2. Differential diagnosis of acute upper airways
obstruction
Common cause
• Viral laryngotracheobronchitis ('croup' - very common)
Rare causes
• Epiglottitis
• Bacterial tracheitis
• Laryngitis
• Retropharyngeal abscess or peritonsillar abscess
• Diphtheria
• IMN causing severe lymph node swelling
• Laryngeal foreign body
• Trauma to the throat
• Inhalation of smoke and hot air in fires
• Allergic laryngeal angioedema (seen in anaphylaxis and recurrent
croup)
• Hypocalcaemia due to poor vitamin D intake
3. BACTERIAL TRACHEITIS
(pseudomembranous croup)
• It is a rare but dangerous condition.
• It may occur as an isolated disease or as a complication of
viral URTI e.g. croup.
• It is similar to severe viral croup except that the child has a
high fever, appears toxic and has rapidly progressive
airways obstruction with copious thick airway secretions.
• It is caused by infection with Staphylococcus aureus.
• Treatment is by intravenous antibiotics and intubation and
ventilation if required.
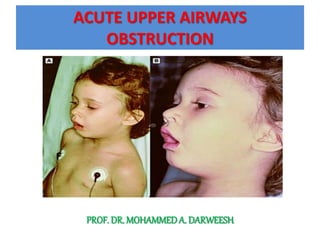
6. ACUTE EPIGLOTTITIS
• A life-threatening emergency due to the high risk of respiratory
obstruction.
• It is caused by H. influenzae type b.
• The introduction Hib vaccine decrease the incidence of
epiglottitis and other invasive H. influenzae type b infections by
99%. Therefore, Streptococcus pyogenes, Streptococcus
pneumoniae, Staphylococcus aureus, and non typeable H.
influenzae, are the main causes of epiglottitis in vaccinated
children.
• There is intense swelling of the epiglottis and surrounding
tissues.
• It is associated with septicaemia.
• Epiglottitis is most common in children aged 1-6 years but it can
affect all the age groups.
7. • It is a very important to distinguish clinically
between epiglottitis and croup as they require quite
different treatment.
• The definitive diagnosis of epiglottitis requires
visualization of a large, cherry red, swollen
epiglottis by laryngoscopy.
• laryngoscopy should be performed urgently in a
controlled environment such as an operating room
or intensive care unit.
12. Croup vs. Epiglottitis
CROUP EPIGOTTITIS
Onset Over days Over hours
Appearance Unwell Toxic, very ill
Preceding coryza Yes No
Cough Severe, barking Absent or slight
Stridor Harsh, rasping Soft, whispering
Voice, cry Hoarse Muffled, reluctant to
speak
Drooling saliva No Yes
Able to drink Yes No
Fever <38.5°C >38.5°C
13. Treatment
• Epiglottitis is a medical emergency required immediate treatment
with an artificial airway.
• Establishing an airway by nasotracheal intubation or, less often, by
tracheostomy is indicated in patients with epiglottitis, regardless of
the degree of apparent respiratory distress, because as many as 6%
of children with epiglottitis without an artificial airway die,
compared with <1% of those with an artificial airway.
• Cultures of blood, epiglottic surface, and, in selected cases, CSF
should be collected after the airway is stabilized.
• Racemic epinephrine and corticosteroids are ineffective.
• Ceftriaxone, cefepime , or meropenum should be given parenterally
for at least 10 days.
14. Chemoprophylaxis
Rifampin prophylaxis
(20 mg/kg orally once a day for 4 days; max. dose: 600
mg) for:
• A child within the home who is younger than 4 y. of
age and incompletely immunized.
• A child younger than 12 m. of age and has not
completed the primary vaccination series.
• Immunocompromised.
15.
16. Case History:
• Acute epiglottitis
A 5-year-old girl developed a severe sore
throat, drooling of saliva, a high fever and
increasing difficulty breathing over 8 hours.
• Epiglottitis was diagnosed and her airway was
guaranteed with a nasotracheal tube.
• Antibiotics were started immediately.
• She made a full recovery.
17.
18. Prognosis
• In general, the length of hospitalization and the mortality rate for
cases of acute infectious upper airway obstruction increase as the
infection extends to involve a greater portion of the respiratory
tract, except in epiglottitis, in which the localized infection itself
can prove to be fatal.
• Untreated epiglottitis has a mortality rate of 6% in some series,
but if the diagnosis is made and appropriate treatment is initiated
before the patient is moribund, the prognosis is excellent.
• The outcome of acute laryngotracheobronchitis, laryngitis, and
spasmodic croup is also excellent.
• Children who need to be hospitalized for croup have somewhat
increased bronchial reactivity compared with normal children
when tested several years later, but the significance is uncertain.