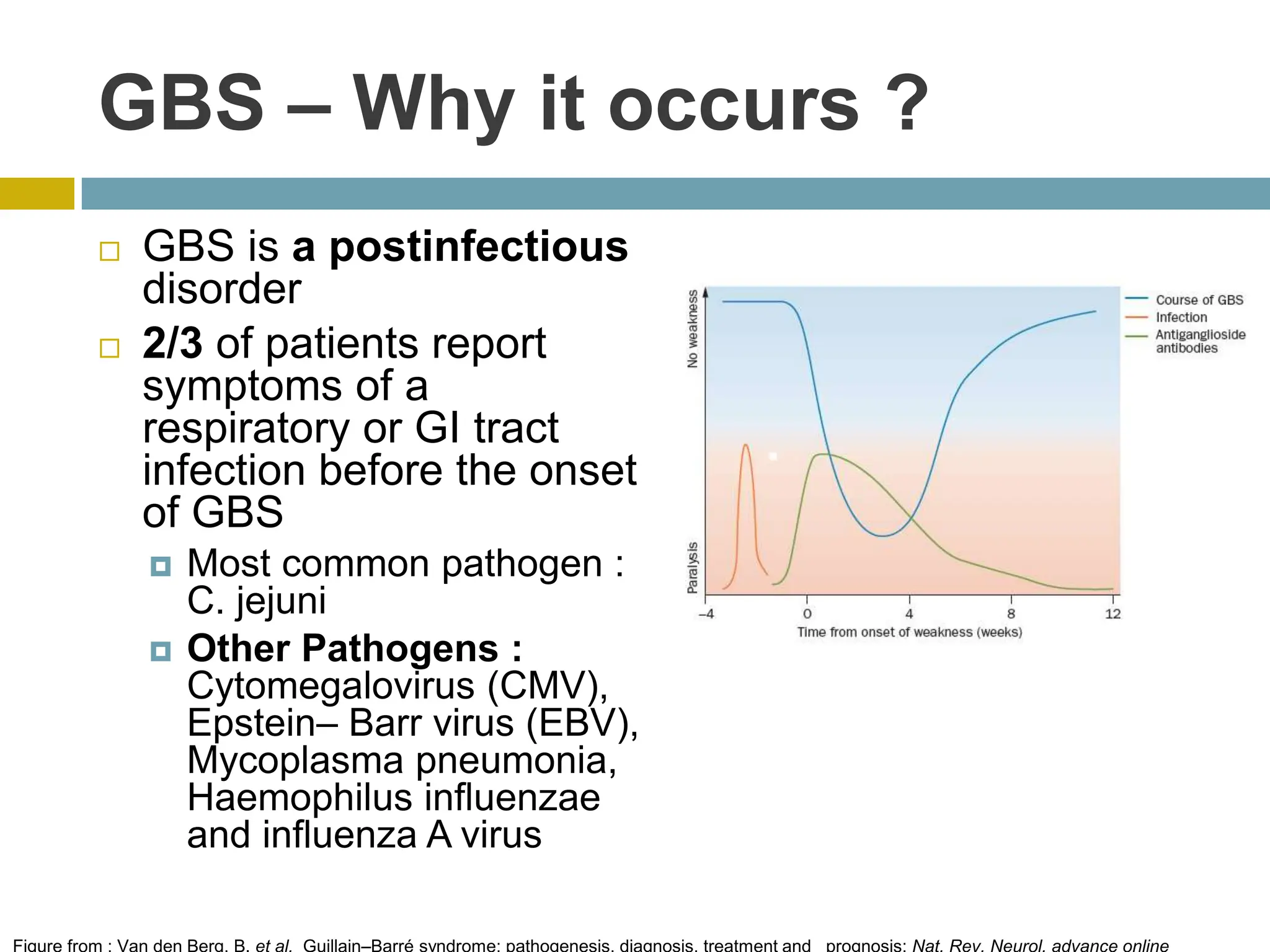
The document outlines Guillain-Barré Syndrome (GBS), its history, types, clinical presentation, pathology, diagnosis, and treatment options, particularly focusing on intravenous immunoglobulin (IVIG) therapy. GBS manifests as an acute inflammatory demyelinating polyneuropathy with various subtypes and is often postinfectious in nature. Current evidence supports IVIG and plasma exchange as effective treatments, with guidelines recommending both for hastening recovery, while noting that IVIG is generally safer and easier to administer.