Download to read offline













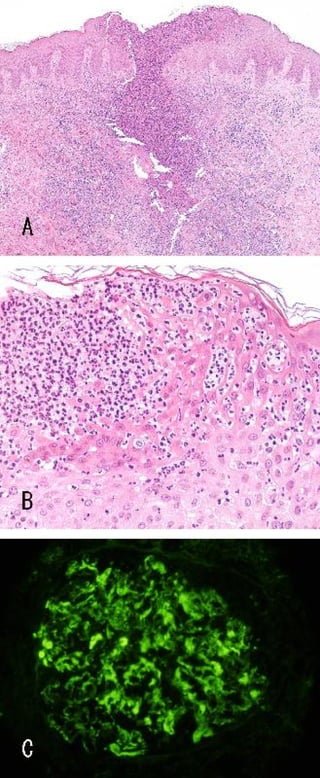



This case report describes a 31-year-old man with amicrobial pustulosis associated with autoimmune diseases (APAD). He suffered from IgA nephropathy and Sjögren's syndrome. His skin symptoms included multiple pustules over his entire body that improved with corticosteroids but relapsed after tapering. Skin biopsies showed neutrophilic infiltration without microorganisms. He achieved complete remission of his skin symptoms after corticosteroid pulse therapy and tonsillectomy. This clinical presentation adds to the limited reports of APAD associated with defined systemic autoimmune diseases.
































































