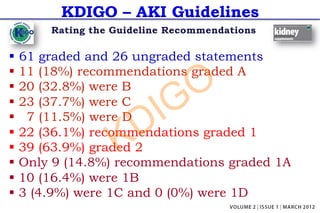
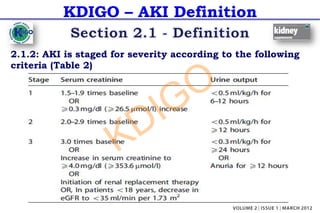
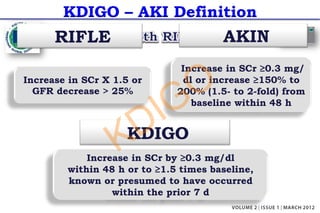
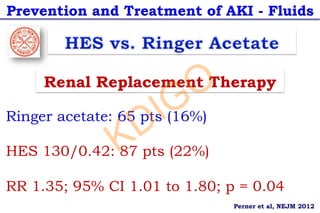
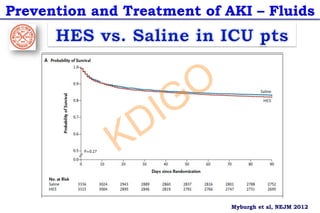
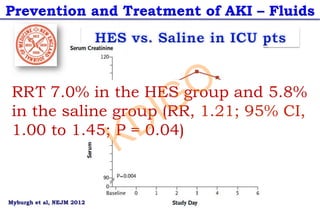
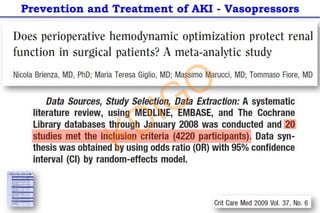
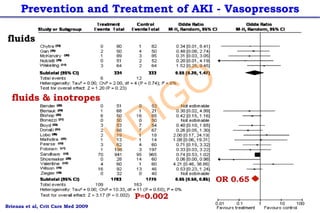
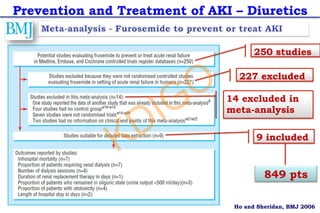
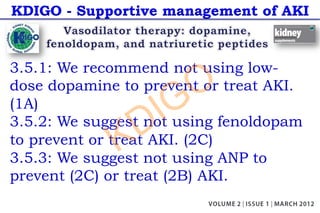
The document summarizes guidelines from KDIGO (Kidney Disease: Improving Global Outcomes) on acute kidney injury (AKI). It describes how the guidelines were developed by an international working group over two years, reviewing over 18,000 citations. The guidelines define AKI and provide recommendations on prevention, evaluation, and management of AKI, including suggesting isotonic crystalloids over colloids for fluid resuscitation; protocol-based management for high-risk perioperative or septic shock patients; and intravenous volume expansion with isotonic fluids to prevent contrast-induced AKI.

![Prevention and Treatment of AKI – Dopamine
Ø 61 trials – 3,359 pts
Ø no effect of low-dose dopamine
Ø Mortality: RR 0.96 [95% CI, 0.78 - 1.19]
Ø Need for RRT: RR 0.93 [CI, 0.76 - 1.15]
Ø Adverse events: RR 1.13 [CI, 0.90 - 1.41]
KDIGO](https://image.slidesharecdn.com/kdigo-aki-guidelinecass-2014-221116192641-e5d231b1/85/KDIGO-AKI-Guideline_Cass-2014-pdf-42-320.jpg)