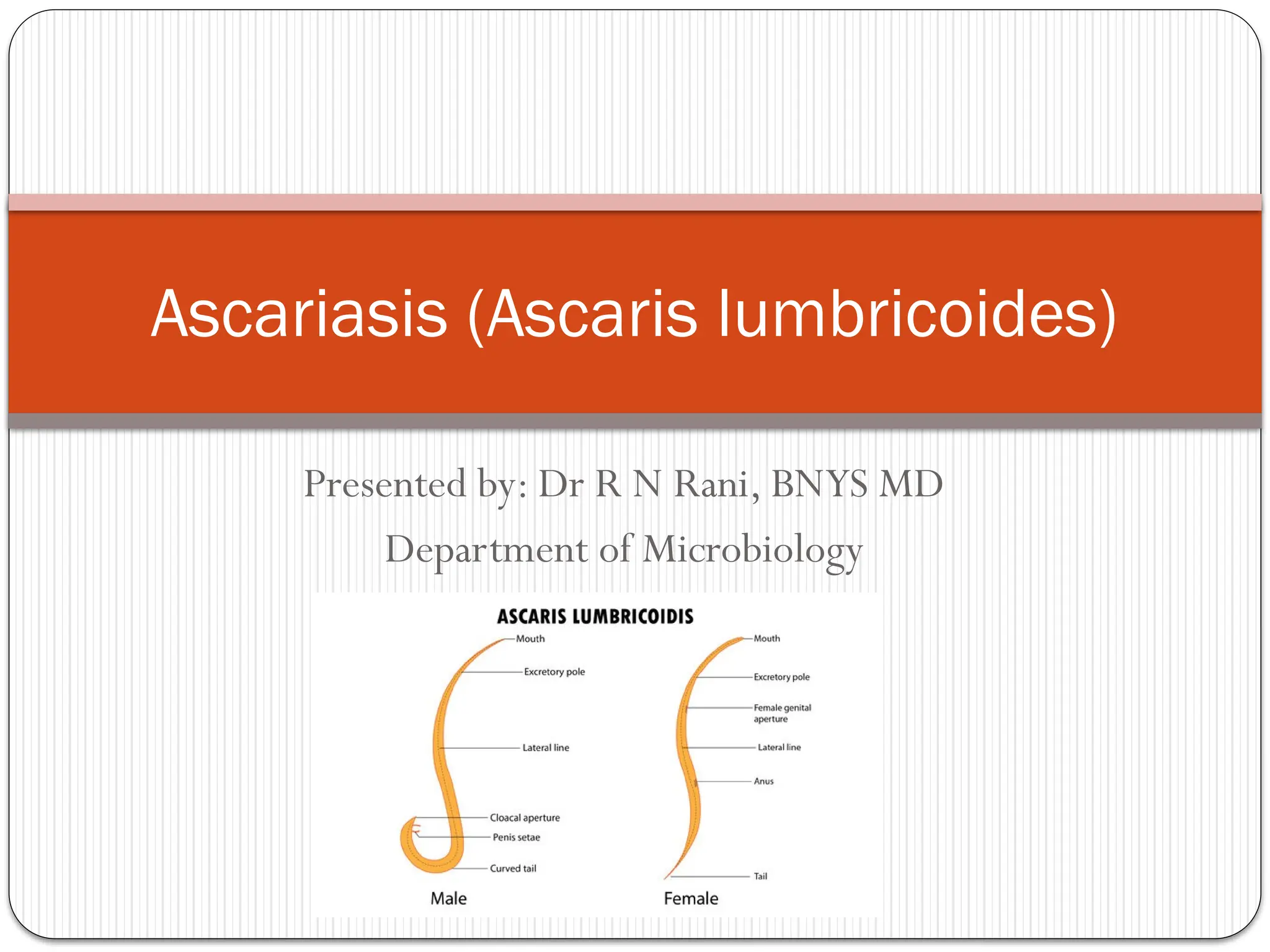
Presented by: DrR N Rani, BNYS MD
Department of Microbiology
Ascariasis (Ascaris lumbricoides)
2.
Introduction
Ascariasis isan intestinal infection caused by the roundworm
Ascaris lumbricoides.
It is one of the most common helminthic infections,
especially in tropical and subtropical regions.
Transmission occurs via ingestion of infective eggs through
contaminated food or water.
3.
Taxonomy and Morphology
Phylum: Nematoda
Class: Secernentea
Order:Ascaridida
Genus:Ascaris
Species: lumbricoides
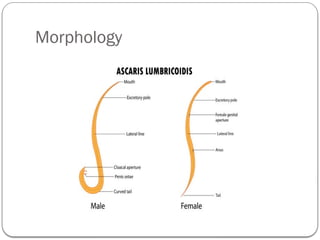
Adult worms are large, creamy-white, cylindrical worms.
Males: 15–30 cm long with curved posterior end.
Females: 20–35 cm long.
Eggs: Fertilized and unfertilized types with thick shell and
mammillated surface.
Distribution and Epidemiology
• Common in tropical and subtropical areas with poor
sanitation.
• More prevalent among children.
• Transmission via fecal contamination of soil, food, and
water.
• Eggs can survive in moist soil for years.
6.
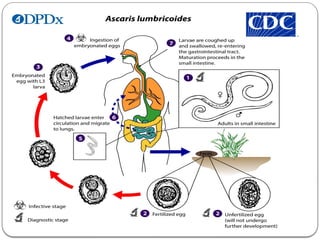
Life Cycle
1.Infective eggs are ingested.
2. Larvae hatch in intestine and migrate via bloodstream to
lungs.
3.After maturation in lungs, larvae ascend trachea, are
swallowed, and mature into adults in intestine.
4. Females produce thousands of eggs passed in feces.
Total cycle duration: 60–75 days.
8.
Pathogenesis and ClinicalFeatures
• Light infections: Often asymptomatic.
• Heavy infections:Abdominal pain, malnutrition, growth
retardation.
• Pulmonary phase: Cough, eosinophilia (Löffler’s
syndrome).
• May cause intestinal obstruction in children.
9.
Complications
• Intestinalobstruction (especially in children)
• Biliary or pancreatic duct obstruction
• Appendicitis or perforation due to migration
• Nutritional deficiency due to malabsorption.
Laboratory Diagnosis
•Stool microscopy: Detection of characteristic eggs.
• Concentration techniques (Kato-Katz, formalin-ether).
• Imaging: Ultrasonography or X-ray in complications.
• Serology rarely needed.
12.
Treatment
• Albendazole400 mg single dose (preferred)
• Mebendazole 100 mg twice daily for 3 days
• Pyrantel pamoate as an alternative.
• Treat all family members simultaneously.
13.
Prevention and Control
• Improve sanitation and hygiene.
• Proper disposal of feces.
• Washing of vegetables and fruits.
• Regular deworming in endemic areas.
• Health education to communities.
14.
Summary
• Ascariasisis caused by Ascaris lumbricoides.
• Transmitted by ingestion of embryonated eggs.
• Life cycle involves larval migration through lungs.
• Diagnosis by stool microscopy.
• Prevention: Sanitation and deworming programs.
15.
References
1. Paniker’sTextbookof Medical Parasitology, 8th Ed.
2. CDC – Ascariasis Fact Sheet.
3.WHO Guidelines for Control of Soil-transmitted
Helminths.

































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















