Downloaded 34 times



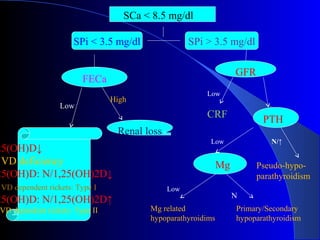
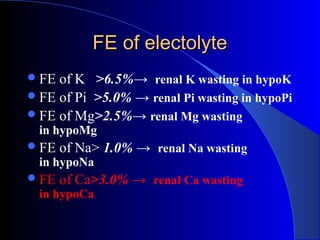
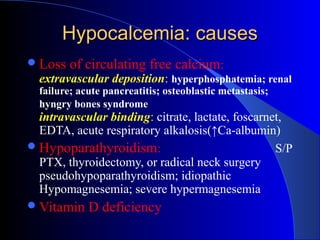

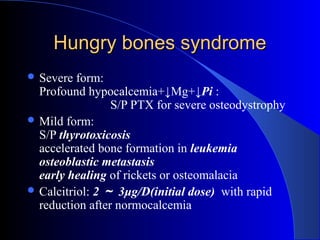






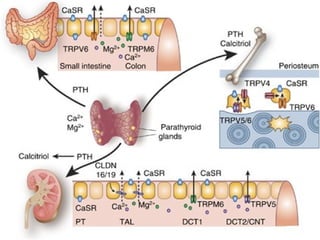
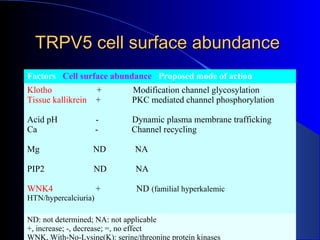
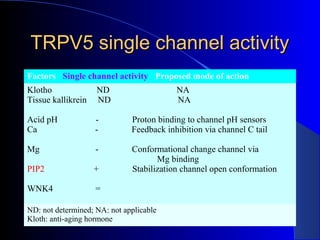
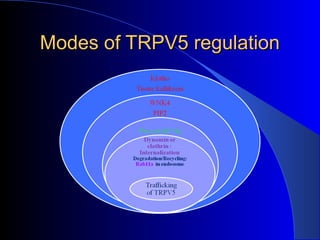
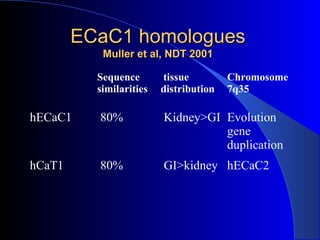




This document provides an overview of hypocalcemia, including: - Causes of hypocalcemia such as hypoparathyroidism, vitamin D deficiency, renal failure, sepsis - Symptoms of hypocalcemia including neurological symptoms, muscle spasms, cardiac issues - Diagnosis and treatment of hypocalcemia including IV calcium supplementation and monitoring calcium levels - Etiologies of hypocalcemia like hungry bone syndrome, acute pancreatitis, medications that can cause hypocalcemia - Overview of calcium regulation in the kidney and genes involved








































































