Anaesthesia for Laparoscopic surgeries and procedures
Anaesthesia for laparoscopy procedures and possible complications for such procedures. This also covers the Anaesthetic perioperative considerations, post operative care and possible perioperative complications.
Introduction
Most Endoscopicprocedures are diagnostic,
few therapeutic, and are carried out by using
the natural orifices, with the use of fibreoptic
with camera.
Cut across all subspecialties with GIT
probably in the lead.
Are mostly done under moderate – Deep
sedation, GA
Laparoscopy – Most challenging
3.
OBJECTIVES
To identifythe anaesthetic challenges
associated with laparoscopic surgical
technique.
To be equipped with evidence based
knowledge to manage patients peri-
operatively for laparoscopic surgeries
and ensure their safety.
4.
OUTLINE
1. History
2. Whatis laparoscopy and its applications
3. Advantages. and disadvantages.
4. Contraindications
5. Physiological changes
6. Choice of anaesthesia
7. Complications
8. Special considerations in Pregnant woman/Children
9. Conclusion.
5.
HISTORY
• George Kellingused cystoscope to
observe abd organs of dogs—
CYSTOSCOPY
• 1910 – Swedish physician Hans Christian
Jacobaeus
used this procedure in man and coined the
term – LAPAROSCOPY
6.
HX
In 1924,Richard Zollikofer of
Switzerland promoted the use of CO2
as the insufflating gas.
Later Janos Veress of Hungary
developed a spring loaded insufflation
needle.
It was Raoul Palmer in Paris in 1944-
monitoring intra-abdominal pressure.
7.
History
It wasanother 20 years, however,
before Kurt Semm in Kiel, Germany,
developed an automatic insufflation
device.
1986 that a computer chip TV camera
was developed and attached to the
scope.
1987 – Mourett in France succesfully removed
a diseased gall bladder.
8.
Trend in Nigeria.
Dr Ojukwu in Lagos early 2000
In Ibadan – 2009, resuscitated
UCH Data- so far
>45 cholecystectomies,2 under CSE
30 Appendectomies, 10 under CSE.
18 OBG.
2 involving children.
Many diagnostic procedures.
Data @ at 2015.
10.
Definition
• It isa minimally access procedure allowing
endoscopic access to peritoneal cavity after
insufflation of gas to create space between the
anterior abd. Wall & viscera for safe manipulation of
instruments & organs.
TYPES
1 Intraperitoneal
2 Extraperitoneal
3 Abd wall retraction (gasless laproscopy)
4 Hand assisted (Hassans tech.)
KEYHOLE SURG
PINHOLE SURG
11.
ADVANTAGES
1 Minimal pain& illeus
2 Improved cosmesis
3 Shorter hospital stay , faster recovery & rapid
return to work, cost?
4 Non muscle splinting incision & less blood loss
5 Post op respiratory muscle function returns to
normal more quickly
6. Wound complications i.e. infection & dehiscence
are less, less retraction.
7 Lap surgery can be done as day care surgery
12.
Disdvantages……
More expensive
More operating time
Difficult in complicated cases
Potential for major complications
in inexperienced hand
Causes of anaesthetic
challenges
Pneumoperitoneum
Mechanicaleffects relating to increased
intra-peritoneal pressure.
Chemical effect of CO2 used for
insufflation.
Effect of Positioning.
Unsuspected visceral injuries
Difficulty in estimating blood loss
Darkness in the OR
INSUFFLATING GAS OFCHOICE FOR
LAPROSCOPY
Ideal insufflating gas of choice
Colorless, non toxic, nonflammable, easily available,
inexpensive, inert, readily soluble in blood and easily
ventilated out of lungs
Why CO2 is the gas of choice for laparoscopy ?
1 Nonflammable & does not support combustion
2 Highly soluble in blood because of rapid buffering
in blood so risk of embolisation is small
3 Rapidly diffusible through membranes so easily removed by
lungs
4 CO2 levels in blood & expired air can be easily measured & its
elimination is augmented by increasing ventilation
5 CO2 is readily available & is inexpensive
18.
Pneumo Peritonium…
Insufflator Gasused
N2O /CO2 /Argon /He/ Air
Preferred gas : CO2
Working pressure : 12 to 14 mm Hg
Slow inflation of 1 liter / minute
(Air & O2 –risk of embolism high.
N2O –bowel distension,risk of explosion,PONV.
He & Argon not available here- embolism)
19.
Hemodynamic Effects
Dependson the interaction of:
patient’s pre-existing cardiopulmonary
status
anesthetic technique
intra-abdominal pressure
carbon dioxide absorption
patient position
duration of surgery.
20.
CVS
Early Hypercarbia stimulatessymp-
adrenal axis with Adr & NAdr in bld
Tachycardia, arrythmia
BP - Elevated BP,CO,CVP
when IAP > 20 – 30mmHg decrease
in BP,CO,CVP , same in late hypercarbia
CNS
2-4% inCBF with every 1mmHg
PCO2 (25-100mmHg)
Raised ICP
Increase in cranio-facial congestion,
worse with Trendeleburg position
23.
RENAL
Oliguria commonduring lap. surgery
Hypovol, IPPV, PEEP
Incr IAP eg > 15mmHg renal BF
decreased 60% & 50% u/o
NO SUCH CHANGES- in Gasless
lap(abd wall lift)
24.
METABOLIC
Temperature variation
continous flowof dry gases over peritoneal surface under P at
high flow rates + lavage with cold fluid
Neuro-hormonal stress response
- equal = open surgery (ACTH, cortisol, insulin, glucagon, bld
glucose)
hypothermia
(0.3˚C/50L co2)
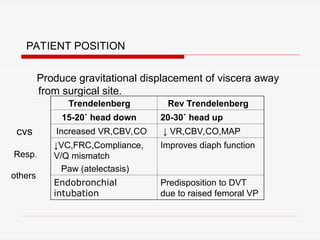
PATIENT POSITION
Produce gravitationaldisplacement of viscera away
from surgical site.
Trendelenberg Rev Trendelenberg
15-20˚ head down 20-30˚ head up
Increased VR,CBV,CO ↓ VR,CBV,CO,MAP
↓VC,FRC,Compliance,
V/Q mismatch
Paw (atelectasis)
Improves diaph function
Endobronchial
intubation
Predisposition to DVT
due to raised femoral VP
cvs
Resp.
others
27.
ANAESTHETIS TECHNIQUES
LapSx amenable to all but
individualize your pt
LA wt mild sedation(aim Ramsay 2-
3)eg in minor lap tubal sterilisation.
GA- may be tech-of-choice with
cuffed ETT
-RA – Spinal,Epidural or CSE
28.
GA plus ETT
Pros- less anxiety,amnesia possible
adeq muscle relaxation-very important
Flexibility(sx may be unusually long
Less risk of regurgitation/aspiration
Unanticipated resp compromise easily
managed
REGIONAL ANAESTHESIA
Betterpost-op analgesia
Less PONV (Vs GA)- less emetogenic
agents use
Less blood loss
Faster recovery etc
Less thromboembolic phenomena.
31.
Cont---
CONS- Highlevel of block required
Sympathetic blockade – may worsen wt
hypercarbia of lap sx
NG Tube discomfort in consciuos pt
May delay discharge for day case.
32.
ANAESTHESIA
Preop.
Done in usualmanner with special attention to
cardiac & pulmonary system
Investigations
1. Complete hemogram
2. RBS
3. E/U, Creatinine
4. Coagulation profile
5. CXR, ECG
Special investigations
1. ECHO
2. PFT
33.
PREMEDICATION
1. NPO
3. Antibioticsas per surgical team
4. Awareness about post op shoulder tip pain
5. Written informed consent for laparotomy
6. Anxiolytics/antiemetics/H2 receptor antagonist/analgesic
7. Antisialagogue (glyco-P) and vagolytic may be
administered at induction of anaes.
8. DVT prophylaxis (rTn, pelvic Sx, long duration,
malignancy, obesity) TED stocking.
CONDUCTION OF LAP.SURGERY UNDER GA
1. Preloading- 5-10 ml/kg to prevent hemodynamic
changes during pneumoperitoneum
2. Induction- propofol, thiopentone Na, TIVA
(propofol+fentanyl)
3. Msl relaxation – Scoline (RSI) for antireflux surg.
NDMR
4. Maintainence – O2 +? N2O + iso/sevo, halo
36.
Cont…..
4. Folleys catheterand NG tube insertion to avoid
bladder/bowel injury (↓PONV, improve surgical view)
5. Ventilatory settings- To maintain normocarbia
(ETco2 34-38 mm Hg)- RR rather than TV as the
lung compliance is low.
6. Positioning – gradually, tilt < 15-20˚, check ETT
position, padding at pressure points.
7. Gas insufflation – slow (1-1.5 →1-2.5 L/min)
IAP<15 mm Hg (10-12)
check ETT position
Nitrous ?
potential undesirableeffects during
lap sx
may cause bowel distension
will worsen pneumothorax if dev.
May be a potential ignition hazards
worsen PONV highly emetogenic
39.
COMPLICATIONS
Intraop. eventsfrom:-
1. Pneumoperitoneum viz cvs, resp.
2. Gas Extravasation, pneumothorax,
Mediasternum, s/c emphysema
3. Positioning, nerve injury,
endobronchal intubation from
Tradelenburg/Abd. distention
40.
GASLESS LAPAROSCOPY
Peritonealcavity is expanded using
abdominal wall lifter.
This avoids haemodynamic &
respiratory repercussions of increased
IAP
It increases technical difficulty
Cont…..
Treatment
1. Release source(stop co2 + release pneumoperit)
2. position – steep head low
3. stop N2O
4. Hyperventilation
5. CVP/PA catheter to aspirate CO2
6. Cardiac massage may break embolus- rapid
absorption
44.
Laparoscopy in children
1Physiological changes = adults
2 Paco2/ ETco2 increase but ETco2 overestimates
Paco2
3 Co2 abs more rapid and intense due to larger
peritoneal SA / body wt.
4 More chances of trauma to liver during trocar
insertion
5 More chances of bradycardia , maintain IAP to as low
as possible
45.
Laparoscopy in pregnancy
Indications-appendicectomy
cholecystectomy
Risk – preterm labour, miscarriage, fetal acidosis
Timing – II trimester (< 23 wk)
Lap technique – HASSANS tech
Special considerations
1.prophylactic- antithrombolytic measures + tocolytics
2.operating time to be minimised
3.IAP as low as possible
4.Continous fetal monitoring .
CONCLUSION
An improvedknowledge of intraoperative
repercussions of laparoscopy permits safe
management of patients who may subsequently
benefit from the multiple postop advantages
offered by this technique
48.
REFERENCES
Joshi, G.Anesthesia for
laparoscopic surgery. Canadian
Journal of Anesthesia 2002; 49:
45-49
Kaba, A. Joris, J. Anesthesia for
laparoscopic surgery. Current
Anesthesia and Critical Care 2001;
12(3): 159-165.
49.
Mullet, C.,Viale J., Sagnard, P., et al.
Pulmonary CO2 elimination during
surgical procedures using intra- or
extraperitoneal CO2 insufflation.
Anesth-Analg 1993; 76: 622-6.
Taylor, E., Feinstein, R., White, P., &
Soper, N. Anesthesia for laparoscopic
cholecystectomy: is nitrous oxide
contraindicated? Anesthesiology
1992; 76: 541-3
Editor's Notes
#1 DR ROTIMI OLONISAKIN, CONSULTANT ANAESTHETIST UCH-IBADAN. 20/07/2021
#7 Jayashree S, Lakshmi J, Kumra V. Endoscopic Surgery-Anaesthetic Challenges –a historical review. Indian J. Anaesth. 2006; 50 : 178-182.
#8 Afuwape O, Acute O, Adebanjo A. Preliminary experience with laparoscopic cholecystectomy in a Nigerian Teaching Hospital. West Afr J Med. 2012;31:120-3
#11 1. O’Malley C, Cunningham AJ. Physiologic changes during laparoscopy. Anesthesiol Clin North America. 2001;19:1–19.



















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






