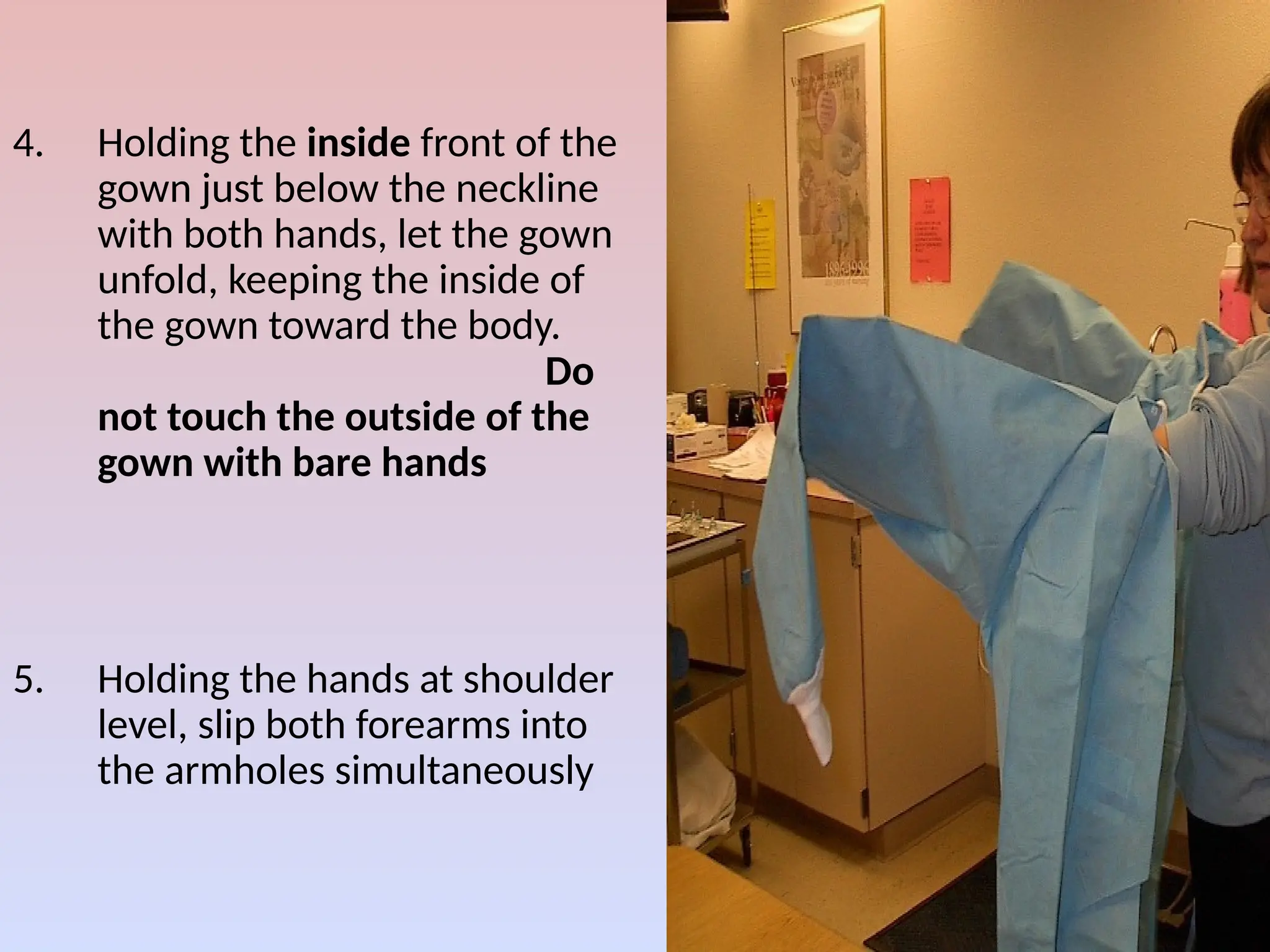
4. Holding theinside front of the
gown just below the neckline
with both hands, let the gown
unfold, keeping the inside of
the gown toward the body.
Do
not touch the outside of the
gown with bare hands
5. Holding the hands at shoulder
level, slip both forearms into
the armholes simultaneously
59.
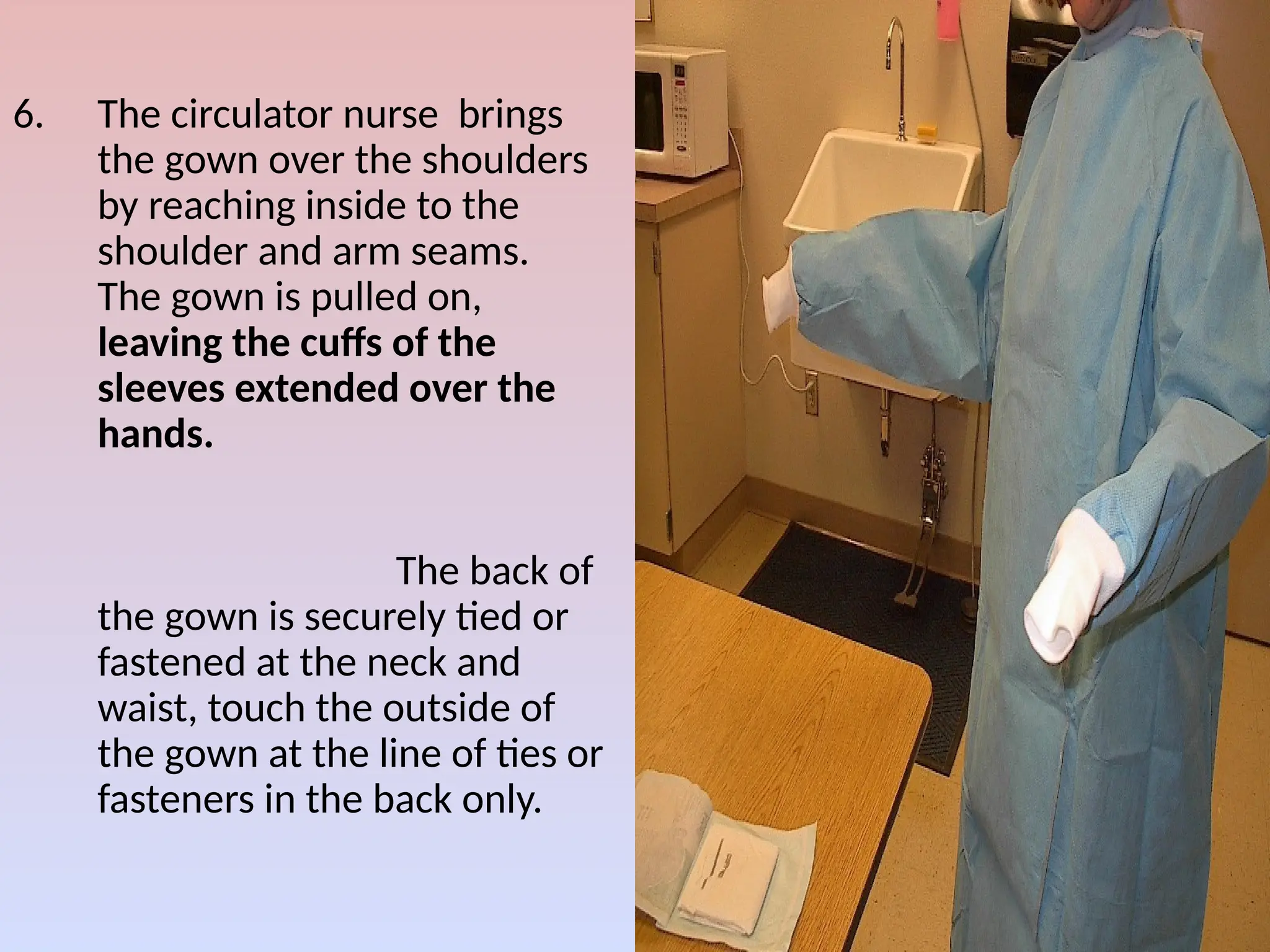
6. The circulatornurse brings
the gown over the shoulders
by reaching inside to the
shoulder and arm seams.
The gown is pulled on,
leaving the cuffs of the
sleeves extended over the
hands.
The back of
the gown is securely tied or
fastened at the neck and
waist, touch the outside of
the gown at the line of ties or
fasteners in the back only.
60.
Gloving --- ClosedGloving Technique
1. Using the right hand and keeping it within
the cuff of the sleeve, pick up the left glove
from the inner wrap of the glove package by
grasping the folded cuff
61.
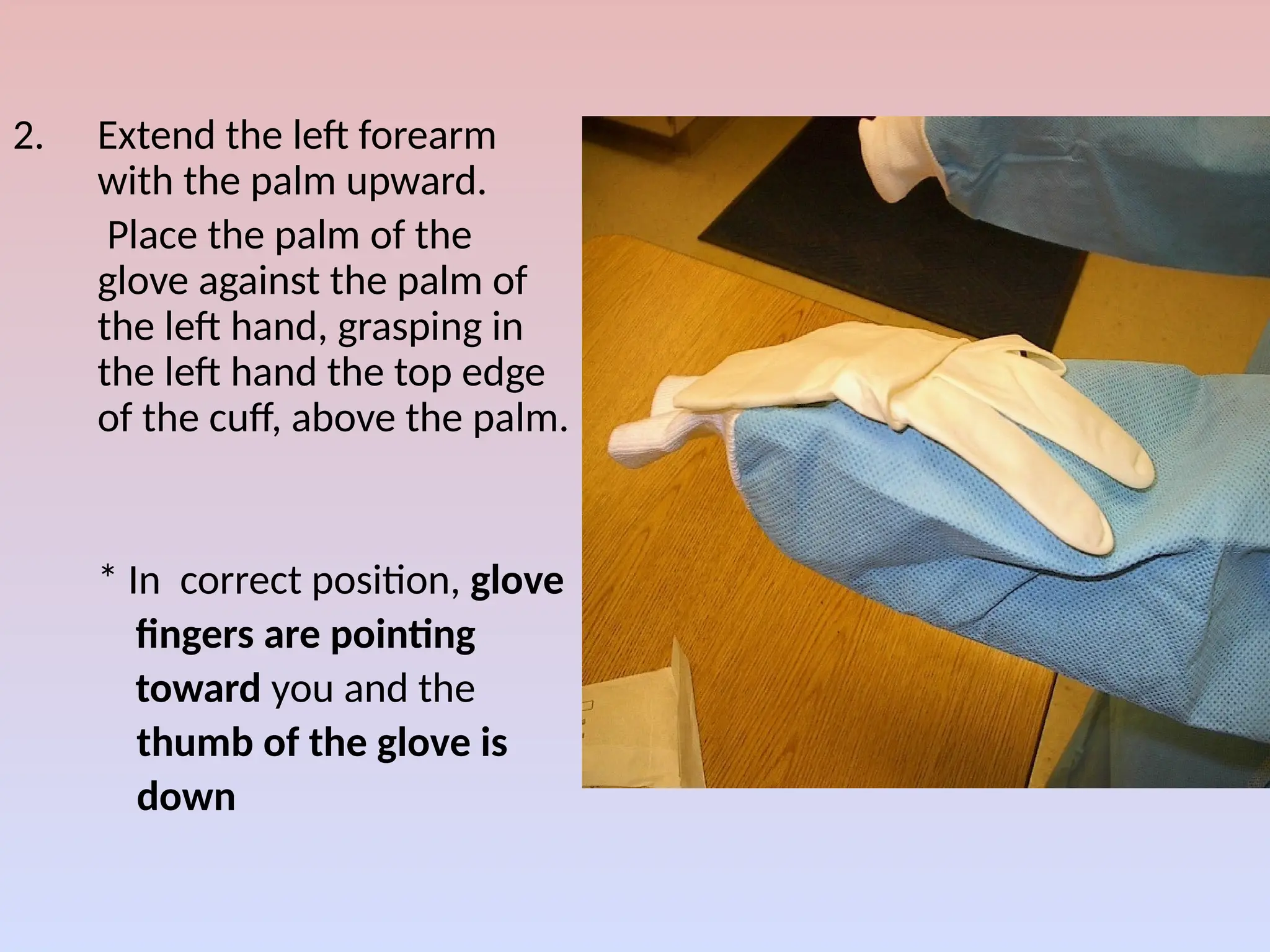
2. Extend theleft forearm
with the palm upward.
Place the palm of the
glove against the palm of
the left hand, grasping in
the left hand the top edge
of the cuff, above the palm.
* In correct position, glove
fingers are pointing
toward you and the
thumb of the glove is
down
62.
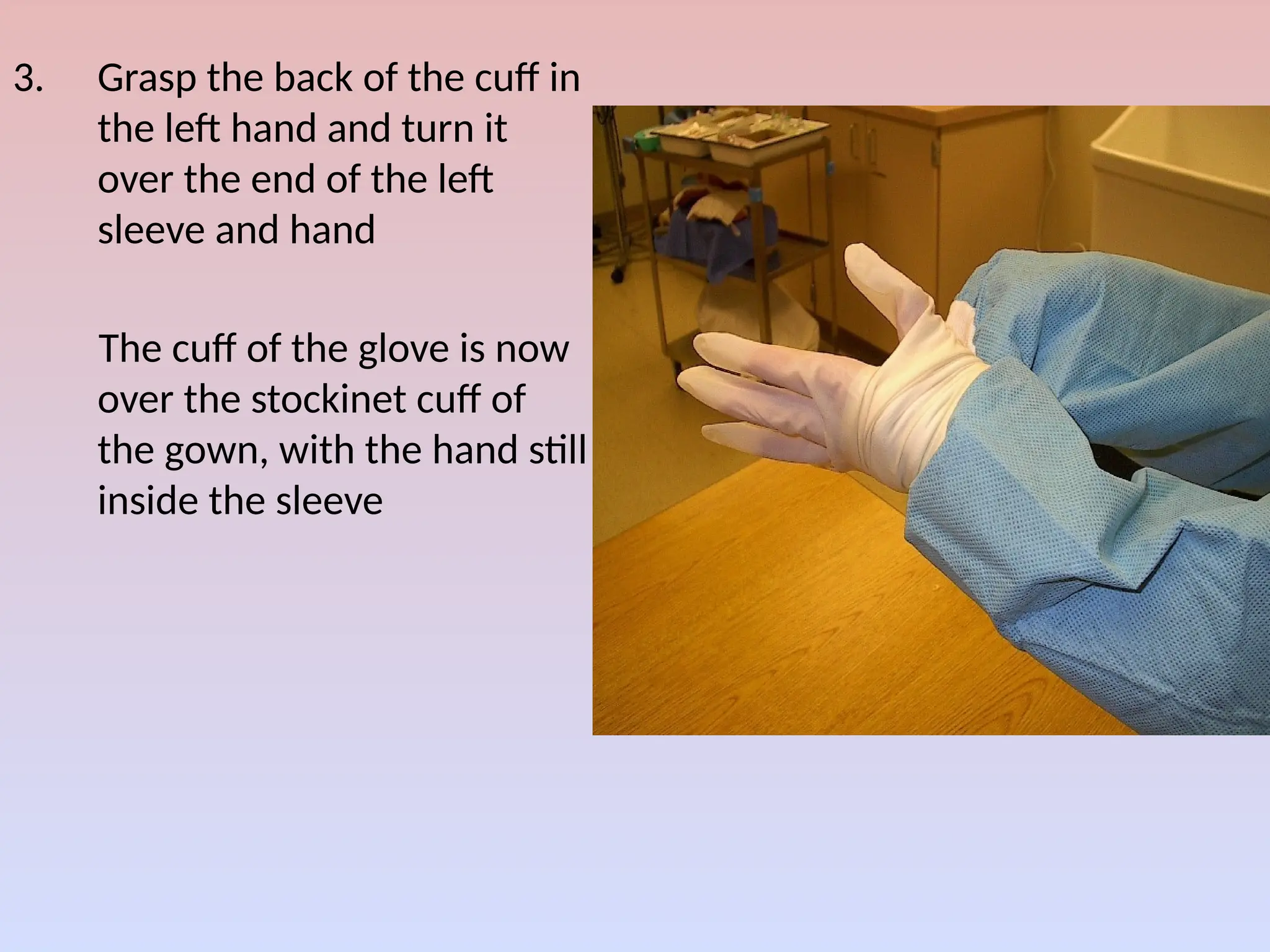
3. Grasp theback of the cuff in
the left hand and turn it
over the end of the left
sleeve and hand
The cuff of the glove is now
over the stockinet cuff of
the gown, with the hand still
inside the sleeve
63.
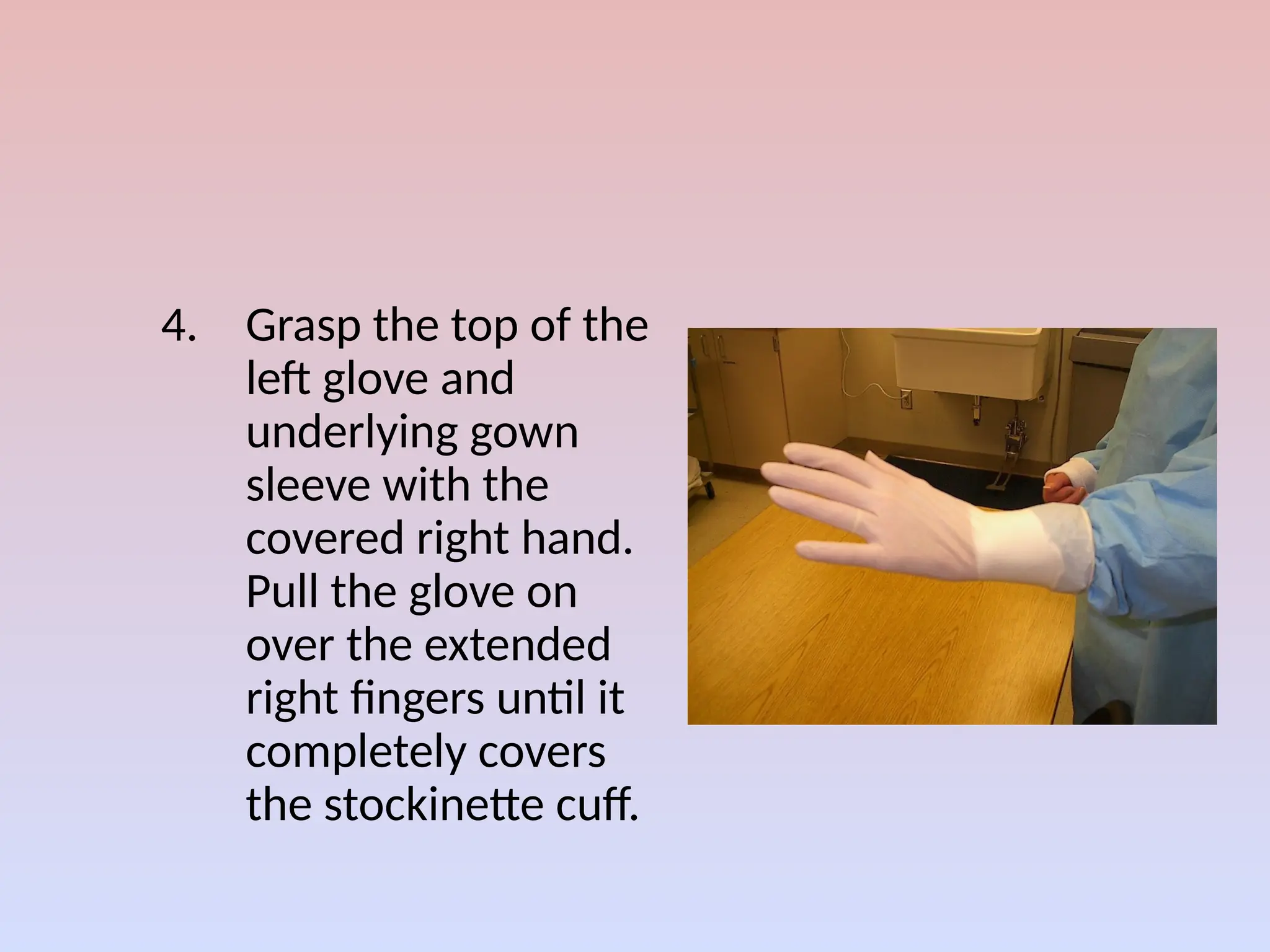
4. Grasp thetop of the
left glove and
underlying gown
sleeve with the
covered right hand.
Pull the glove on
over the extended
right fingers until it
completely covers
the stockinette cuff.
64.
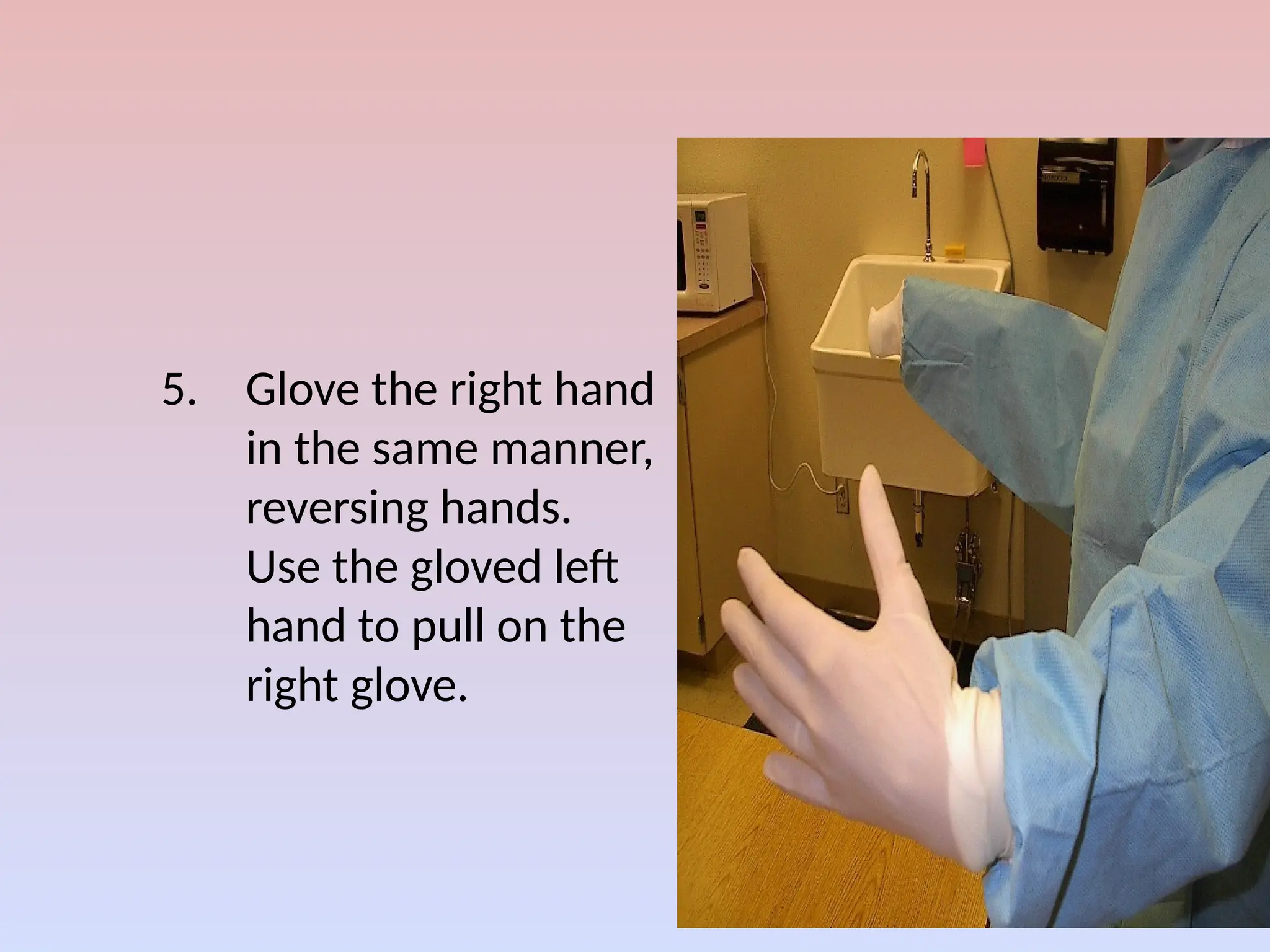
5. Glove theright hand
in the same manner,
reversing hands.
Use the gloved left
hand to pull on the
right glove.
Gloves, Gowns, Drapes
•Wearing two pairs of surgical gloves
– to provide an additional barrier and to further reduce the risk
of contamination
• The current CDC recommendation is to use surgical
gowns and drapes that resist liquid penetration and
remain effective barriers when wet
69.
Sterile Technique
• Sterileobject remains sterile only when touched by another
sterile object
• Only sterile objects may be placed on a sterile field
• A sterile object (field) out of range of vision or an object held
below a person’s waist is contaminated
• When a sterile surface comes in contact with a wet, contaminated
surface, the sterile object or field becomes contaminated by
capillary action
• The edges of a sterile field or container are considered to be
contaminated (1 inch)
70.
Surgical Principles OfAsepsis
• Know what is sterile
• Know what is not sterile
• Keep the two apart
• Remedy contamination immediately
71.
Define Sterility
• Gownsare considered sterile in front from chest high to
the operative level
• Sterile persons should keep hands in sight and keep
them at or above waist level
• Contamination occurs when sterile gown and drapes are
permeated*
• Tables are sterile only at the operative level
72.
Maintain Sterility
• Allitems used within the sterile field must be sterile
• Sterile persons touch only sterile items or sterile areas
• Articles of doubtful sterility are considered unsterile
• Unsterile personnel stay beyond one foot of the sterile field
• Every case is considered dirty and the same infection control
precautions are taken for all pts
73.
Remedy contamination immediately!!!
•When contamination occurs , take care of it
immediately
• Break in technique is pointed out and action is
taken to change situation …..change gloves
74.
Surgeon
• Most ofthe local factors that make a surgical site favorable
to bacteria are under the control of the surgeon
– Careful attention to cleanliness and technique
• Hemostasis
• sharp dissection
• fine sutures
• anatomic dissection
• gentle handling of tissues
• obliterate dead space
• Expeditious surgery(Speed and poor technique are not suitable
approaches)
• Appropriate use of electrocautery…
75.
• Drains
• Operativesite should not be drained through
the wound
• Closed suction drain… preferable
• Simple penrose drain( can also function as an
access route for pathogens
Editor's Notes
#3 Infections may be limited to the surgical site or widespread with systemic effects
#7 *Careful patient selection and preparation, including judicious use of antibiotic prophylaxis, can decrease the overall risk of infection, especially after clean-contaminated and contaminated operations
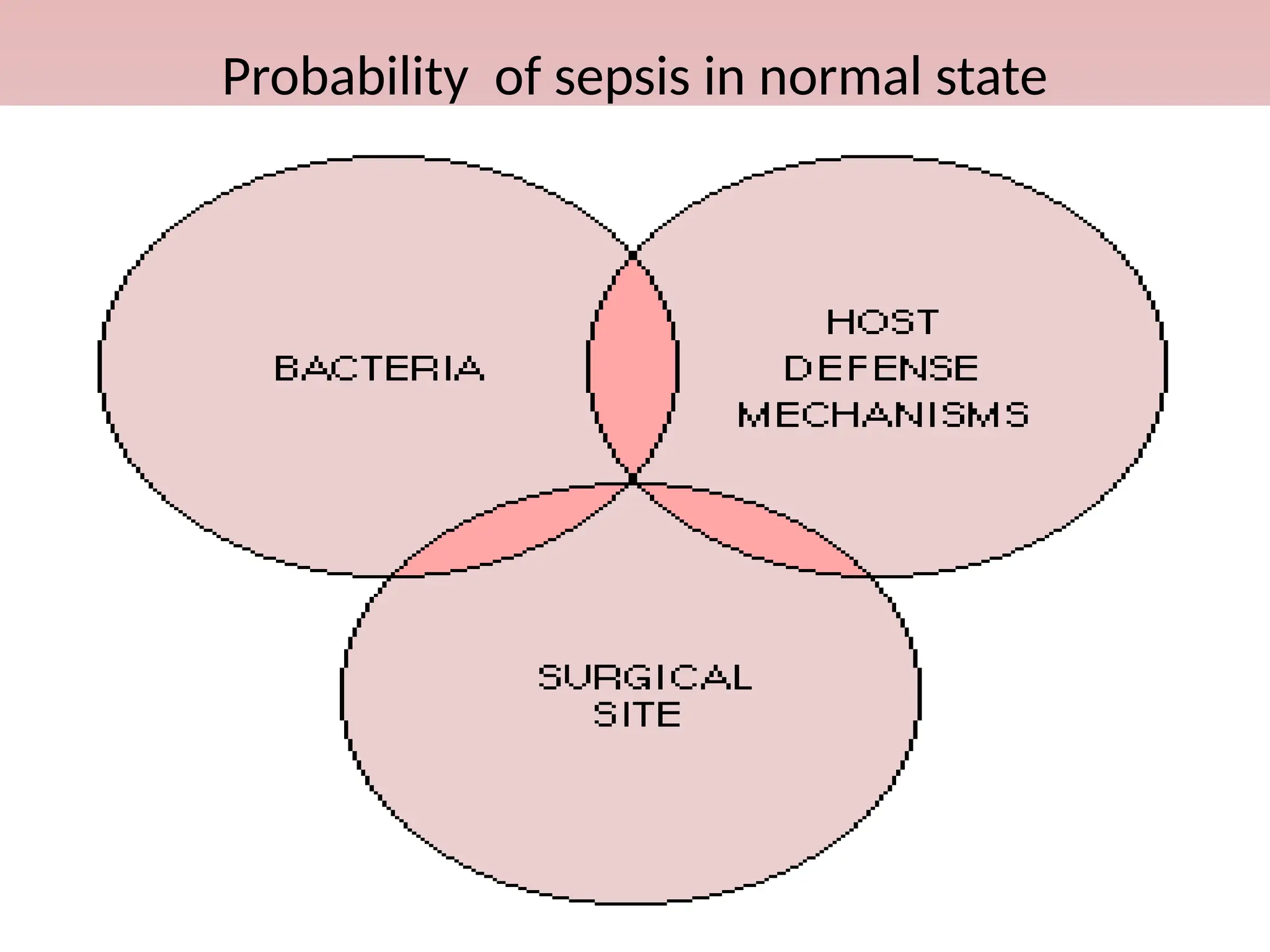
#8 Wounds are particularly appropriate for analysis of infection with respect to these three determinants. Because many components of the bacterial contribution to wound infection now are clearly understood and measures to control bacteria have been implemented, the host factors become more apparent. In addition, interactions between the three determinants play a critical role, and with limited exceptions (e.g., massive contamination), few infections will be the result of only one factor
#9 The principles of asepsis are based on rational thinking and on a strong theoretical and empirical rationale…..a common sense
#10 Aseptic techniques are practiced for all invasive medical procedures. Types of handwashing and gloves are diferrent according to the procedures performed
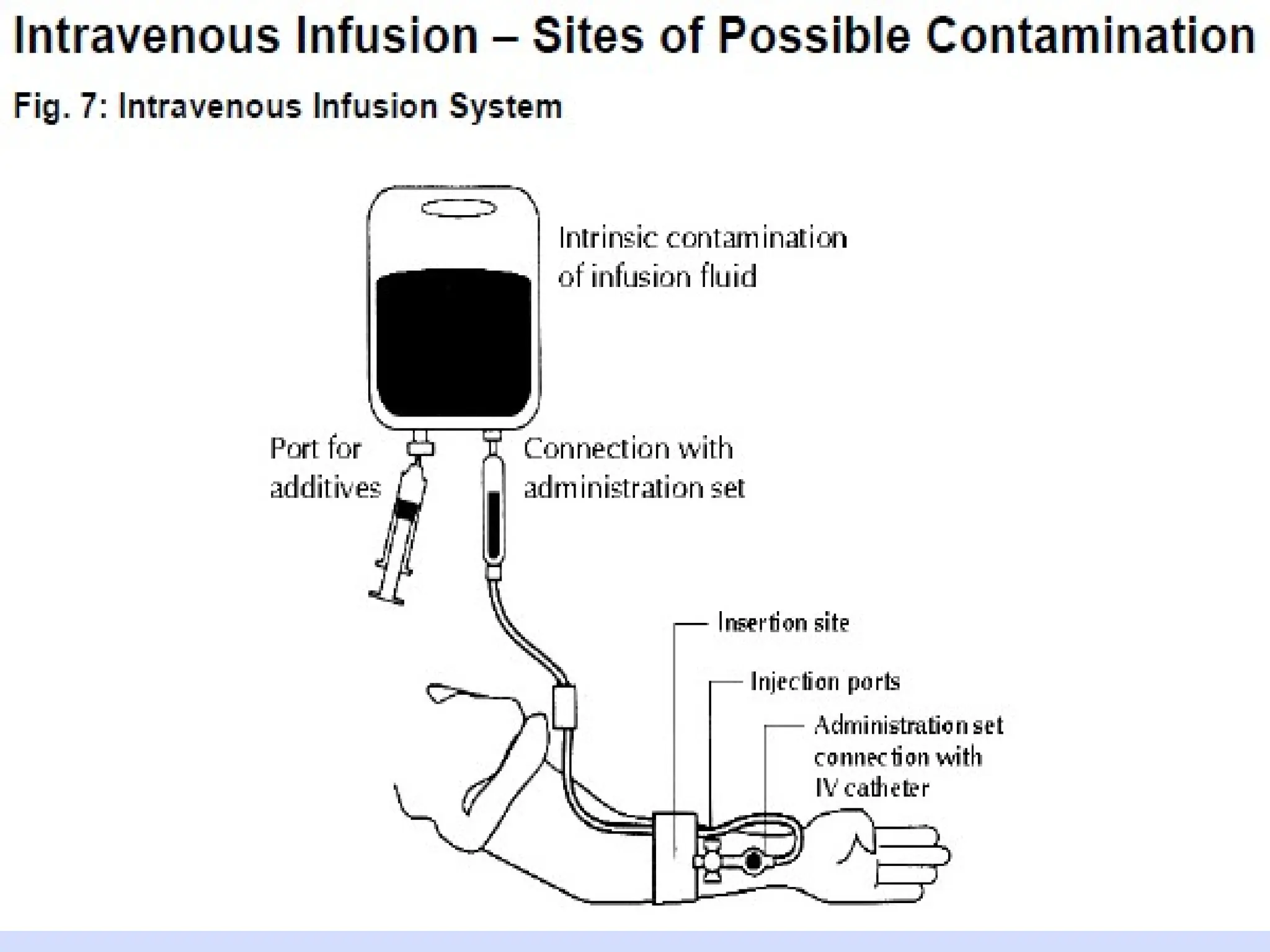
#11 Even in countries with well established infection control programmes, hospital acquired infections related to poor compliance with aseptic techniques is an impt public health problems(Eg. In USA surgical site infections are the third most frequently reported infection accounting for 14 – 16% of all hospital acquired infections….extrinsic contamination of IV fluids, reuse of needles and syringes
#12 *transient and resident flora refers to where bacteria and other organisms are located in the layers of skin. Transient flora are acquired through contact with pts, other healthcare workers or contaminated surfaces(e.g, examination tables, floors or toilets) during the course of the normal workday. These organisms live in the upper layers of the skin and are partially removed by washing with plain soap and clean water.they are the organisms most likely to cause nosocomial infections. Resident flora live in the deeper layers of the skin,as well as within hair follicles, and cannot be completely removed, even by vigorous washing and rinsing with plain soap and clean water. Fourtunately, in most cases, resident flora is less likely to be associated with infection.
Disinfectant agents used to kill or inhibit env’tal microbes
Antiseptics and disinfectants should be used according to label
#15 *general aseptic procedures as insertion of IV catheters or urinary catheters and examples of “no-touch” technique
#17 A clear policy on hand hygiene is therefore essential and should be followed by all personnel*
* Although the use of gloves reduces the transmission of bacteria, hand washing is still essential after the gloves have been taken off in order to remove any contamination that might have occurred via small punctures,and the multiplication of organisms that occurred in warm , moist env’t caused by glove wearing
#18 By minimizing contact with non-sterile surfaces or reuse of equipment and devices intended for single pt use
** this means the skin in the area of insertion should not be touched after skin antisepsis. Similarly IV administration tubing should e kept sterile and tops of vials of medication should be disinfected prior to entry
#20 *On the ward, even minimal contact with colonized patients has been demonstrated to transfer microorganisms. As many as 1,000 organisms were transferred by simply touching the patient's hand, taking a pulse, or lifting the patient
**before and after pt examination, after handling soiled instruments, after touching mucous membranes, blood or other body fluids(secretions or excretions)
Hands can be washed with soap and water or antiseptic handrub can be used
#22 The six steps of Hygienic Hand
Washing
Palm to palm
Palm to back
Finger webs
Finger tips
Thumb
Wrist
#29 *No infection, proper apparel , no jewelry, no long nails or nail polish
**no tacky mats
#39 In addition, some bacteria could be in the growth phase rather than the dormant or the lag phase and thus could be more pathogenic
** In patients with urinary tract infections, wounds frequently become infected with the same organism.
#40 *Multiple preoperative baths may prevent postoperative infection in selected pt groups,
( who carry S.aureus on their skin or who have infectious lesions)
#41 *secondary to the trauma of the shave and the inevitable small areas of inflammation and infection
**because they cause serious irritation and rashes in a significant number of patients, especially when used near the eyes and the genitalia.
#45 *The intertriginous folds and the umbilicus often require mechanical scrubbing to generate sufficient friction to remove entrapped microorganisms.
**In one study, cleansing of contaminated wounds by means of ultrasound debridement was compared with high-pressure irrigation and soaking. The experimental wounds were contaminated with a colloidal clay that potentiates infection 1,000-fold. The investigators irrigated wounds at pressures of 8 to 10 psl, a level obtained by using a 30 ml syringe with a 1.5 in long 19-gauge needle and 300 ml of 0.85% sterile saline solution. High-pressure irrigation removed slightly more particulate matter (59%) than ultrasound debridement (48%), and both of these methods removed more matter than soaking (26%).123 Both ultrasound debridement and high pressure irrigation were also effective in reducing the wound infection rate in experimental wounds contaminated with a subinfective dose of S. aureus .
#67 *Because of the invasive nature of surgery, there is a high risk of pathogen transfer during an operation, a risk from which both the patient and the surgical team must be protected
The risk can be reduced by using protective barriers, such as surgical gloves
#74 *contamination certainly increases with time, Wound edges can dry out, become macerated, or in other ways be made more susceptible to infection (i.e., requiring fewer bacteria for development of infection).; expeditious operation is appropriate.
* *electrocautery-pipoint coagulation,minimal tissue destruction, no charring, then no change in wound infection rate.
#75 *Use varies widely and is very subjective
A simple penrose drain can function not only as a drainage route but also as an access route for pathogens to the pt
It is important that the operative site not be drained through the wound. The use of a closed suction drain further reduces the potential for contamination and infection







![[Gen. surg] asepis and antisepsis from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/cl0boxvgty2rybxdgdhl-signature-488639c0f2ed9772258765aac732a52dc3089a746e9bf5544a488c47cab4cc69-poli-150813092039-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
































































