• WHO definesadolescents as young people aged 10-19 years
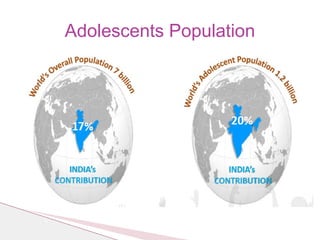
• One fifth of world’s population is in this group(about 1.2 billion)
• Four out of five live in developing countries
❖ Early adolescence (10-13 years)
❖ Mid-adolescence (14-16 years)
❖ Late adolescence(17-19 years)
ADOLESCENTS
1. Physical Development
2.Emotional Development
3. Social Development
Developmental characteristics of
adolescents
5.
1. Psychological issues(depression/low self esteem)
2. Health issues such as anaemia, under/over nutrition
3. Anxiety about pubertal issues, stress etc
4. SRH issues menstrual problems, early and unwanted
pregnancy, symptoms of RTIs/STIs, HIV/AIDS
5. Injury and Violence i.e. sexual assault, domestic
violence, RTA etc.
6. Use of tobacco, alcohol and other substances
Possible health implications of adolescent
development
6.
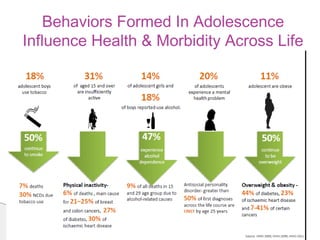
• Lifestyle andbehaviour are linked to 20-25% of the
global burden of disease
• By 2020, non-communicable diseases are expected to
account for 7 out of 10 deaths in the developing
regions
• More than 33% of the disease burden and almost
60% of premature deaths among adults can be
associated with behaviour or conditions that began or
occurred during adolescence
• According to WHO, around 50% of deaths are
reported due to RTA among adolescents (Global status report on road safety,
2018, WHO).
Burden Of Disease
7.
• Comprehensive andcorrect knowledge about HIV
in adolescents aged 15–19 years in India
- 28.20% (males)
- 18.50% (females)
UNICEF. Global and Regional trends 2021
• Adolescent HIV prevalence in India 0.22%
• Adult HIV prevalence 0.25% among males and at
0.19% among females (Source: HIV Estimation 2017)
• ↑ TotalFertility Rate
• Low Contraceptive prevalence rate
• ↑ MMR
• ↑IMR
• ↑ Under 5 mortality rate
• High abortion rate
• High STI/HIV incidence/prevalence rate
Indicators affected by adolescent
sexuality
17.
• Early diagnosis
•Antenatal care
• Counseling during pregnancy
• Management of labor and delivery
• Post partum care
Role of health sector regarding
adolescent pregnancy
18.
• Delay inseeking abortion
• Negative attitude of service providers
• Resorting to untrained providers
• Use of dangerous methods
• Laws restricting to abortion
• Service delivery factors
• Complications following spontaneous abortion
Factors contributing to post abortal
complications in adolescents
19.
• To inculcatehealthy habits and lifestyle
• To reduce morbidity and mortality in adolescents
• To impact national indicators like high TFR, MMR, &IMR,
arrest HIV epidemic
• A healthy adolescent grows into a healthy adult
• Economic benefits
• As a human right they have a right to achieve optimum level
of health
Reasons for investing in adolescent health and
development
20.
• Launch date7/1/2014
• In 231 districts
• Expanded the scope
• Changed the Approach
Rashtriya Kishor Swasthya
Karyakram: A Paradigm Shift
21.
A. Realigns theexisting clinic-based curative approach
Focuses on
- Community based health promotion and preventive
care (PE,AHD,WIFS,MHS)
- Strengthening of preventive diagnostic and curative
services across levels of the health facilities
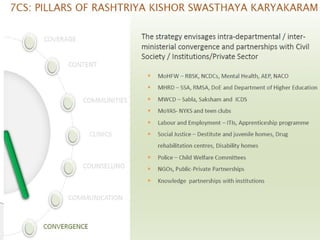
B. A convergent model of service delivery to secure and
strengthen mechanism for access and relevance
RKSK
22.
Operates in fourmajor areas
Individual
Family
School
Community
By providing comprehensive package of
Information
Commodities
Services
RKSK
23.
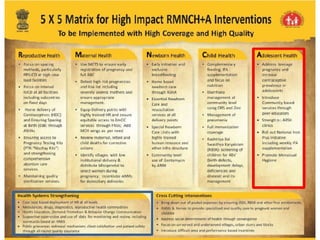
1. Improve nutrition
-Reduce the prevalence of malnutrition among
adolescent girls and boys (including overweight/obesity)
- Reduce the prevalence of iron-deficiency anaemia (IDA)
among adolescent girls and boys
2. Enable sexual and reproductive health
- Improve knowledge, attitudes and behaviour, in relation
to SRH
- Reduce teenage pregnancies
- Promote healthy menstrual hygiene practices among
adolescent girls
- Improve birth preparedness, complication readiness and
provide early parenting support for adolescent parents
Objectives of AH Strategy
24.
3. Enhance mentalhealth
- Address mental health concerns of adolescents
4. Prevent injuries and violence
- Promote favourable attitudes for preventing injuries and
violence (including GBV) among adolescents
5. Prevent substance misuse
- Increase adolescent’s awareness of the adverse effects
and consequences of substance misuse
6. Address conditions for NCDs
- Promote behaviour change in adolescents to prevent
NCDs such as cancer, diabetes, cardio- vascular diseases
and strokes
Objectives of AH Strategy
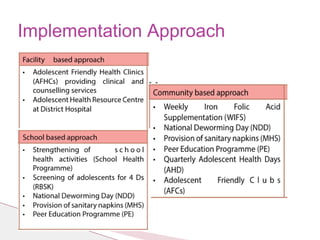
1. Adolescent nutrition;iron and folic acid supplementation
(WIFS)
2. Community based ARSH
(Peer educator and AHD)
3. Facility-based adolescent friendly health services
(Adolescent friendly health clinics)
4. Menstrual hygiene
5. Preventive health checkups(RBSK)
Priority interventions
37.
(National Nutrition MonitoringBureau 2006, shows that
adolescent boys and girls consume only 32-45% of RDA of Iron
and only two thirds of recommended calories)
Common Factors
-Conditioning factors
- Cultural Factors
- Socio-economic factors
- Gender Issues
- Factors specific to adolescents
Factors influencing nutrition of adolescents
38.
• Communication onconsumption of balanced diet, nutritious food
• Nutrition education sessions
- at the community level
- to be included in school curriculum
• Nutritional counselling on a dedicated quarterly Adolescent
Health Day
• Linkages with MWCD (SABLA scheme) and MoHRD (Mid-Day
Meal Programme)
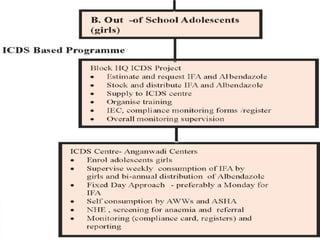
1. Adolescent Nutrition and Folic Acid
Supplementation
40.
• A community-basedintervention
• Objective
◦ To reduce the prevalence and severity of anaemia in adolescent
population (10-19 years)
• Target Group
◦ Covers both boys and girls from rural and urban areas
◦ Adolescents enrolled in class VI–XII of government, government
aided and municipal schools as well as ‘out of school’ girls
(through AWC)
◦ The WIFS programme also covers married adolescent girls
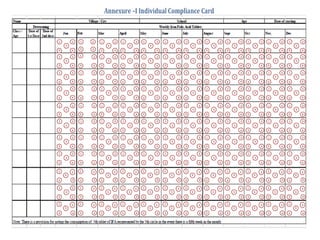
Weekly Iron and Folic acid
Supplementation Scheme(WIFS)
41.
1. Supervised administrationof supplement of 60 mg
elemental iron and 500 mcg folic acid
2. Bi-annual de-worming (Albendazole 400 mg)
NDD on 10th
February and 10th
August
3. Information and counselling for improving dietary intake
and preventive actions for intestinal worm infestation
4. Screening of target groups for moderate and severe
anaemia and referral to an appropriate health facility
WIFS – Interventions
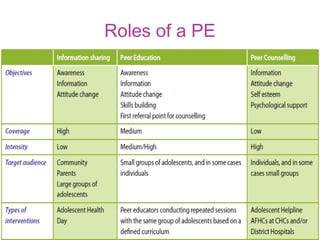
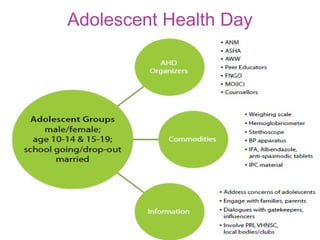
46.
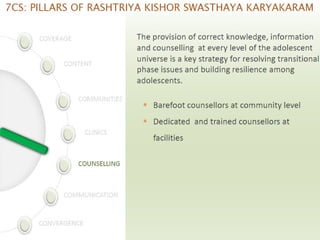
• Information andcounselling on ARSH and other
health issues
• To improve knowledge, attitude and behaviours
• Life Skills Education- through educational
institutions and in community settings
- Kishori Samooh
- Teen Club
- Peer Education
- AHD
2. Community based ARSH
47.
◦ In ruralareas four volunteer PE per village
◦ In urban areas four volunteer PE per UPHC
◦ PE should share similar social and demographic
characteristics as their peer group
◦ Trained in existing ASHA training system on AH
◦ Non-financial incentives
◦ Peer Coordinators ( ASHA & ANM)
Peer Education
Barriers
1. Lack ofknowledge about availability of services and means
of access
2. Social and cultural deterrents
3. Perceived lack of privacy or confidentiality
4. Services are difficult to access
5. Staff appears unfriendly
3. Facility based ARSH (Adolescent Friendly
Health Clinics)
53.
Role of HealthSector
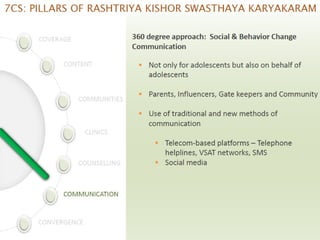
• Provide accurate information to adolescents, families,
media
• Address groups of adolescents/ parents/teachers/schools
• Provide services in a friendly manner
• Facilitate provision of life skills education, delaying age of
marriage
Facility based ARSH (Adolescent Friendly
Health Clinics)
54.
Key friendly characteristics
FromUser Perspective
◾Accessible
◾Acceptable
From Provider’s Perspective
◾Appropriate
◾Comprehensive
◾Effective
◾Equitable
Facility based ARSH (Adolescent
Friendly Health Clinics)
55.
Structure of AFHCservices
• Service Providers: Adequate, appropriate, competent
• Location, ambiance, and supplies
• Guidelines and Procedures
• IEC and resource materials
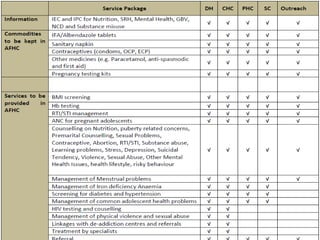
56.
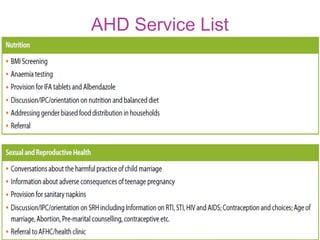
Package of AFHCservices
1. Focused care during the antenatal period
2. Counselling and provision for emergency
contraceptive pills and reversible contraceptives
3. Information/advice on SRH issues
4. Services for Prophylaxis against Nutritional Anaemia
5. Nutrition Counselling
6. Services for early and safe termination of pregnancy
and management of post abortion complications
57.
Package of AFHCservices
7. Treatment for common RTIs/STIs
8. Treatment and counselling for menstrual disorders
9. Treatment and counselling for sexual concerns of male
and female adolescents
10. Management of sexual abuse among girls
11.Linkage with de-addiction centres and referrals
12.Management od sexual violence and abuse
13.Organize and conduct outreach activities
59.
Training of Healthcare providers
• Capacity building includes competency enhancement –
both in clinical skills and interpersonal skills as well as
motivation
• All identified providers will be oriented to ‘How to do’ skills
in training workshops. Their ‘clinical skills’ will be updated
during the standard skills development trainings in RCH-II
for MOs 4 days
for ANM/LHVs 5 days
for counsellors 6 days
• Infrastructure clean,bright and colorful
• Maintains privacy and confidentiality
• Can be easily accessed by the adolescents
(distance, convenient working hours and cost)
• Adolescents are aware about the clinic and range
of service it provides
• Non judgmental and competent health service
providers
• Community members are aware of the services
provided and understand the need for the same
Benchmarks of an AFHC
62.
• AFHC prescriptionfor every adolescent visiting the
AFHC, with a registration number. Counsellor will
fill up the initial findings, followed by doctor filling in
treatment details. The AFHC prescription will be
kept by the adolescent
• Enrollment and clinical register for registering
adolescents who have come to the AFHC. This
should
• Counselling register maintained by the Counsellor
• Stock register (existing format used in the PHC).
This would be maintained by the health assistant
(female) at the registration desk
Monitoring
63.
• Adolescent girlsin the age group of 10-19 year in
rural areas
Objectives of the scheme:
• To increase awareness among adolescent girls on
Menstrual Hygiene
• To increase access to and use of high quality
sanitary napkins to adolescent girls in rural areas.
• To ensure safe disposal of Sanitary Napkins in an
environmentally friendly manner.
4. Menstrual Hygiene Scheme
64.
• Under thescheme a pack of 6 sanitary napkins is
provided under the NRHM’s brand ‘Freedays’
• Initially implemented in 17 states
• Sold @ Rs. 6 for a pack of 6 napkins in the village
by the ASHA
• Door to door sale, AWC
• On sale of each pack, the ASHA gets an incentive
of Rs. 1 per pack besides a free pack of sanitary
napkins per month.
Menstrual Hygiene Scheme
65.
• This initiativewas launched in February 2013
• To improve the overall quality of life of children
• To provide comprehensive care to all the children
in the community
• Screening of children from birth to 18 years of age
for four Ds
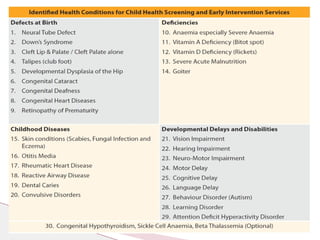
• Spanning 32 common health conditions for early
detection and free treatment and management,
including surgeries at tertiary level
5.RBSK
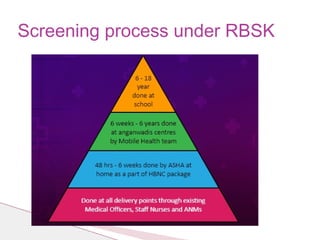
• Facility level:
Alldelivery points through existing MOs, SNs and ANMs at
birth
• Community level:
ASHA at home as a part of Home Based New-born Care
(HBNC) for 48 hrs to 6 weeks
Mobile Health teams at -AWC for 6 weeks to 6 years
-Govt. aided schools for 6-18 years
• District Early Intervention Centre (DEIC) for 0-6 years age group
• Existing public health facilities for 6-18 years age group
• Treatment/intervention is delivered at zero cost to the family
RBSK- Implementation mechanism




































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)















