Downloaded 34 times





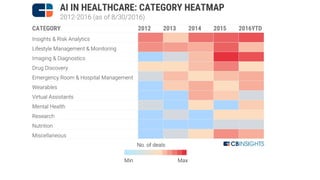
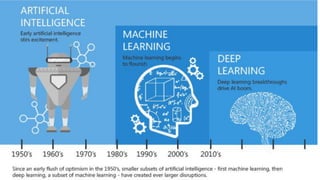

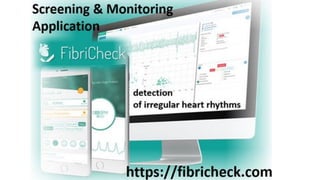
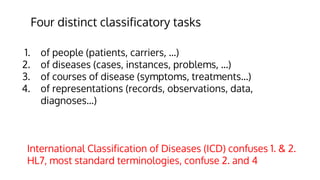


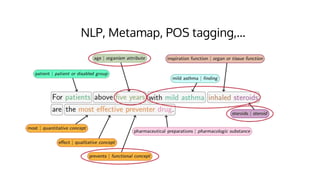
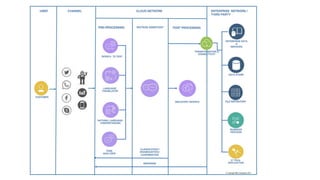
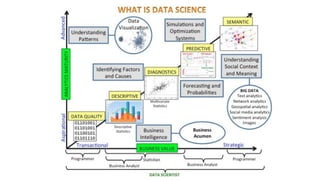
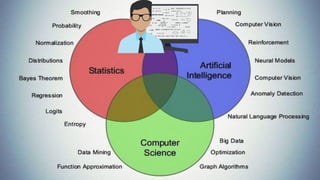

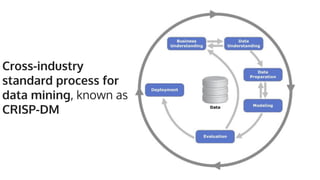











This document discusses the potential for artificial intelligence and machine learning in medicine. It notes that while 80% of healthcare data remains unstructured, machine learning could help analyze this data by mapping and validating data fields for modeling. However, significant preprocessing is required due to limitations in available data sets and variables. The document also discusses challenges including different classifications for patients, diseases, and representations in records. It provides an example of a study using clinical notes to predict acute kidney injury. Overall, the document outlines both the promise and challenges of applying artificial intelligence and machine learning to healthcare data.









































![[台灣人工智慧學校] 開創台灣產業智慧轉型的新契機](https://cdn.slidesharecdn.com/ss_thumbnails/aiinhealthcare-20190216victoria-v6-190227081004-thumbnail.jpg?width=640&height=640&fit=bounds)























