. Inflammatory diseases of the skin, subcutaneous tissue, loose connective tissue (cellular spaces). (lecture 10).pdf
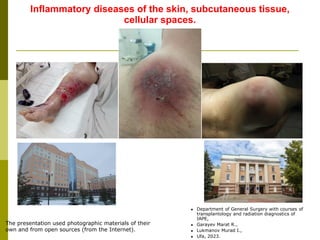
1. Inflammatory diseases of the skin, subcutaneous tissue,
cellular spaces.
The presentation used photographic materials of their
own and from open sources (from the Internet).
Department of General Surgery with courses of
transplantology and radiation diagnostics of
IAPE,
Garayev Marat R.,
Lukmanov Murad I.,
Ufa, 2023.
2. 1.1. Uncomplicated infections
1st level—skin
1. Furuncle and furunculosis
2. Erysipelas
2nd level—subcutaneous tissue
1. Carbuncle
2. Hydradenitis
3. Uncomplicated abscesses
4. Cellulite
5. Phlegmon
1.2. Complicated infections
2nd level—subcutaneous tissue
Necrotic cellulitis
3rd level - superficial fascia
Necrotizing fasciitis
Level 4—muscles and deep fascial structures
1. Pyomyositis
2. Myonecrosis
Classification of primary surgical infections of the skin and
soft tissues:
3. - Folliculitis;
- Furuncle (boil);
- Furunculosis);
- Carbuncle;
- Hydradenitis;
- Erysipelas;
- Abscess;
- Phlegmon.
The most common inflammatory diseases of the skin and
subcutaneous tissue include:
4. - acute purulent inflammation of the hair follicle.
Clinical picture: The process begins with the development of hyperemia and infiltration in the area of the
hair follicle. Then (within a few days) a pustule with purulent contents is formed from which the hair comes
out. When the pustule is opened and the abscess is emptied, an ulcer remains, which becomes covered
with a crust. Subsequently, the skin defect heals by secondary intention. Sometimes there is a noticeable
scar, sometimes hyperpigmentation is possible. Most often, folliculitis is multiple.
Most often, patients with pyoderma, which includes folliculitis, are observed and treated by a dermatologist,
but may also be in the surgeon's field of vision.
Complications: transition to more severe forms of purulent skin processes such as boils, carbuncles,
abscesses, etc.
Diagnostics: sowing of the separated pustules with the definition of the pathogen and its sensitivity to
antimicrobial / antiviral drugs; dermatoscopy.
Treatment: in the initial stage and mild cases, treatment includes lubricating the affected skin with dyes
(fukartsin, "brilliant green"), treating the skin around with boric or salicylic alcohol, and prescribing
UVI. In more severe and recurrent cases, antimicrobials are used systemically, and background
diseases that aggravate the course of folliculitis (diabetes mellitus, immunodeficiency states) are
identified and treated.
Folliculitis
5. - acute purulent inflammation of the hair follicle, sebaceous gland and involvement in the process of
surrounding fatty tissue.
Clinical picture: The process proceeds in 2 stages: infiltration (reversible stage) and abscess formation
(irreversible stage). The disease begins with the formation of an inflammatory infiltrate in the area of the
hair follicle. In the stage of infiltration, the reverse development of the process is possible. With the
progression of the process, necrosis of the skin and tissue occurs with the formation of a purulent-necrotic
rod in the center of the infiltrate along the hair and accumulation of pus (abscess formation) in the
subcutaneous tissue.
Complications and outcomes:
1) In the stage of abscess formation, the following are possible: - breakthrough and emptying of the
abscess into the external environment, followed by cleansing and healing of the resulting wound;
- distribution of the process to the surrounding tissue with the development of phlegmon, sepsis, etc.
2) When localized on the face (in the nasolabial triangle, buccal areas), it is possible
spread of infection through the veins: facial vein angular vein superior ophthalmic vein cavernous
sinus of the dura mater development of meningitis/encephalitis.
3) With lymphogenous spread of the infection, the development of lymphangitis / regional lymphadenitis is
possible
Furuncle (continued)
6. Treatment: in the stage of infiltration, the treatment is conservative, including lubrication with
alcohol, iodine tincture, it is possible to use physiotherapy (UHF, UVI), half-alcohol compresses and
dressings with ichthyol ointment.
In the stage of abscessing - surgical treatment: opening the abscess under local infiltration anesthesia
with the removal of a purulent-necrotic rod, evacuation of the abscess and drainage with a rubber
strip for 1-3 days. It is strictly forbidden to extrude a boil, especially on the face, which can lead to the
spread of the purulent process to neighboring tissues or the generalization of the process.
Furuncle (continued)
7. - inflammation of several hair follicles simultaneously or sequentially.
Clinical picture: There are many boils simultaneously or sequentially. Often, furunculosis also indicates
the presence of serious problems with immunity, it can develop against the background of diabetes
mellitus, beriberi, hormonal imbalance, and chronic sepsis.
Treatment: for effective treatment of furunculosis, it is necessary to examine the patient in order to
identify the cause of the disease. In the treatment, in addition to surgical treatment at the stage of
abscess formation, antibiotics, autohemotherapy, immunostimulants, and ultraviolet blood are used.
As an additional treatment, biologically active additives (brewer's yeast) can be used.
Furunculosis
8. - acute purulent-necrotic inflammation of several hair follicles, merging into a single infiltrate,
accompanied by necrosis of the skin and fiber and their purulent impregnation.
Clinical picture: proceeds acutely with high body temperature, expressed by general intoxication of the
body. An extensive (up to 10 cm or more in diameter) focus is formed locally with all signs of inflammation,
later tissue necrosis develops in the central part.
Complications: in the absence of surgical treatment, there is a high risk of spreading the process to the
surrounding tissue with the development of phlegmon, sepsis, etc.
Carbuncle
9. Treatment: strictly surgical, under anesthesia, an abscess is opened with a cruciform incision with excision
of necrotic tissues - necrectomy. Subsequently, dressings are carried out with antiseptic solutions,
water-soluble ointments with an antimicrobial effect. To speed up the cleansing, a surgical laser,
ultrasound, hydrosurgery are used. With the formation of large defects in the skin, after the relief of
inflammation and the transition of the wound process to the second phase, a skin transplant is
performed.
Carbuncle (continued)
The next day
(after
surgery)
In 3
weeks
10. - acute purulent inflammation of the apocrine sweat glands. Most often localized in the armpits.
Clinical picture: the disease begins with the formation of a painful seal or several seals (often in multiple
forms) in the axillary (less often inguinal or nipple, etc.) area (infiltration stage), then local hyperemia, skin
hyperthermia develop and an abscess forms, which sometimes breaks out with the formation of a purulent
fistula. The occurrence of hydradenitis is facilitated by the use of antiperspirants (they disrupt the
functioning of the sweat glands) and shaving of the skin (microtraumas that serve as entry gates for
infection).
Complications: the formation of purulent fistulas; chronization of the process with frequent exacerbations;
in the absence of surgical treatment, there is a possibility of the process spreading to the surrounding tissue
with the development of phlegmon, sepsis, etc.;
Diagnostics: additional ultrasound - in case of doubt in the diagnosis.
Hydradenitis
12. Treatment: Before abscessing, conservative treatment is possible: warming compresses, UHF, stopping the
use of antiperspirants and shaving the inflamed area, strengthening immunity, normalizing
metabolism.
With abscess formation - surgical treatment under local infiltration anesthesia:
1) opening, sanitation and drainage of the purulent cavity; at the same time, a part of the capsule of the
inflamed sweat gland may remain, which often causes relapses of hydradenitis in the future;
2) excision of an inflamed sweat gland with a capsule and surrounding tissue, which eliminates the
possibility of a recurrence of the disease. This option is often performed not in the purulent phase of
the disease.
Hydradenitis (continued)
13. - acute inflammation of the skin itself, and in rare cases - of the mucous membranes.
Etiology: Refers to infectious diseases, infection occurs when the pathogen penetrates into the thickness of the
skin or mucous membrane through the "entrance gate" (wounds, cracks, scratches, ulcers, calluses, diaper
rash, etc.). Streptococci - in most cases, less often - mixed infection.
Classification: (V.L. Cherkasov, 1996):
According to the nature of local manifestations:
- erythematous;
- erythematous-bullous;
- erythematous-hemorrhagic;
- bullous-hemorrhagic.
By severity:
- light (I);
- medium (II);
- heavy (III).
By clinical course:
- primary;
- repeated (with a recurrence of the disease after two years; a different localization of the
process);
- recurrent (if there are at least three recurrences of erysipelas per year, it is advisable to define
"frequently recurrent erysipelas").
According to the prevalence of local manifestations:
- localized;
- widespread (migratory);
- metastatic with the occurrence of foci of inflammation distant from each other.
Complications:
Early:
- local (abscess, phlegmon, necrosis, phlebitis, periadenitis and others);
- general (sepsis, infectious-toxic shock, pulmonary embolism and others).
Later: persistent lymphostasis (lymphatic edema, lymphedema); secondary elephantiasis
Erysipelas
14. Clinical picture: The onset is acute: symptoms of general intoxication predominate (weakness, chills,
myalgia ...) with high (up to 40-41 degrees) body temperature. Later, local symptoms join in the zone of
future development of inflammation (burning sensation, paresthesia). After 1-2 days, local changes
develop, depending on the nature of which the form of the disease is classified. Most often (about 80%),
the process develops on the lower extremities, less often on the face (up to 15-20%) and upper extremities
(4-7%); in other areas it is very rare.
Erythematous form: a small red spot appears, which in a few hours turns into a characteristic erythema
erysipelas (a clearly demarcated area of hyperemic skin with uneven borders in the form of teeth, tongues).
The skin in the area of erythema is infiltrated, tense, hot to the touch, moderately painful on palpation
(more along the periphery). Sometimes you can find a "peripheral roller" in the form of infiltrated and
elevated edges of erythema. Skin edema develops, extending beyond the erythema.
Diagnostics: leukocytosis and an increase in ESR (Erythrocyte Sedimentation Rate) in the blood test.
Rare: Antistreptolysin O (ASLO), PCR.
Treatment: in the erythematous form, conservative: dressings with antiseptics, ultraviolet radiation,
antibiotics (primarily penicillin), desensitizing therapy.
Erysipelas (continued)
15. Erythematous bullous form: develops in terms from several hours to 2-5 days against the
background of erythema. Against the background of erythema, bullae (bubbles) appear, which
is associated with increased exudation in the focus of inflammation and detachment of the
epidermis from the dermis, accumulated fluid. If the surfaces of the blisters are damaged or
spontaneously rupture, exudate flows out of them, often in large quantities, erosion occurs in
place of the blisters. While maintaining the integrity of the blisters, they gradually shrink with
the formation of yellow or brown crusts.
Diagnostics: leukocytosis and an increase in ESR in the blood test. Sowing discharge from opened blisters
with the identification of the pathogen and the determination of sensitivity to antimicrobial drugs.
Treatment: opening of blisters under aseptic conditions, dressings with antiseptics, ultraviolet radiation,
antibiotics (primarily penicillin), desensitizing therapy.
Erysipelas (continued)
16. Erythematous-hemorrhagic form: develops against the background of erythematous
erysipelas within 1-3 days from the onset of the disease, less often later. Hemorrhages of
various sizes appear - from small petechiae to extensive drain hemorrhages, sometimes
throughout the erythema.
Diagnostics: leukocytosis and an increase in ESR in the blood test. Sowing discharge from opened blisters
with the identification of the pathogen and the determination of sensitivity to antimicrobial drugs.
Rare: ASLO, PCR. Ultrasound of blood vessels to exclude patency disorders, vascular thrombosis.
Treatment: dressings with antiseptics, ultraviolet radiation, antibiotics (primarily penicillin), desensitizing
therapy, correction of coagulation system parameters.
Erysipelas (continued)
17. Bullous-hemorrhagic form (the most severe and most severe form of complications): develops
from an erythematous-bullous or erythematous-hemorrhagic form as a result of damage to the blood
vessels of the dermis. The bullae are filled with hemorrhagic and/or fibrohemorrhagic exudate, extensive
hemorrhages occur in the skin. Blisters of dark color with inclusions of fibrin are formed. In patients with
the development of repair in the area of the bulls, brown crusts form. In other cases, the bullae rupture and
their contents are torn away, exposing the eroded bottom. In most patients, then gradual epithelialization of
skin defects occurs. With significant hemorrhages in the bottom of the bladder and the thickness of the
skin, necrosis may develop, sometimes with the addition of a secondary infection, the development of
phlegmon, sepsis.
Diagnostics: leukocytosis and an increase in ESR in the blood test. Sowing discharge from opened blisters
with the identification of the pathogen and the determination of sensitivity to antimicrobial drugs.
Treatment: dressings with antiseptics, ultraviolet irradiation, antibiotics (combination of several drugs),
detoxification therapy, desensitizing therapy, correction of coagulation system parameters. With the
development of phlegmon - a wide opening of the subcutaneous tissue, with tissue necrosis -
necrotomy (dissection of tissues) and necrectomy (excision of necrosis); after relief of inflammation
and the transition of the wound process to the second phase - skin grafting to close the defect.
Erysipelas (continued)
19. - limited accumulation of pus in soft tissues, cavities or organs; has a cavity filled with pus, a capsule forms
over time.
Classifications:
By localization:
- Surface.
- Deep:
a) abscesses of internal organs: abscesses of the brain, lungs, liver, etc.
b) cavity abscesses - abscesses of the abdominal cavity:
subphrenic, subhepatic, interintestinal, Douglas space.
By clinical course:
Acute - a more pronounced clinical picture that develops in a short time;
Chronic - the clinical picture is less bright, the process is long (more often in the lungs).
Complications:
Breakthrough of the abscess into adjacent cavities with the development of peritonitis, pyothorax, infectious
toxic shock, sepsis, renal amyloidosis
Abscess
20. Clinical picture: an abscess is most often a complication of either an inflammatory process
(lymphadenitis, pneumonia, etc.) or a disease (hematoma suppuration), manifestations may
be metastatic (abscesses with septicopyemia) or post-injection (if hypertonic solutions, certain
drugs (magnesium) enter the tissues ) sulfate, calcium chloride)) nature, less often - is a
complication of surgical interventions (postoperative abscess). It is manifested by edema,
hyperemia and soreness in the focus, dysfunction of this part of the body, and an increase in
local temperature. In the center of the inflammatory infiltrate, fluctuation (softening) occurs
during abscess formation. With large abscesses, chills, hectic fever, and severe intoxication are
characteristic.
Abscess (continued)
21. Diagnostics: Leukocytosis and an increase in ESR in the blood test. Ultrasound of soft tissues, diagnostic
puncture - in case of doubt in the diagnosis; Ultrasound, CT, MRI for deep abscesses; laparoscopy - in the
diagnosis of the inflammatory process in the abdominal cavity.
Abscess (continued)
22. Treatment: abscess surgery only:
1. Puncture method - puncture and evacuation of pus (including under the control of ultrasound /
CT);
2. Puncture-flow method - puncture and drainage (including under the control of ultrasound /
CT);
3. Open method - opening, sanitation and drainage of the abscess;
4. A radical method is the removal of part or all of an organ with an abscess (for example:
lobectomy - removal of a lung lobe during its abscess).
Abscess (continued)
24. - acute diffuse inflammation of the cellular tissue, which does not tend to delimit.
- Classifications:
By localization:
- Subcutaneous;
- Subfascial;
- Intermuscular;
- Deep cellular spaces: mediastinum - mediastinitis,
deep phlegmon of the neck
phlegmon of the retroperitoneal space,
pararectal space - paraproctitis,
perirenal space - paranephritis, etc.
By the nature of the exudate:
- Serous;
- Purulent;
- Putrid.
Phlegmon
25. Clinical picture: phlegmon is most often a complication of any inflammatory process. It is manifested by
edema, hyperemia and soreness in the focus, dysfunction of this part of the body, an increase in local and
general temperature.
Diagnostics: Leukocytosis and an increase in ESR in the blood test. Ultrasound of soft tissues, diagnostic
puncture - in case of doubt in the diagnosis; Ultrasound, CT, MRI with phlegmon of deep cellular spaces.
Treatment: Before suppuration (tissue destruction), conservative treatment is possible: half-alcohol
compresses, UHF, strengthening immunity, normalizing metabolism, prescribing antimicrobial drugs.
In case of suppuration, surgical treatment under regional or general anesthesia: wide
(throughout the inflammation zone) opening, sanitation of the purulent focus, excision of non-viable
tissues (necrectomy), open management (without suturing) or drainage through additional incisions
(counter-openings) of the resulting wound until suppression microflora and relief of inflammation.
Phlegmon (continued)
26. phlegmon of the cellular spaces of the neck
mediastinitis;
paraproctitis;
phlegmon of the retroperitoneal space;
paranephritis.
The most significant inflammatory processes of cellular
spaces include:
27. - inflammation of the tissue located under and between the fascia of the neck.
Infection in the deep cellular spaces of the neck most often enters from the oral cavity, nasopharynx,
trachea, esophagus, less often by the hematogenous or lymphogenous route. Progression of the
inflammatory process in the teeth (caries), complicated by osteomyelitis of the jaw and perimaxillary
phlegmon, phlegmon of the floor of the mouth, can lead to deep phlegmon of the neck. Also, a deep
phlegmon of the neck can be complicated by a pharyngeal abscess, suppuration of neck cysts, injuries of
the cervical esophagus and trachea, purulent inflammation of the lymph nodes of the neck, etc.
Clinical picture: in the debut of the disease, patients note arching pains in the neck and local
swelling; there is no local hyperemia at the beginning, which makes it difficult to diagnose the process. The
progression of the process leads to an increase in local temperature, a dense edema develops, which leads
to compression of the trachea and esophagus. Severe intoxication develops: high fever, tachycardia,
leukocytosis. Often, inflammation is putrefactive or anaerobic in nature, which, if diagnosed late, can lead
to mediastinitis, sepsis.
Features of deep phlegmon of the neck:
- The possibility of spreading through numerous interfascial fissures and along the neurovascular bundles of
the neck, with the development of purulent mediastinitis;
- Erased local signs of inflammation in the initial stages, which leads to late diagnosis of neck phlegmon.
Deep phlegmon of the neck
28. Diagnostics: Leukocytosis and increased ESR - in the blood test. Ultrasound, CT (main method) of the soft
tissues of the neck; FEGDS (with suspected damage to the esophagus, pharynx), FBS (with suspected
damage to the trachea).
Treatment: Before suppuration (tissue destruction), conservative treatment is possible: half-alcohol
compresses, UHF, prescription of antimicrobial drugs, continuous monitoring of the dynamics of the process.
In case of suppuration, surgical treatment under general anesthesia: opening, debridement of the
purulent focus, excision of non-viable tissues (necrectomy), open management (without suturing) or
drainage through additional incisions (counter-openings) of the resulting wound until the microflora is
suppressed and inflammation is relieved.
Deep phlegmon of the neck (continued)
29. - purulent inflammation of the tissue of the mediastinum.
The causes of mediastinitis can be: phlegmon of the neck, damage to the trachea and bronchi,
complications during operations on the mediastinum, perforation of the esophagus (foreign body, with
diagnostic and therapeutic endoscopy, with Boerhaave's syndrome - "banquet syndrome").
Clinical picture: Downstream, a lightning-fast form is isolated, when patients die in the first two
days. More often there is an acute form with a less violent clinical picture. The process can also have a
subacute course, especially with massive antibiotic therapy. At the beginning of the disease, patients report
pain behind the sternum or in the back. The disease is extremely difficult, developing: hyperthermia up to
39-42 degrees, chills, tachycardia up to 120-140 beats per minute, shortness of breath, chest pain. The
pain is aggravated by swallowing, dysphagia is observed. Crepitation due to subcutaneous emphysema is
possible.
Diagnostics: Leukocytosis and increased ESR - in the blood test. X-ray of the chest in 2 projections,
where the expansion of the shadow of the mediastinum, free air or fluid level in the mediastinum can be
detected. For early diagnosis/clarification, confirmation of the diagnosis, CT (the main method) of chest is
used; fluoroscopy of the esophagus (it is possible to detect leakage of contrast outside the esophagus) and
FEGDS (if damage to the esophagus, pharynx is suspected), FBS (if damage to the trachea is suspected).
With the development of concomitant pleurisy, fluid is detected in the pleural cavity.
Purulent mediastinitis
31. Treatment: emergency surgery under anesthesia immediately after diagnosis. The operation consists in
mediastinotomy - opening the mediastinum from the cervical access, transthoracic transpleural access
or laparotomy access (depending on the location of the inflammation zone in the mediastinum), or
use their combination for active washing and sanitation of the mediastinum.
In case of damage to the esophagus, various tactics of patient management are possible:
- drainage of the rupture zone and gastrostomy
- extirpation of the esophagus with esophagostomy and gastrostomy
- extirpation of the esophagus with its simultaneous plastic surgery.
NB! Mortality in mediastinitis is extremely high!
Purulent mediastinitis (continued)
34. - purulent inflammation of the pararectal (near-rectal) tissue.
More often, an infection (colibacillary, enterococcal, anaerobic) enters the pararectal tissue with injuries of
the perineum and rectum, with inflammation of the anal crypts, and also as a complication of a number of
diseases of the rectum.
Classification:
By localization:
- subcutaneous,
- submucosal,
- ischiorectal,
- retrorectal,
- pelvic-rectal paraproctitis.
By clinical course:
Acute and chronic paraproctitis.
Paraproctitis
35. Clinical picture: the disease begins with malaise, pain in the perineum, aggravated by
defecation. The temperature rises to 38-40ºС with chills. With superficial forms (subcutaneous
paraproctitis), hyperemia and swelling of the skin of the perineum and buttocks appear. With
deep paraproctitis, there may be no visible changes. A rectal digital examination reveals sharp
pain, infiltration and bulging of the walls of the rectum. With untimely treatment or diagnosis,
the abscess can open outward into the perineum or rectum, with the formation of fistulas.
From this time, the transition of acute paraproctitis to chronic begins, fistulas are incomplete
external or internal, and complete, one end of which has a message with the rectum, the
other end opens outward.
Paraproctitis (continued)
36. Diagnostics: Leukocytosis, shift of the leukoformula to the left and an increase in ESR - in the KLA. With
deep forms - ultrasound, rarely - CT, to examine the mucosa, they use - examination in the mirrors,
sigmoidoscopy.
Treatment: in acute paraproctitis, surgical treatment is indicated - opening the abscess under local or
regional (less often intravenous) anesthesia under the control of a finger inserted into the rectum (to
prevent injury to the mucosa). The incision is made taking into account the location of the external anal
sphincter. With putrefactive and anaerobic paraproctitis, a wide opening of the phlegmon with necrectomy is
shown. in acute paraproctitis, surgical treatment is indicated - opening the abscess under local or regional
(less often intravenous) anesthesia under the control of a finger inserted into the rectum (to prevent injury
to the mucosa). The incision is made taking into account the location of the external anal sphincter. With
putrefactive and anaerobic paraproctitis, a wide opening of the phlegmon with necrectomy is shown.
Paraproctitis (continued)
38. - purulent inflammation of the retroperitoneal tissue.
Most often it develops with retroperitoneal appendicitis, with complicated pancreatitis, with rupture or
perforation of an ulcer of the retroperitoneal part of the duodenum 12, with osteomyelitis of the pelvic
bones and vertebrae.
Clinical picture: the onset of retroperitoneal phlegmon is superimposed on the course of the
underlying disease and is rarely detected in the early stages. At the height of the disease, pain in the
lumbar regions, the forced position of the patient with legs brought to the stomach, an increase in body
temperature up to 39-40 g can develop. C, chills, worsening of the general condition of patients. Later (with
the addition of peritonitis), abdominal pain occurs, intestinal paresis develops.
Diagnostics: Leukocytosis and increased ESR - in the blood test. Ultrasound of the organs of the
abdominal cavity (OAC), retroperitoneal space (RS). For early diagnosis / clarification, confirmation of the
diagnosis, CT (the main method) of OAC, RS is used.
Phlegmon of the retroperitoneal space
39. Treatment: operational. They try to open the retroperitoneal phlegmon extraperitoneally, for which they perform
either a lumbotomy or a laparotomy, open the omental bag and the retroperitoneal space, followed by
isolation - marsupialization. Surgical intervention is combined with complex medical treatment.
Phlegmon of the retroperitoneal space (continued)
40. - purulent inflammation of the perirenal (perinephric) tissue.
Most often, paranephritis is secondary, it develops as a result of the spread of inflammation from the kidney
with carbuncle of the kidney, apostematous purulent pyelonephritis, kidney abscess, damage to the
perirenal tissue, urolithiasis with pyonephrosis, etc. Less commonly, paranephritis occurs with
lymphogenous and hematogenous infection.
Clinical picture: the disease is characterized by an increase in body temperature up to 38-40
degrees, chills, back pain. Pain can radiate distally - to the thigh, aggravated by walking, positive psoas
symptom - pain and impossibility of flexion in the hip joint of the straightened leg, so the leg takes a
forced position - half-bent at the knee and hip joints and brought to the stomach. Later, swelling and
soreness of the lumbar region develop.
Paranephritis
41. Paranephritis (continued)
Diagnostics:
1. Leukocytosis, shift of the leukoformula to the left and an increase in ESR - in the blood test.
Urinalysis shows proteinuria, leukocytes are detected.
2. X-ray methods. Plain urography reveals smoothness or disappearance of the contour of the psoas
muscle on the side of the lesion. Excretory urography reveals stenosis, occlusion of the urinary ducts (if they
were the cause of the disease).
3. Ultrasound examination - reveals signs of carbuncle of the kidney, pyelonephritis, infiltration of
perinephric tissue.
4. CT - reveals perirenal infiltration.
5. In the absence of ultrasound and CT, a diagnostic puncture of the perirenal tissue is possible
(currently rarely used).
43. Treatment: is a combination of surgical and medical methods. If paranephritis is detected, a
lumbotomy is performed, an autopsy, sanitation and drainage of perinephric tissue.
When identifying the primary cause, they try to eliminate it (remove the stone, stent the
ureter, etc.)
After the operation, broad-spectrum antibiotics, infusion therapy are prescribed, methods of
gravitational surgery are used, and kidney function is monitored.
Paranephritis (continued)
Incisions for access to the kidney