3
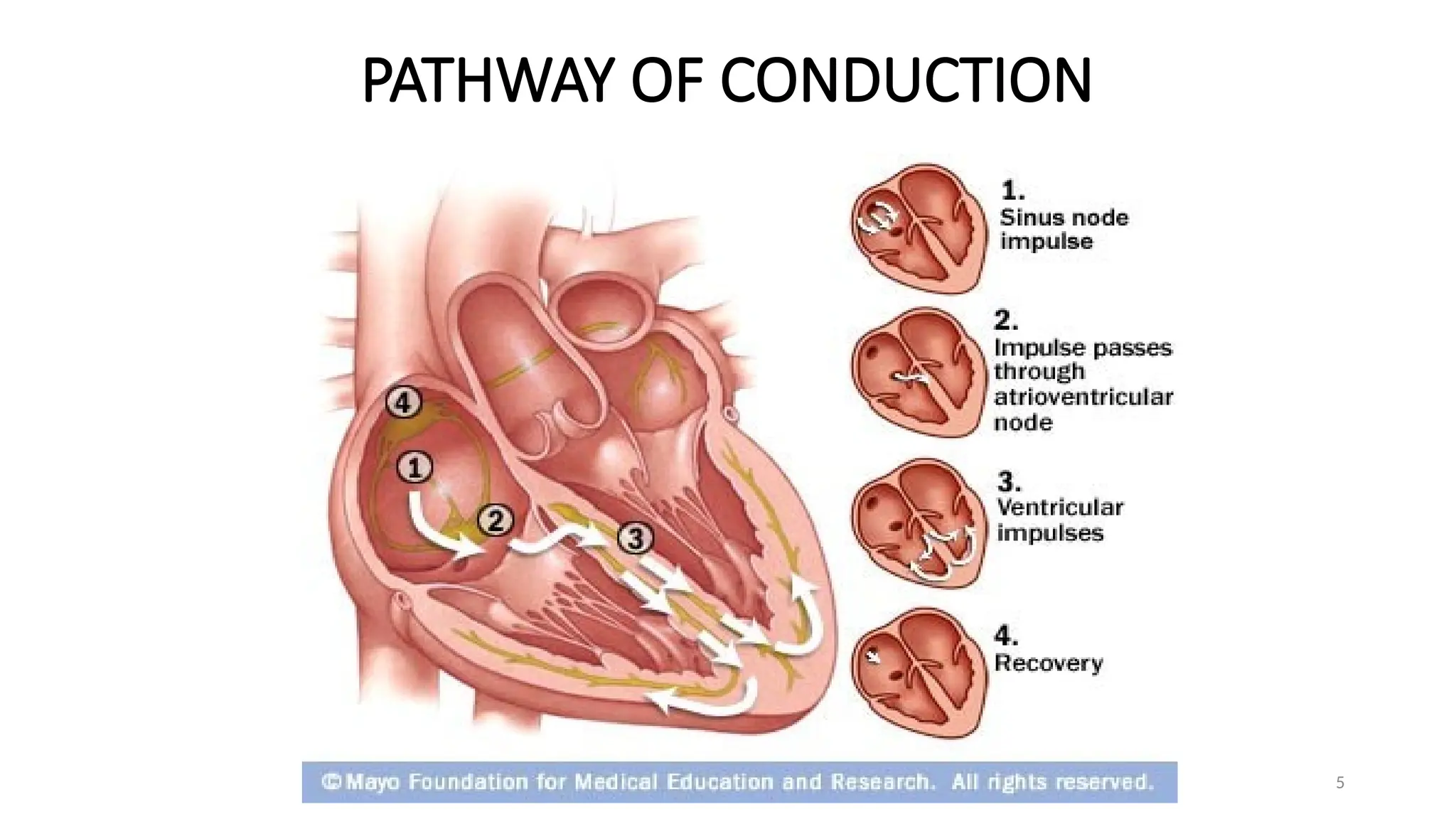
Introduction Normal cardiacfunction relies on the flow of
electric impulses through the heart in an
exquisitely coordinated fashion.
This pathway is made up of 5 elements:
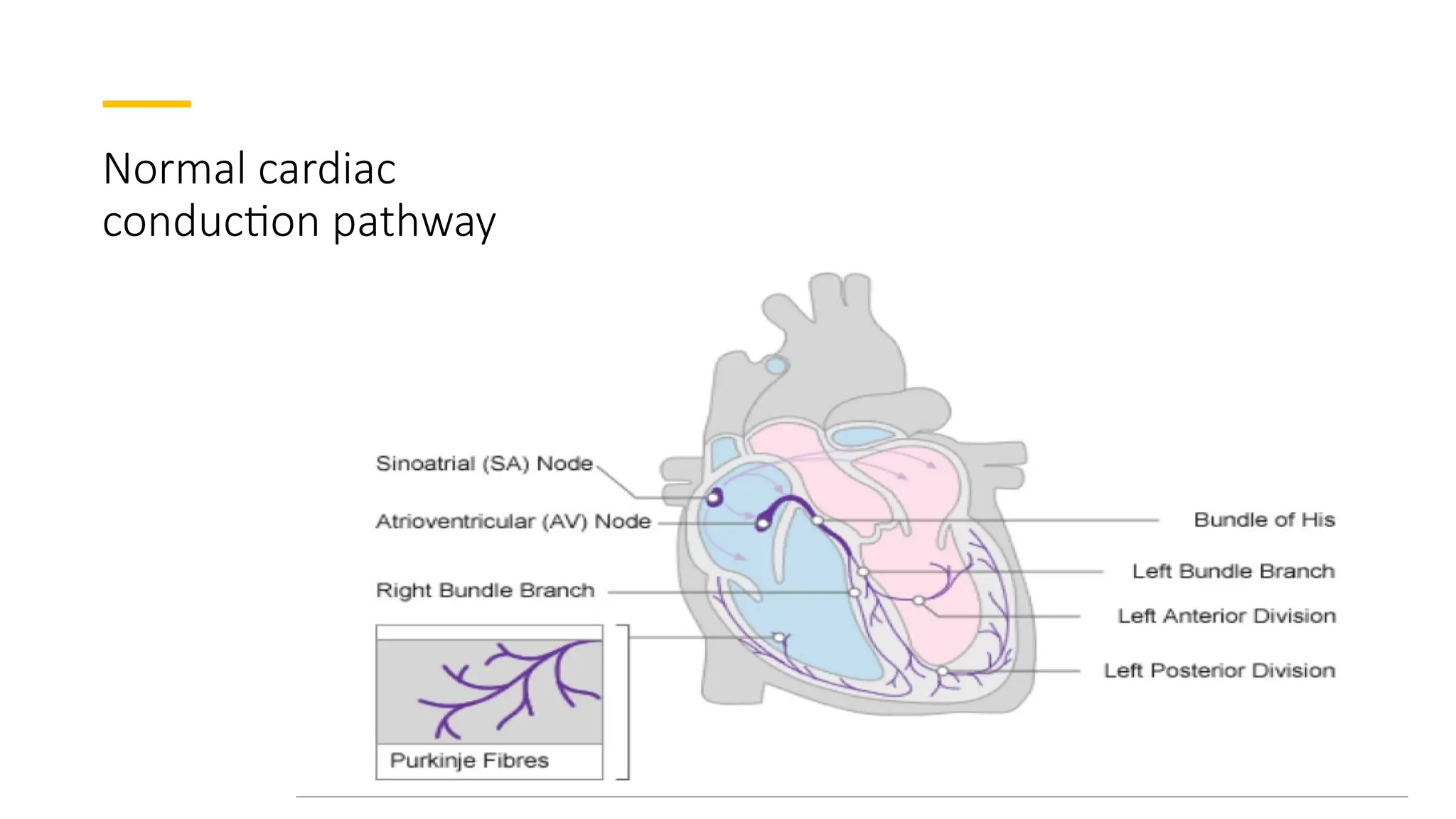
1.The sino-atrial (SA) node
2.The atrioventricular (AV) node
3.The bundle of His
4.The left and right bundle branches
5.The Purkinje fibres
6
Arrhythmia 1 •Disorders of heart rhythm resulting from alterations of
impulse formation, impulse conduction, or both.
• Cardiac arrhythmia (or dysrhythmia) describes any
abnormality of cardiac rhythm.
• Arrhythmias may cause sudden death, syncope, heart
failure, dizziness, palpitations or no symptoms at all.
Broadly divided into two
• Slow heart rhythms are termed bradycardias (or
bradyarrhythmias).
• Fast rhythms are known as tachycardias (or
tachyarrhythmias).
7.
7
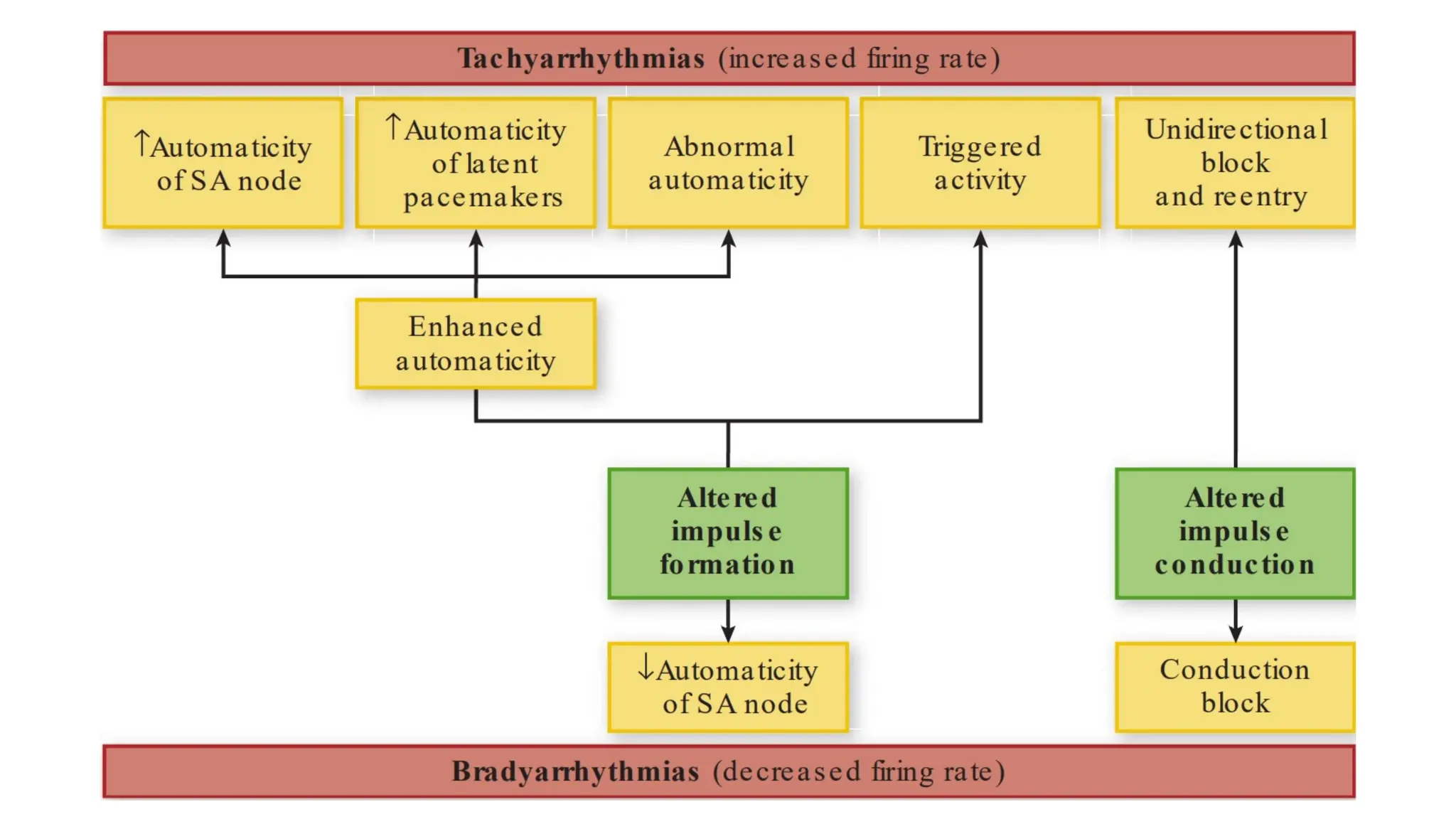
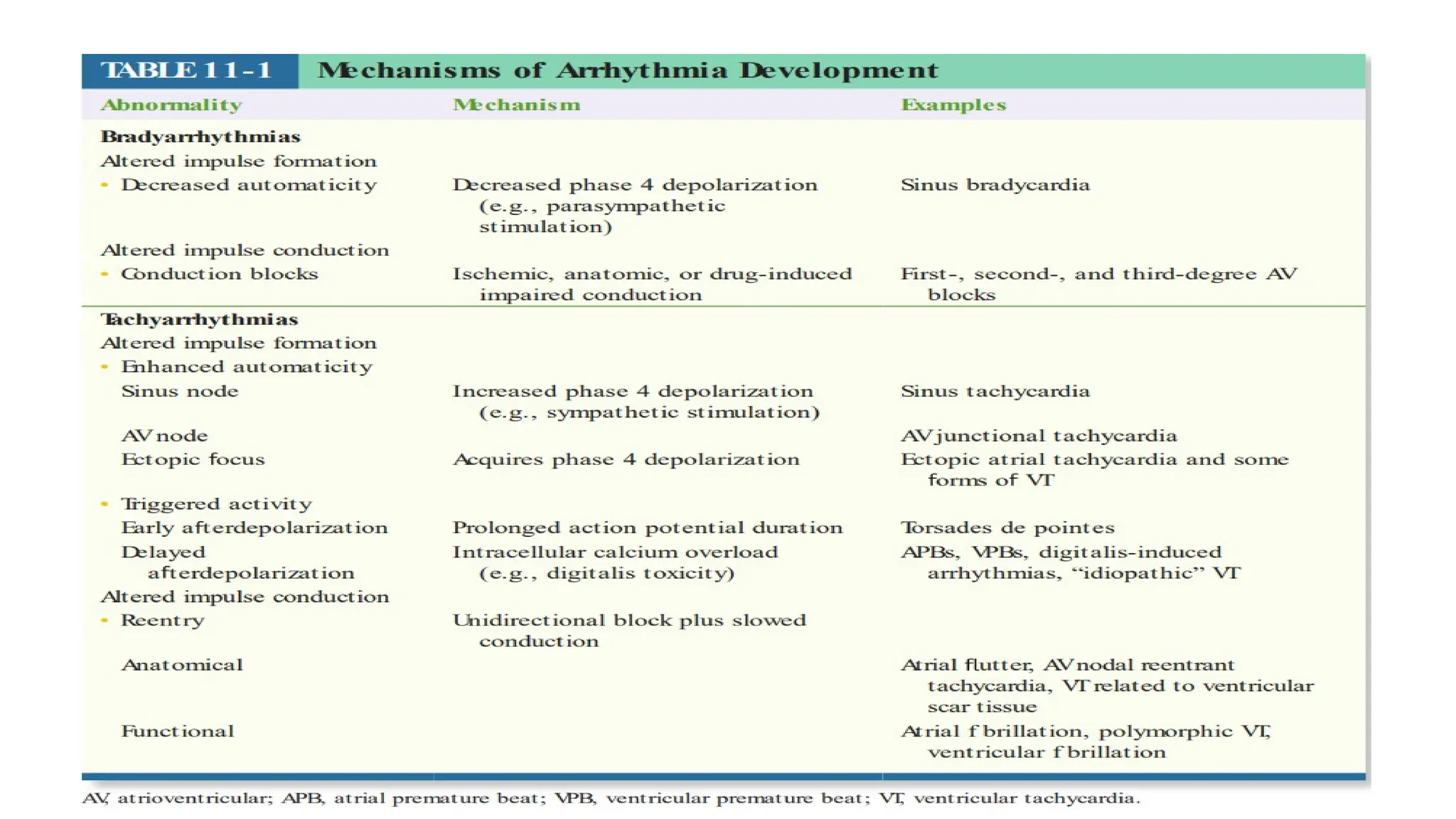
Arrhythmia Bradyarrhythmias resultfrom decreased
automaticity or conduction block.
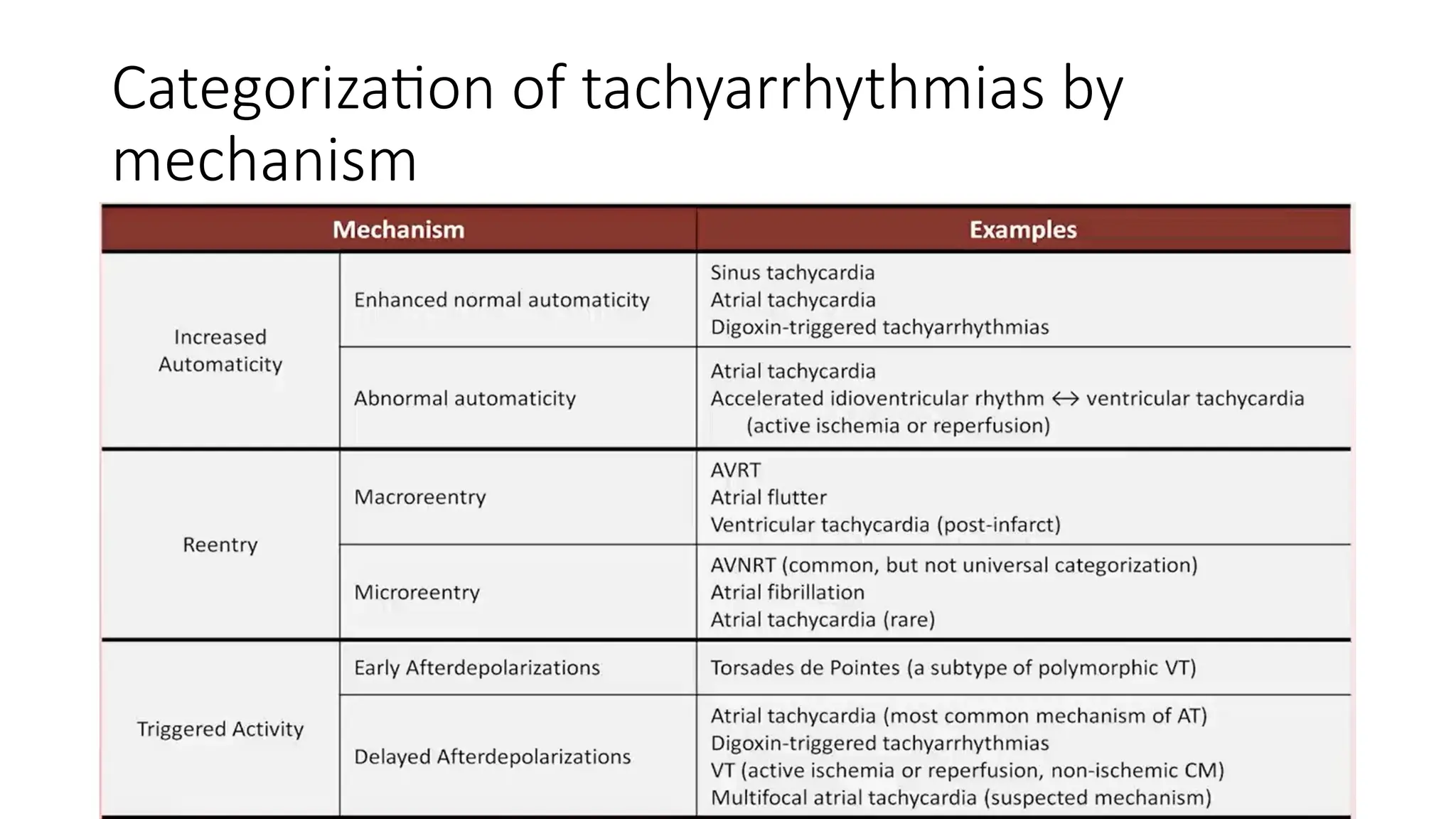
Tachyarrhythmias result from enhanced
automaticity, reentry, or triggered activity.
Tachycardias are further characterized
1. Supraventricular when they involve the
atrium or atrioventricular (AV) node.
2. Ventricular when they originate from the
His–Purkinje system or ventricles.
8.
8
Cardiac excitation-contraction coupling
•Describes the physiological process by which electrical stimulation of
the cardiomyocytes (the action potential) results in a mechanical
response (muscle contraction).
• The contraction of a cardiac myocyte is governed primarily by
intracellular Ca2+
concentration.
9.
Myocardial
action
potential
9
The cardiac actionpotential results from
the sequential opening & closing of ion
channels that span the plasma
membrane of individual myocytes.
Its conduction through the heart depends
on electrical coupling between these
cells, which is mediated by gap junctions.
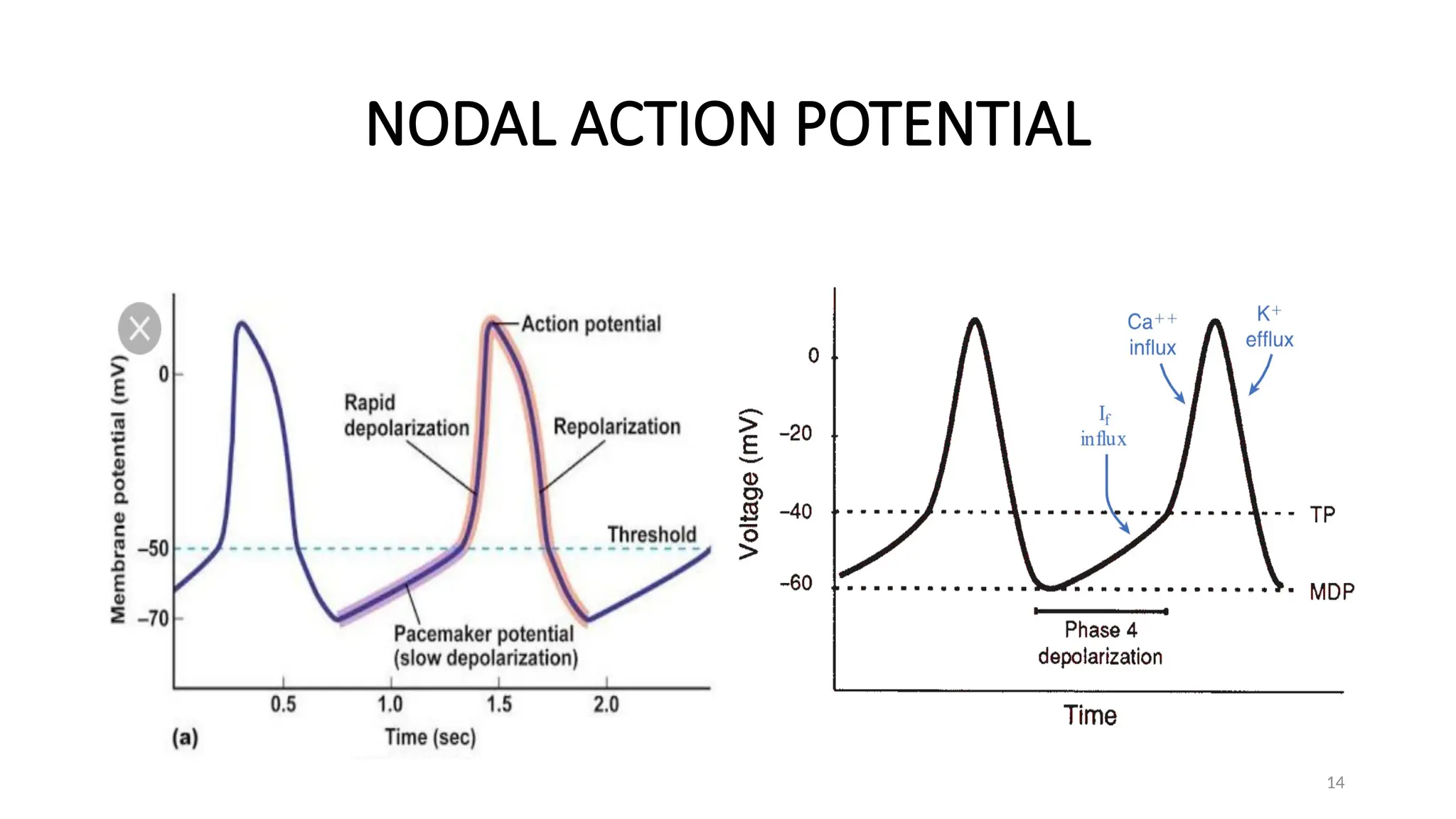
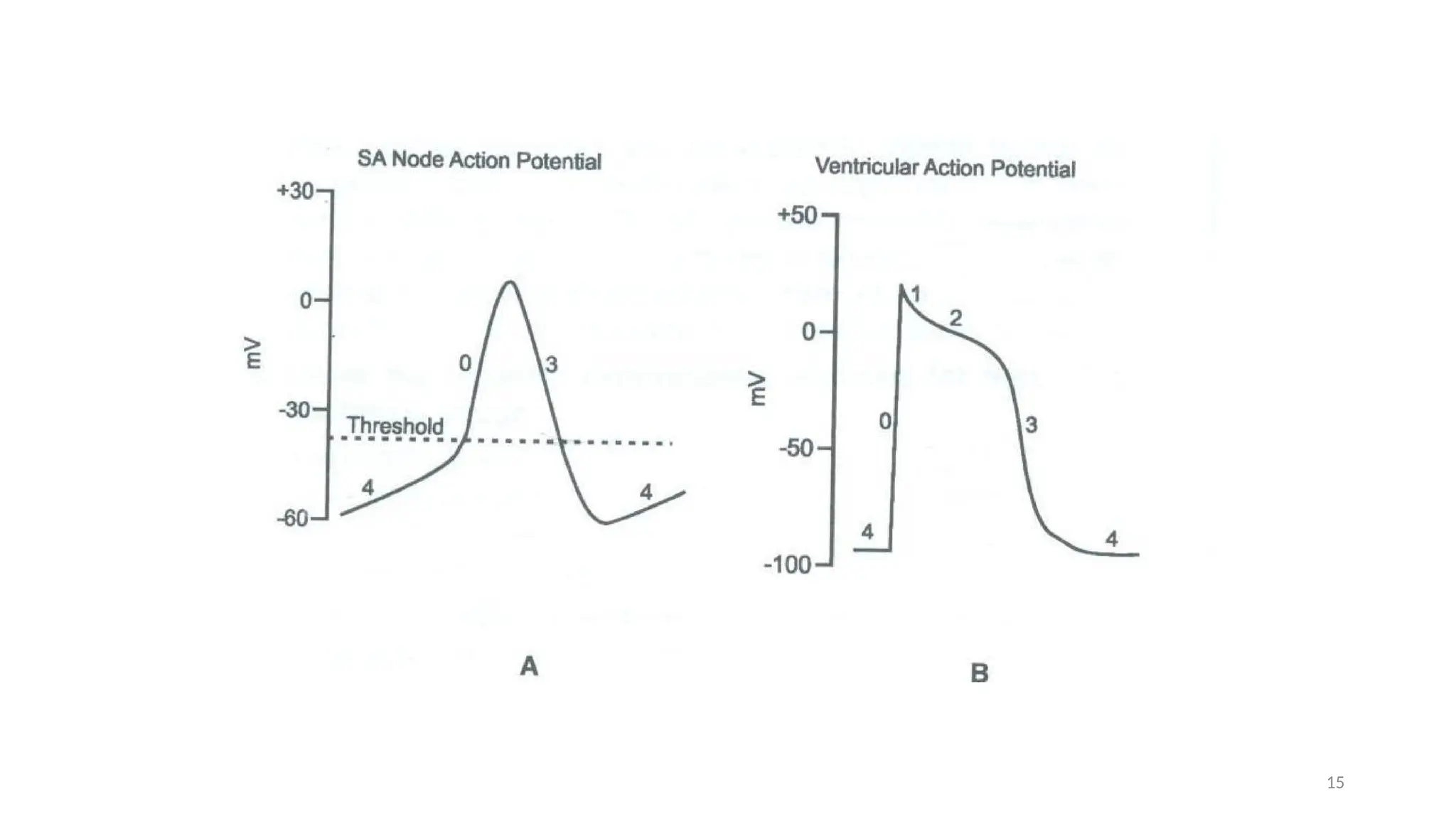
5 phases (from 0 to 4)
Cardiac action
potential
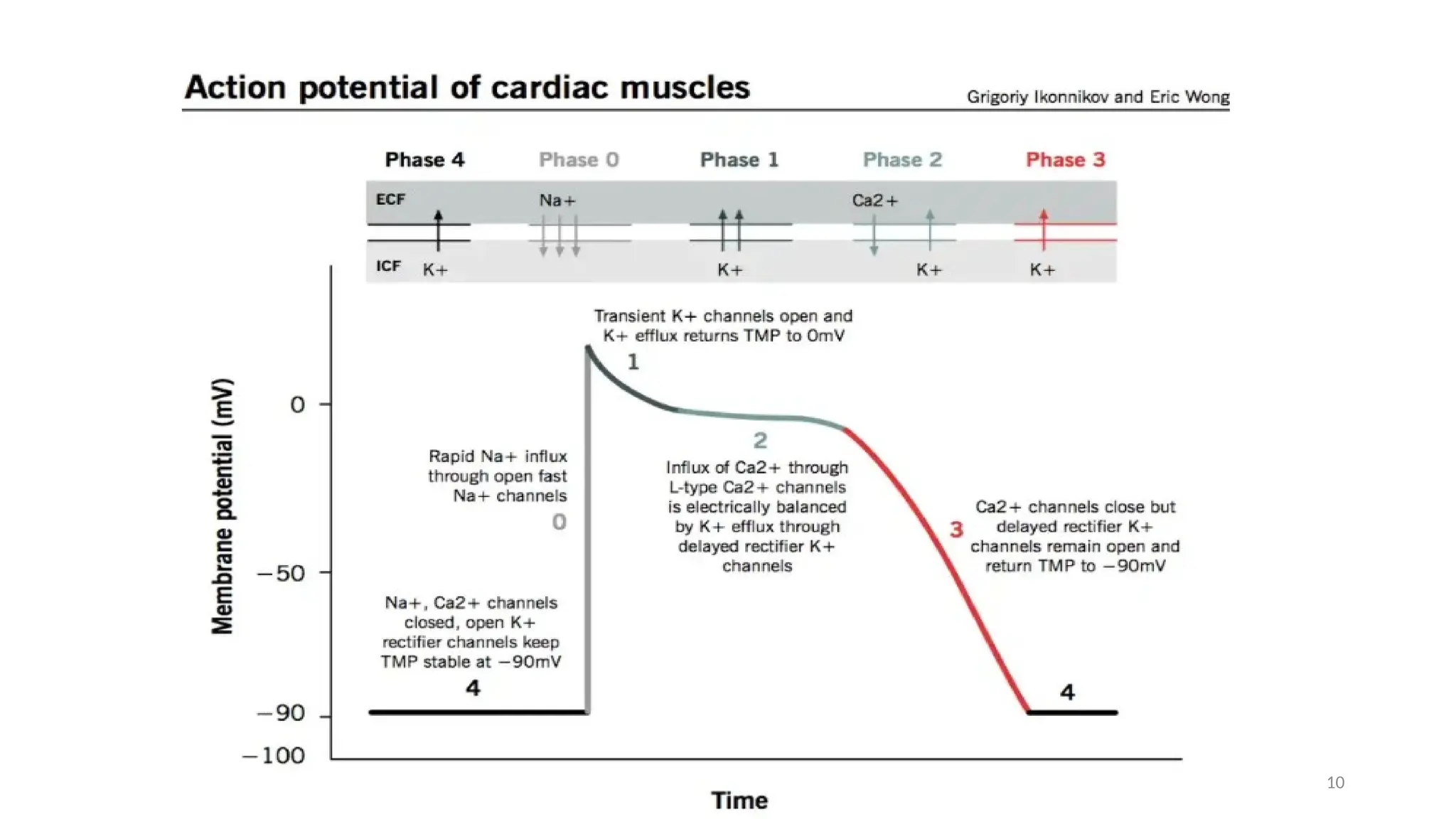
• Phase0 - depolarization from the SA node brings the
membrane potential to the threshold, opening voltage-
activated sodium channels.
• Phase 1 - early rapid repolarization then results from the
activation of the fast and slow transient outward
potassium currents
• Phase 2 - prolonged plateau resulting from a balance
between the inward currents mediated by the L-type
Ca2+
channel and Na+
–Ca2+
exchanger and outward
currents mediated by delayed rectifier K+
channels
11
12.
Cardiac action
potential
• Phase3 - Calcium channels become inactivated;
outward potassium currents predominate further
repolarization membrane potential moves
towards the potassium equilibrium potential.
• Phase 4 - Membrane potential returns to its resting
value after full repolarization (-90mV)
• The repolarization phase of pacemaker cells results
from both the inactivation of the open calcium
channels and the opening of voltage-gated
potassium channels that permit the efflux of
potassium from the cells.
• The resting state is maintained mainly by K+
inward
rectifier current & weak inward rectifying ATP-
dependent K+
channels
12
13.
13
Cardiac action potentials
•The distinct populations of automatic cells in the specialized
conduction pathway have different intrinsic rates of firing.
• These rates are determined by three variables that influence how fast
the membrane potential reaches the threshold condition:
(1) Rate (i.e., the slope) of phase 4 spontaneous depolarization
(2) Maximum negative diastolic potential
(3) The Threshold potential
Cardiac Arrhythmia •Cardiac tissue is composed of electrically
coupled cells operating as a syncytium.
• As myocytes depolarize and the electrical
activity rapidly propagates from one cell to the
next with minimal resistance, spreading
through a large mass of tissue.
• Electrical impulse formation in the heart arises
from the intrinsic automaticity of specialized
cardiac cells.
• Automaticity refers to a cell’s ability to
spontaneously depolarise to a threshold
voltage to generate an action potential.
16
17.
Cardiac Arrhythmia •The cells of the specialized conducting system
do possess natural automaticity and are
therefore termed pacemaker cells.
• The specialized conducting system includes
the sinoatrial (SA) node, the AV nodal region,
and the ventricular conducting system.
• The latter comprises the bundle of His, the
bundle branches, and the Purkinje fibres.
• Although atrial and ventricular myocytes do
not have this property under normal
conditions, In pathologic situations, they may
also acquire automaticity
17
18.
18
Pacemakers: sinoatrial node(SA node) and atrioventricular node (AV node)
Normally, SA node is the dominant pacemaker (sinus rhythm) at a rate of 60-
100bpm
Subsidiary (latent) pacemakers – AV node (40-60bpm), Purkinje fibres (20-40bpm)
SA node suppresses other subsidiary pacemakers cells by overdrive suppression
Pacemakers of the heart
Pathophysiology
• The hearthas intrinsic pacemaker activity
• SAN depolarizes more rapidly than other cells in
Conducting System
• Cardiac myocytes are excitable cells
• Rate of depolarization is dependent on:
location, autonomic, pathologic & pharmacologic states of
the cells
20
21.
21
Pathophysiology
Abnormalities of Cardiacconducting system & cardiac muscles
can predispose to loss of membrane potential → arrhythmias
Acquired or inherited abnormalities in sarcoplasmic reticulum
(SR) Ca release channels &/or SR Ca-binding proteins
Abnormal milieu eg hyperkalemia
22.
22
Pathophysiology
Neural changes maycreate electrical instability
Alteration in vagal & sympathetic innervation → arrhythmia
Damage to nerves extrinsic to heart eg stellate ganglia
Intrinsic cardiac nerves dx eg, viral infections
Secondary to dx that causes cardiac damage → Cardioneuropathy
25
Automaticity
Describes the propertyof some cardiac myocytes to undergo
spontaneous depolarization initiating an electrical impulse.
It occurs due to increasing the rate of diastolic depolarization or
changing the threshold potential.
Abnormal automaticity can occur in virtually all cardiac tissues and
may initiate arrhythmias.
Such changes are thought to produce sinus tachycardia, escape
rhythms and accelerated AV nodal (junctional) rhythms.
26.
26
Mechanisms of cardiacarrhythmia
Abnormal automaticity is defined as an inappropriate increase in the rate of discharge of
a tissue that has physiological pacemaker properties (sinus node, AV node, or Purkinje
fibres) or the pathological development of automaticity in atrial or ventricular myocytes.
Such abnormalities are most commonly seen in the presence of ischaemia, sympathetic
stimulation, or drug toxicity, especially digoxin.
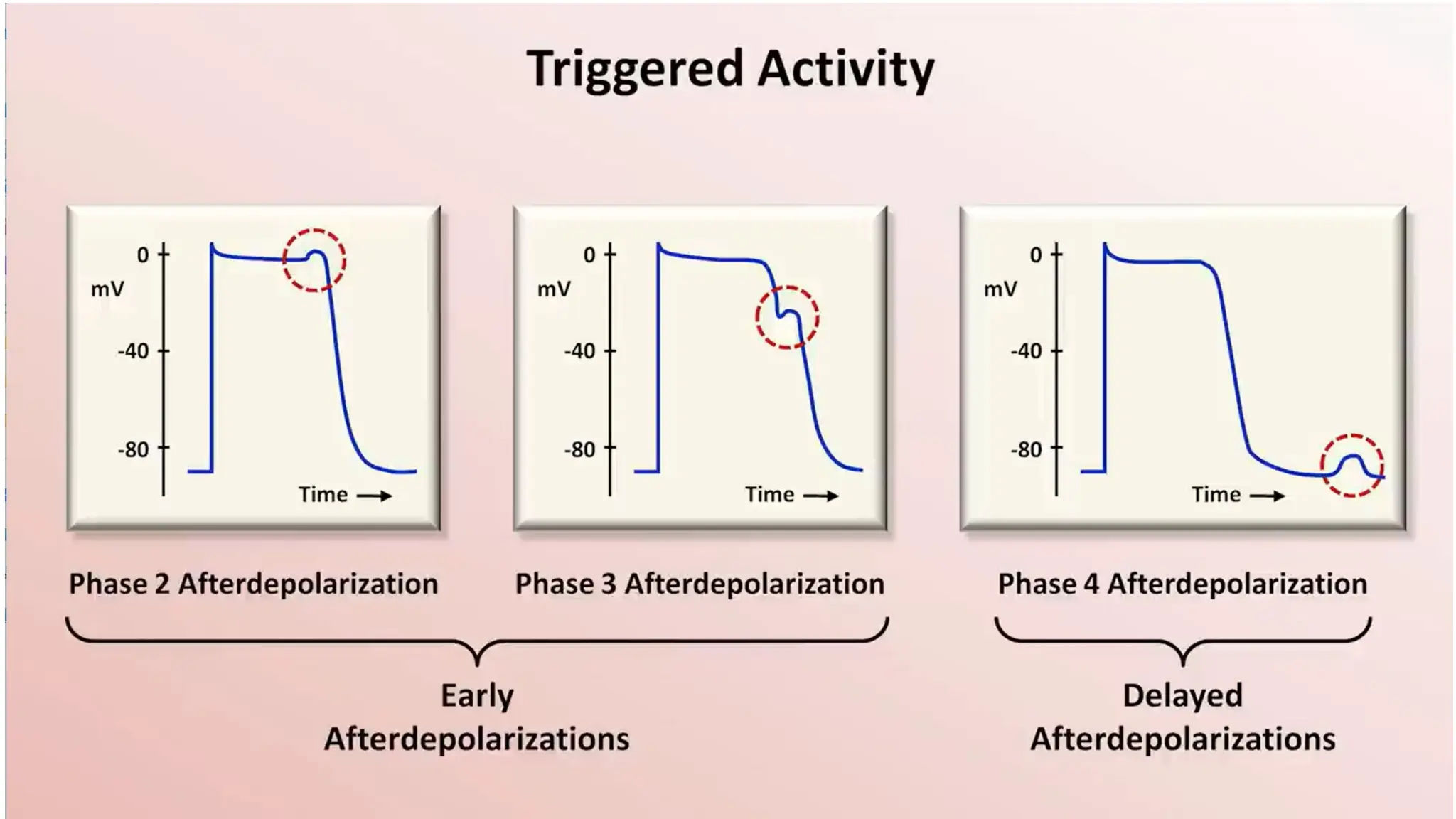
Triggered
Activity
• Occurs when
depolarizingoscillations
of the membrane
potential occur during or
after an action potential
in which one oscillation
is strong enough to
trigger a new potential.
• These oscillations are
called
afterdepolarizations
31
32.
32
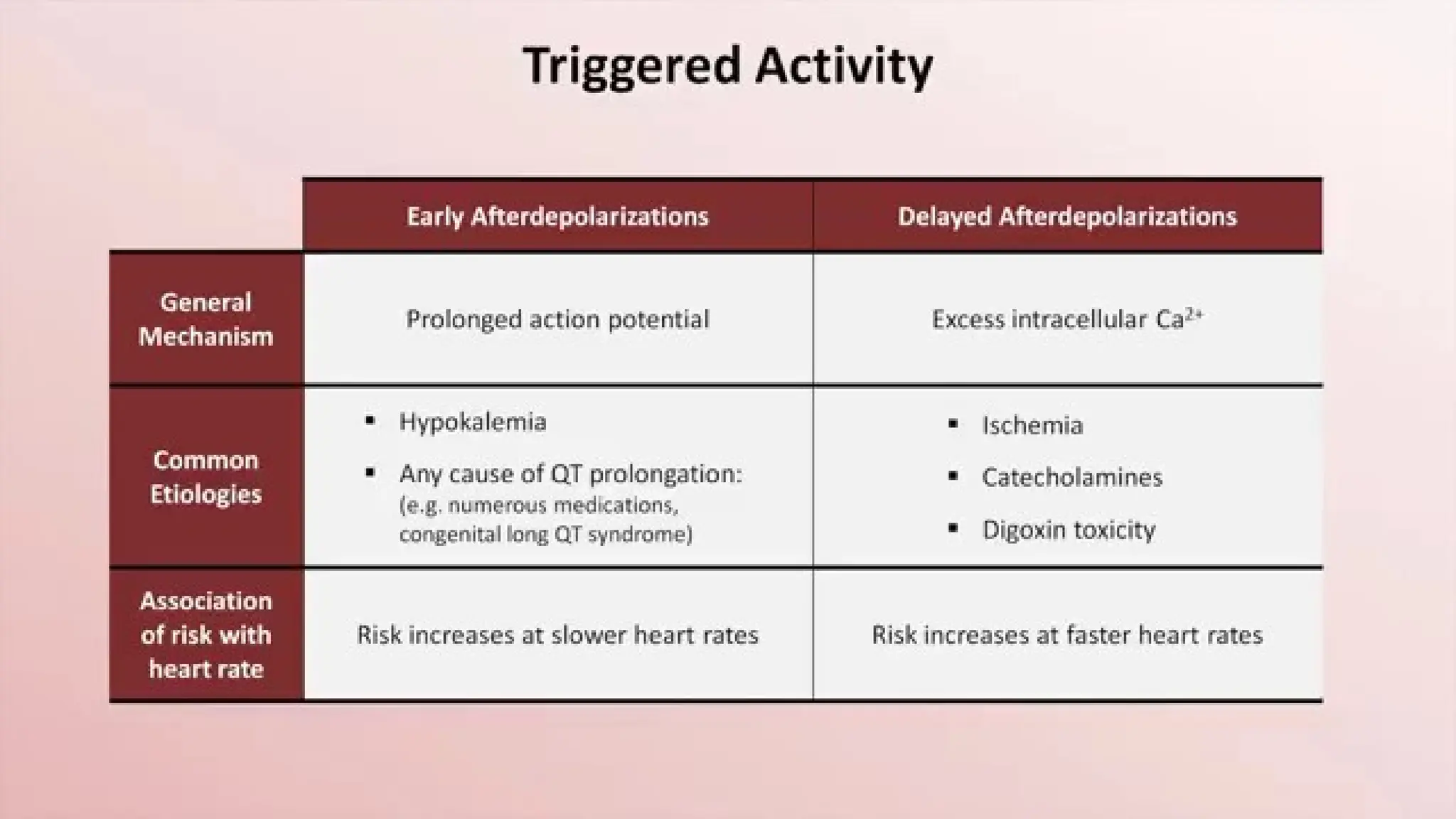
Triggered activity
Under certainconditions, an action potential can trigger abnormal depolarizations that result in extra
heartbeats or tachyarrhythmias.
A preceding action potential stimulates this type of automaticity.
There are two types of afterdepolarizations depending on their timing after the inciting action potential.
Early afterdepolarizations (EAD) occur during the repolarization phase of the inciting beat
Delayed afterdepolarizations(DAD) occur shortly after repolarization has been completed.
In either case, abnormal action potentials are triggered if the afterdepolarization reaches a threshold voltage
Early after depolarization
•EAD occur during the plateau phase of the action potential, prior to repolarization, and
are more evident at slow heart rates, particularly in the presence of hypokalaemia and
hypomagnesaemia.
• Mutations in cardiac Na+ or K+ channels, or drugs that prolong myocardial repolarization
by inhibiting one or more components of the outward potassium current, IK, (class IA and
class III antiarrhythmics, tricyclic antidepressants, antihistamines, organophosphorus
insecticides, and many others) can predispose to the appearance of early after-
depolarizations.
34
35.
35
Delayed after depolarization
•These are subthreshold depolarisations occurring after full repolarization of the action
potential.
• Their amplitude is increased by tachycardia or intracellular calcium overload and may
reach a threshold at which an action potential is generated, potentially initiating
sustained tachycardia.
• Delayed after-depolarizations can be induced experimentally by digitalis overload and are
the likely mechanism of digitoxic arrhythmias.
37
Reentry
An electric impulsecirculates repeatedly around a reentry path,
recurrently depolarizing a region of cardiac tissue.
It occurs when an electrical impulse does not cease at the end of one
cardiac cycle but rather persists and re-excites the heart as part of a
self-propagating mechanism.
38.
38
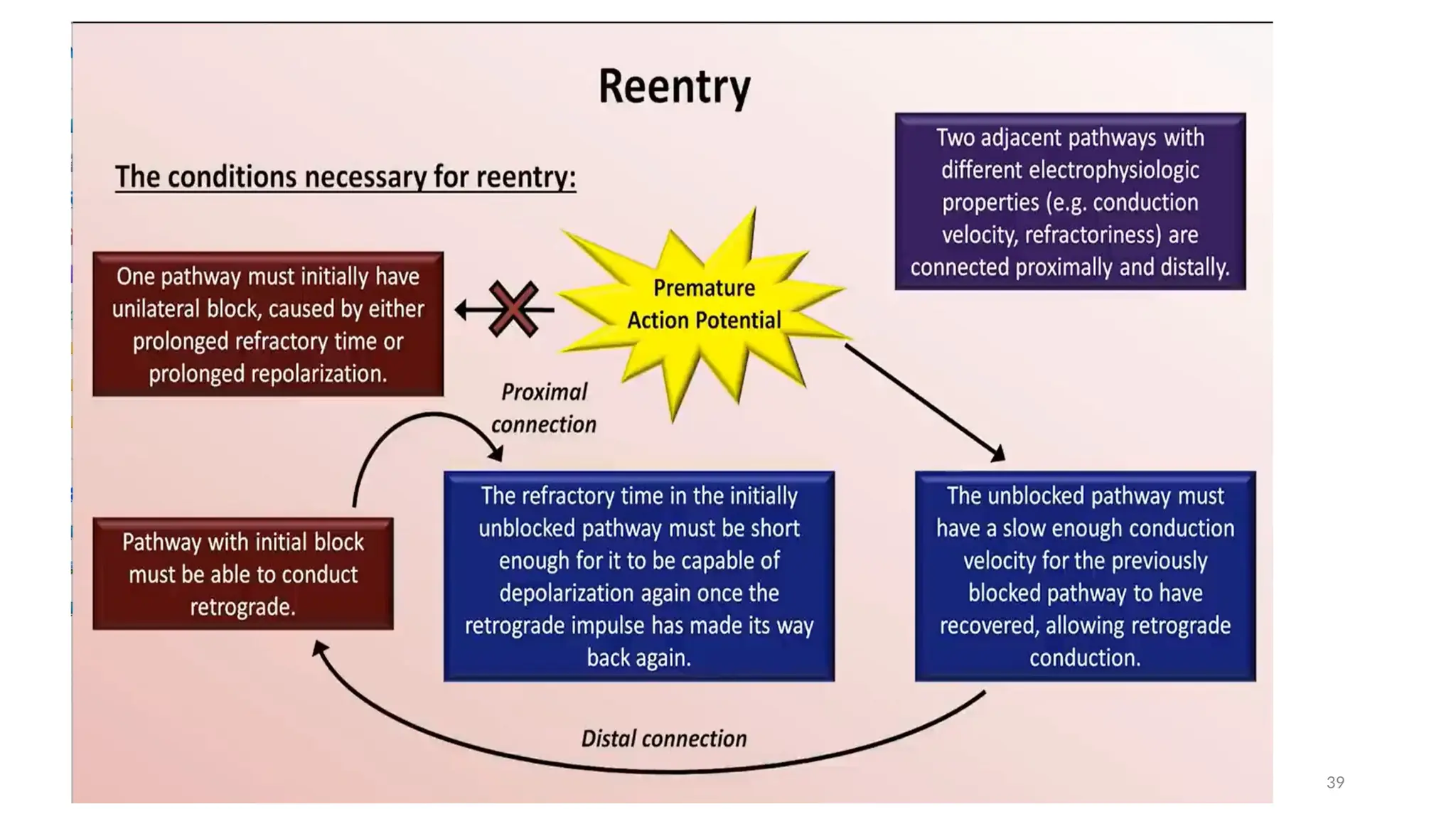
Re-entry
The mechanism ofre-entry occurs when a 'ring' of cardiac tissue surrounds an inexcitable core (e.g. in
a region of scarred myocardium).
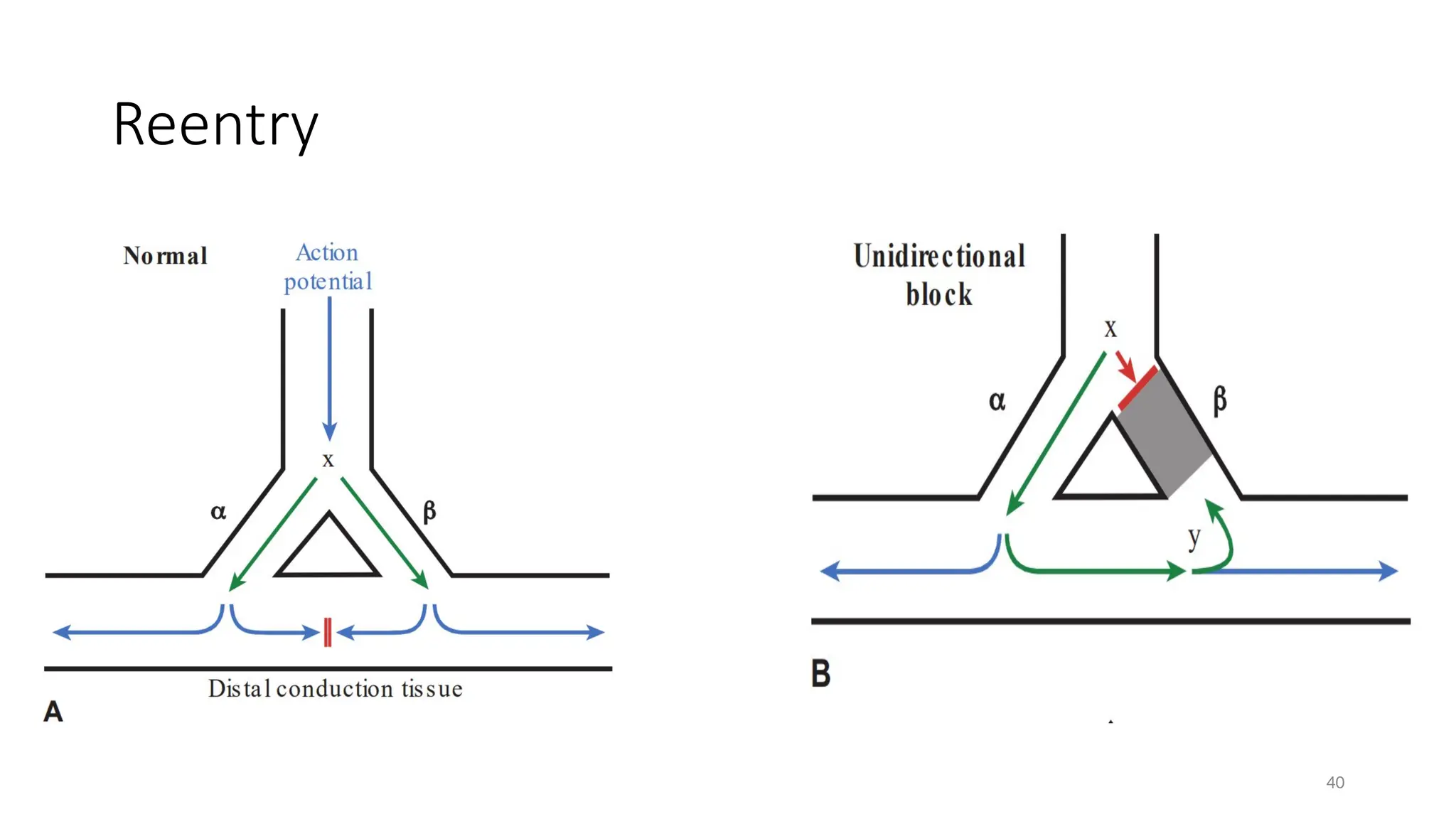
Tachycardia is initiated if an ectopic beat finds one limb refractory (α), resulting in the unidirectional
block and the other limb excitable.
Provided conduction through the excitable limb (β) is slow enough, the other limb (α) will have
recovered and will allow retrograde activation to complete the re-entry loop.
If the time to conduct around the ring is longer than the recovery times (refractory periods) of the
tissue within the ring, circus movement will be maintained, producing a run of tachycardia.
The majority of regular paroxysmal tachycardias are produced by this mechanism
Reentry
• Reentry canbe subdivided into 2
categories based on whether the reentrant
circuit is large enough to be mapped via
catheter
• Macroreentry –Circuit is large enough to
be mapped (e.g Atrial flutter, AVRT)
• Microreentry- Circuit is too small to be
mapped e.g atrial fibrillation, intraatrial
reentrant tachycardia
42













































![Reading Techniques [Autosaved].pptxReading Techniques [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/readingtechniquesautosaved-251211193055-b8821f9d-thumbnail.jpg?width=640&height=640&fit=bounds)

