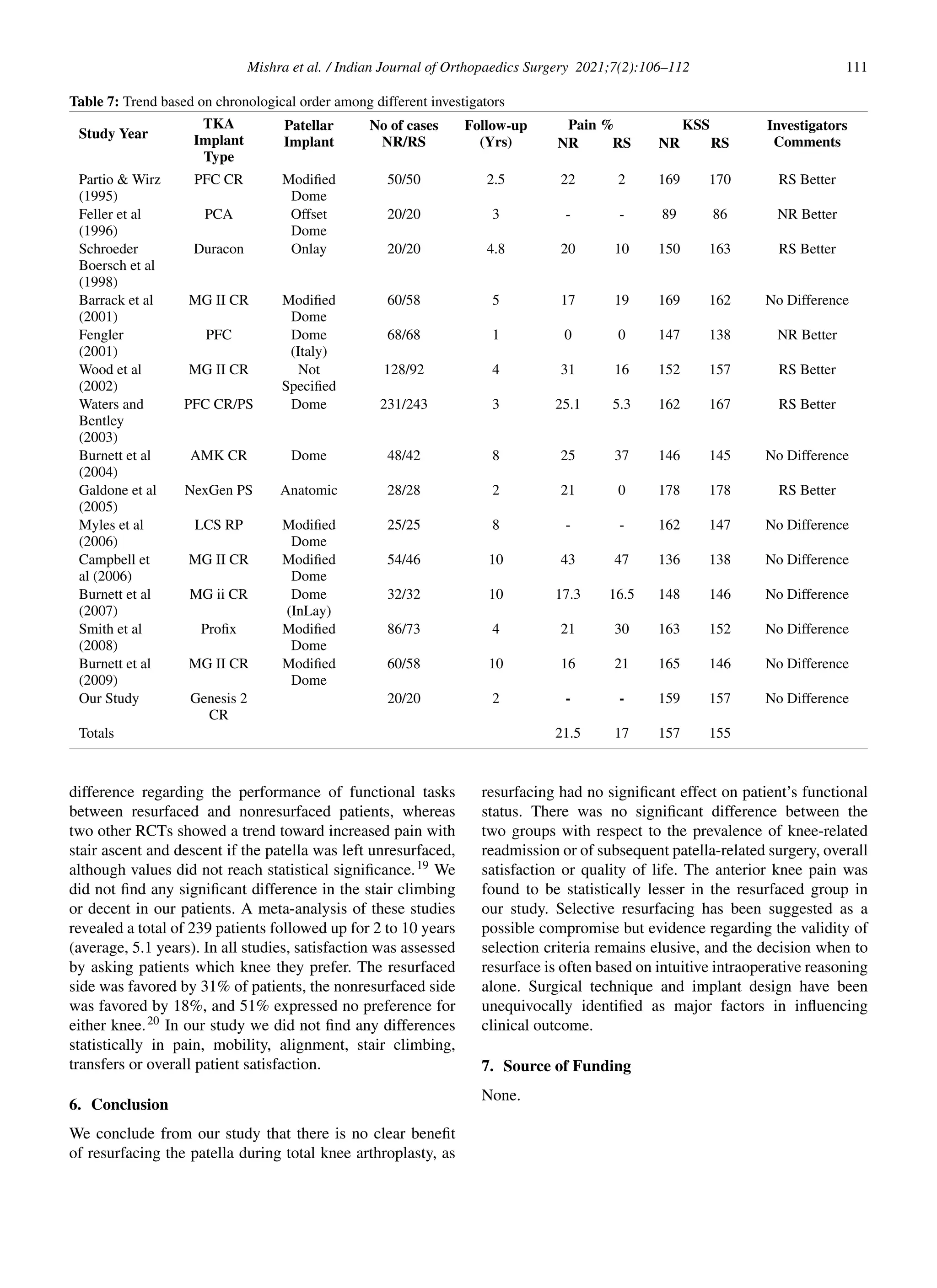
This study compares the outcomes of patellar resurfacing versus non-resurfacing in total knee arthroplasty among a South Indian population, revealing no significant functional differences between both groups after two years. Although anterior knee pain was notably reduced in the resurfaced group, overall patient satisfaction and knee function scores showed no significant disparities. The findings suggest selective patellar resurfacing may be beneficial, particularly for reducing anterior knee pain.