ADOLESCENT
It is avital stage of growth and
development.
It is a period of transition from
childhood to adulthood.
Adolescent as individual in the 10-
19 years age group.
3.
Characterized by :-
Rapid physical
Psychological
Cognitive
Behavioural changes and
developments.
4.
Adolescence is classifiedinto three
groups:
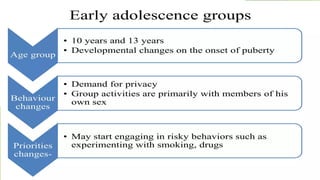
Early adolescence groups
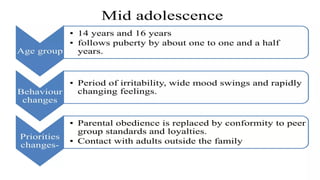
Mid adolescence groups.
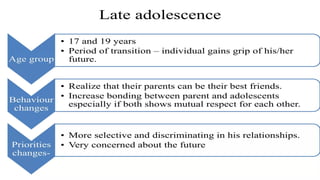
Late adolescence groups.
8.
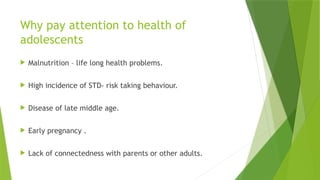
Why pay attentionto health of
adolescents
Malnutrition – life long health problems.
High incidence of STD- risk taking behaviour.
Disease of late middle age.
Early pregnancy .
Lack of connectedness with parents or other adults.
9.
Adolescent health programmes
1. RMNCH+A
2. Rashtriya Kishor Swasthya Karyakram[RKSK].
3. Kishori Shakti Yojana: to improve the health and nutritional
status of girls.
4. Nutrition Programme for Adolescent Girls[NPAG].
5. Balika Samridhi Yojana.
6. WIFS
7. National AIDS Control Programme.
8. Adolescent Friendly Health Clinics[AFHCs]
10.
RMNCH+A
KEY STRATEGIES
Family planning.
-Expansion of the basket of FP choices.
- Home delivery of contraceptives by ASHAs
- Fixed day static services at all facilities.
- Enhanced compensation scheme.
- Emphasis on post partum and post abortion FP services.
11.
Maternal Health
Earlyregistration of pregnancy .
ANC services, detection and follow-up on high risk cases
using MCTS (mother & child tracking system).
Encouraging institutional deliveries, improving access by
setting up delivery points & FRUs-over 20000 delivery
points &2200 FRUs
Maternal death review.
Comprehensive abortion care.
12.
JANANI SHISHU SURAKSHAKARYAKRAM
-JSSK launched in June 1st 2011 in mewat district in
Haryana.
-JSSK is an initiative under the overall umbrella of NRHM
that aims to reduce out of pocket expenses related to
maternal and new born care.
-Free services to all pregnant women & sick neonates
accessing public health institutions.
-Cashless services to pregnant women including normal
deliveries & c- sections.
13.
-Treatment ofsick women till 30 days.
-To be implemented in all govt. hospitals across states.
- Bound to benefit 1 crore pregnant mothers and
neonates.
IN emergency conditions it provides advanced life
support, vehicles with trained staff & equipments with
ambulance .
14.
JANANI SURAKSHA YOJANA
Launched on 12th
April 2005.
It is a govt of india sponsored scheme which is
being implemented with the objective of reducing
maternal & infant mortality by promoting
institutional delivery among pregnant women.
15.
BENEFITS
- If anexpected pregnant woman from rural area gets delivered at
Public Health Facility will get a cash assistance of Rs. 1400/- after
delivery irrespective of age, birth order, or income group(BPL & APL)
- If an expected pregnant women from urban area gets delivered at
Public Health Facility will get a cash assistance of Rs. 1000/- after
delivery irrespective of age, birth order, or income group (BPL& APL).
-
16.
Child health
Essentialnewborn care at facility – specialized units for
stabilization and care of sick newborn babies
Home based newborn care
Promotion of breastfeeding and timely initiation of
complimentory feeding
Management of cases of severe acute malnutrition at
nutrition rehabilitation centres
Micronutrient supplementation
17.
National iron +initiative
Minimum service package for the management of
anaemia across life stages .
Iron and folic acid (IFA) supplementation.
Pregnant
Lactating women
Children in the age group of 6-60 months.
Adolescents; women in reproductive age group.
18.
Under national iron+initiative, the following age
groups are covered
Bi-weekly 20mg elemental iron and 100 microgram(mcg) folic acid per
ml of liquid formulation and age appropriate de-worming for
preschool children of 6-59months.
Weekly supplementation of 45mg elemental iron and 400 mcg folic
acid per child per day for children from 1st
to 5th
grade in govt. and
govt. aided schools, and at AWC for out of school children ( 6 to 10
years).
Weekly dose of 100mg elemental iron and 500 mcg folic acid with
biannual de-worming in adolescents ( 10-19 years ) under WIFS.
Weekly supplementation for women in reproductive age, pregnant
and lactating women .
19.
Rashtriya Kishor Swasthya
Karyakram(RKSK)
The Ministry of Health & Family Welfare.
Launched on 7th
January, 2014
RKSK has been developed to strengthen the adolescent
component of the RMNCH+A strategy .
20.
Objectives
Improve nutrition.
Improve sexual and reproductive health
Enhance mental health
Prevent injuries and violence
Prevent substance misuse
Prevent non communicable disesase
21.
Services provided
WIFS
Clinics and counselling
Peer educator & adolescent health day
Menstrual hygiene scheme
22.
WIFS
Weekly Iron Folicacid Supplementation.
The programme covers 11.2 crore beneficiaries
8.4 crore in school
2.8 crore out of school beneficiaries.
23.
Salient features ofWIFS
To reduce the prevalence and severity of anaemia
in adolescent population (10-19 years).
24.
Target groups
Schoolgoing adolescent girls and boys in 6th
to 12th
class
enrolled in government / government aided / municipal
schools.
Out of school student
Urban and rural areas
25.
Intervention
Supervised weeklyiron- folic acid supplements 100mg
elemental iron and 500mg folic acid .
Screening of target groups for moderate / severe anaemia
and referring these cases to an appropriate health
facility .
Biannual de-worming (Albendazole 400mg )
26.
Peer Education
Toimprove life skills , knowledge and attitude of
adolescents
Nutrition
Sexual and reproductive health
Conditions for NCDS
Substance misuse, injuries and violence
Mental health.
27.
Adolescent Health Day
One of the strategies to achieve the objectives of the
adolescent health program.
Increase awareness among adolescents, parents and families and
stakeholders
The AHD should be organized in every village .
Once every quarter on a convenient day ( preferably on a
Sunday )
AWCs or community spaces may be – venues for organizing the
AHD.
Services should be offered to all the adolescent target
groups( male/ female; 10-14 and 15-19 age; school going, drop
out; and married adolescents)
Kishori Shakti Yojana
Launched year 2000
Key component of ICDS
Aim- breaking the intergenerational life cycle of
nutritional & gender disadvantage and providing a
supportive environment for self development.
30.
Objectives
To improvenutritional and health status of girls in age group of
11-18 years.
To provide required literacy and numeracy skills through the
non- formal stream of education .
To stimulate a desire for more social exposure and knowledge
and to help them improve their decision making capabilities.
To train and equip the adolescent girls to improve / upgrade
home –based and vocational skills.
To promote awareness of health, hygiene, nutrition family
welfare, home management and child care.
To gain a better understanding of their environment related
social issues and the impact on their lives.
31.
IFA supplementationalong with deworming.
Education for school dropouts and functional literacy
among illiterate adolescent girls.
Non formal education to adolescent girls.
Emphasis on life education aspects including physical,
developmental and sex education is given.
Nutrition programme foradolescent girls
It was initiated as a pilot project 2002-03
Centrally sponsored scheme.
51 identified districts across the country.
AIM- address the problem of under-nutrition among
adolescent girls.
35.
Objectives
To improvenutritional status.
To create gender awareness and development of
adolescent girls.
36.
Beneficiaries
Adolescent girls(11-15 years) with body weight less than
30kg.
Adolescent girls(15-19 years) with body weight less than 35kg.
Eligibilty criteria:
adolescent girls(11-19 years)-registered in an Anganwadi
centres irrespective of Financial status of the family to which
they belong.
37.
Benefits
Improvement ofnutritional and health status of girls.
Training and equipment of adolescent girls to upgrade
home based vocational skills.
6kg of free food grain (rice) per month per beneficiary.
Promotion of health, hygiene, nutrition, family welfare,
home management and childcare.
Better understanding of their environment related social
issues and its impact on their lives.
Objectives
To changenegative family and community attitudes
towards the girl child at birth and towards her mother.
To improve enrollment and retention of girl children in
schools to increase the age of marriage of girls and to
assist the girl to undertake income generation activities.
40.
Beneficiaries
Girl childrenbelonging to families below the poverty line.
Who are born on or after 15th
august 1997.
The benefits are restricted to two girl children in a household
irrespective of number of children in the household.
A post birth grant amount of Rs 500.
Payment: attaining 18 years of age.
Girl getting married <18yrs she will not be given the benefit.
In case of death all money will be withdrawn.
41.
National AIDS ControlProgramme
It was launched in the year 1987.
The government forming the national AIDS
committee(NAC) headed by the union health secretary.
National AIDS Control Organization(NACO) 1992 is a
organization of govt of India under the Ministry of Health
and Family Welfare with the primary objective to control
the epidemic in India.
GOAL- effective containment of the infection levels of
HIV/ AIDS in the general population in order to achieve
zero-level of new infections by 2007.
42.
AIDS prevention andcontrol strategy
focuses on following areas:
Program management
Surveillance and Research.
Information, Education and communication including social
mobilization through Non-Governmental Oragnization(NGOs),
Control of sexually transmitted diseases,
Condom Programming.
Blood safety.
Reduction of impact.
43.
The Adolescence Education
Programme(AEP)
Co-curricular adolescence education in classes 9th
-11th
Life skills education in classes 1st -8th
.
Inclusion of HIV prevention education in pre- service and
in-service teacher training and teacher education
programmes.
Inclusion of HIV prevention education – out of school
adolescents and young persons.
Incorporating measures to prevent stigma, discrimination
against learners/ students and educators.
Services provided
Consellingand curative services
Counselling services –
- Nutrition
- Puberty
- RTI / STI prevention
- Contraception and delaying marriage
46.
Curative Services availableat AFHC
Treatment of severe malnutrition
Treatment of common RTI/STI problems
Treatment of menstrual disorders
Treatment of sexual concerns of male and female
Mental health service/management of depression
47.
Treatment ofnon communicable diseases like
Hypertension , Stroke , cardiovascular diseases , diabetes
and other common ailments
Management of injuries related to accidents and violence
48.
Other important services
Delay first pregnancy
Decrease teenage pregnancies
Reduction in maternal deaths among adolescent girls.
Management of anaemia :-
1. Iron supplementation and nutritional counselling.
2. Appropriate health facility referrals.
3. Early and safe abortion services are provided to
adolescents.
4. Reduction in incidence of sexually transmitted diseases and
proportion of HIV positive cases in adolescent.
49.
Commodities available atAFHC
Weekly iron and folic acid supplementation & albendazole.
Sanitary napkins
Contraceptives.
Medicines.

![Adolescent health programmes
1. RMNCH+A
2. Rashtriya Kishor Swasthya Karyakram[RKSK].
3. Kishori Shakti Yojana: to improve the health and nutritional
status of girls.
4. Nutrition Programme for Adolescent Girls[NPAG].
5. Balika Samridhi Yojana.
6. WIFS
7. National AIDS Control Programme.
8. Adolescent Friendly Health Clinics[AFHCs]](https://image.slidesharecdn.com/adolescenthealthprogrammes-250409102515-147cbca9/85/ADOLESCENT-HEALRTH-PROGRAMME-AND-ITS-GUIDELINES-9-320.jpg)



































![HEALTH_CARE_DELIVERY_SYSTEM[1] 2(1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/healthcaredeliverysystem11-251113170857-854694f1-thumbnail.jpg?width=640&height=640&fit=bounds)






































