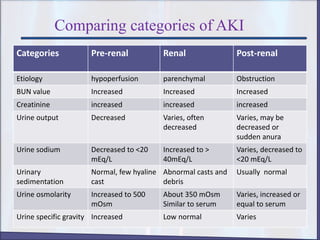
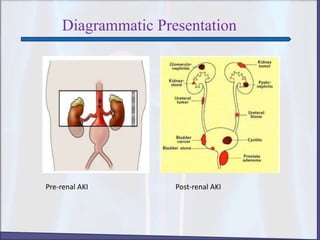
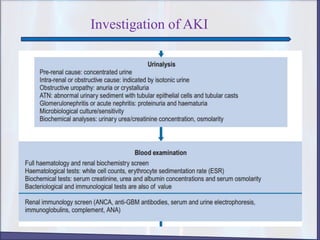
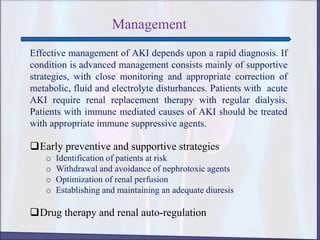
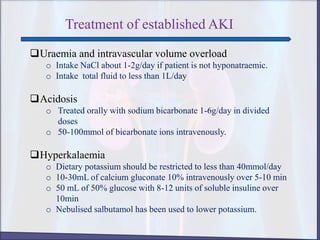
Acute Kidney Injury (AKI) is a rapid loss of kidney function classified into three categories: pre-renal, renal (intrinsic), and post-renal, each with distinct causes and clinical manifestations. Diagnosis involves history-taking, physical examination, and various imaging and lab tests, while management focuses on rapid diagnosis and supportive care, including monitoring and potential renal replacement therapy. Preventive strategies include risk identification, avoiding nephrotoxic agents, and optimizing renal perfusion, with specific treatments for associated complications such as hyperkalemia and acidosis.