Downloaded 191 times




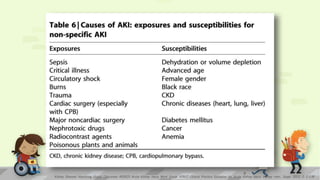
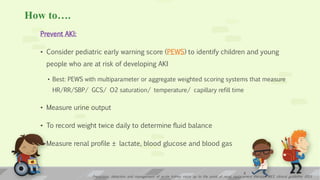
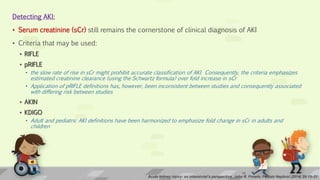
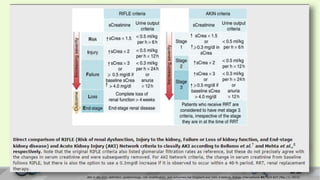
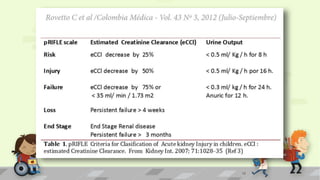
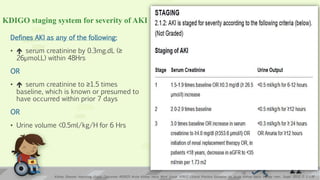
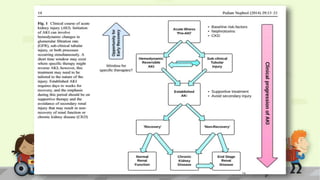

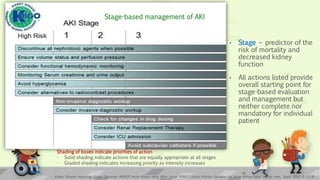
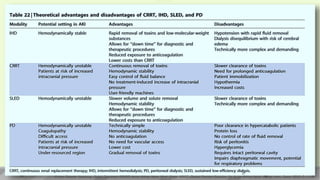

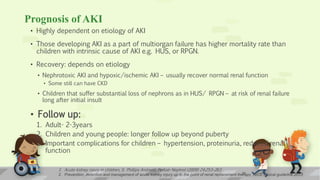

Acute kidney injury (AKI) in children is a reversible increase in creatinine and waste products with impaired kidney function. It has various etiologies like ischemia, toxicity, or multi-organ failure. Early detection using creatinine and urine output is important. Risk assessment considers factors exposing children to AKI. Management includes fluid management to prevent overload, glycemic control, nutrition support, and nephrology referral for severe or unknown cases. Renal replacement therapy may be considered for fluid, metabolic, and other imbalances. Prognosis depends on etiology, with intrinsic causes often having full recovery but multi-organ injury carrying higher mortality.



































































