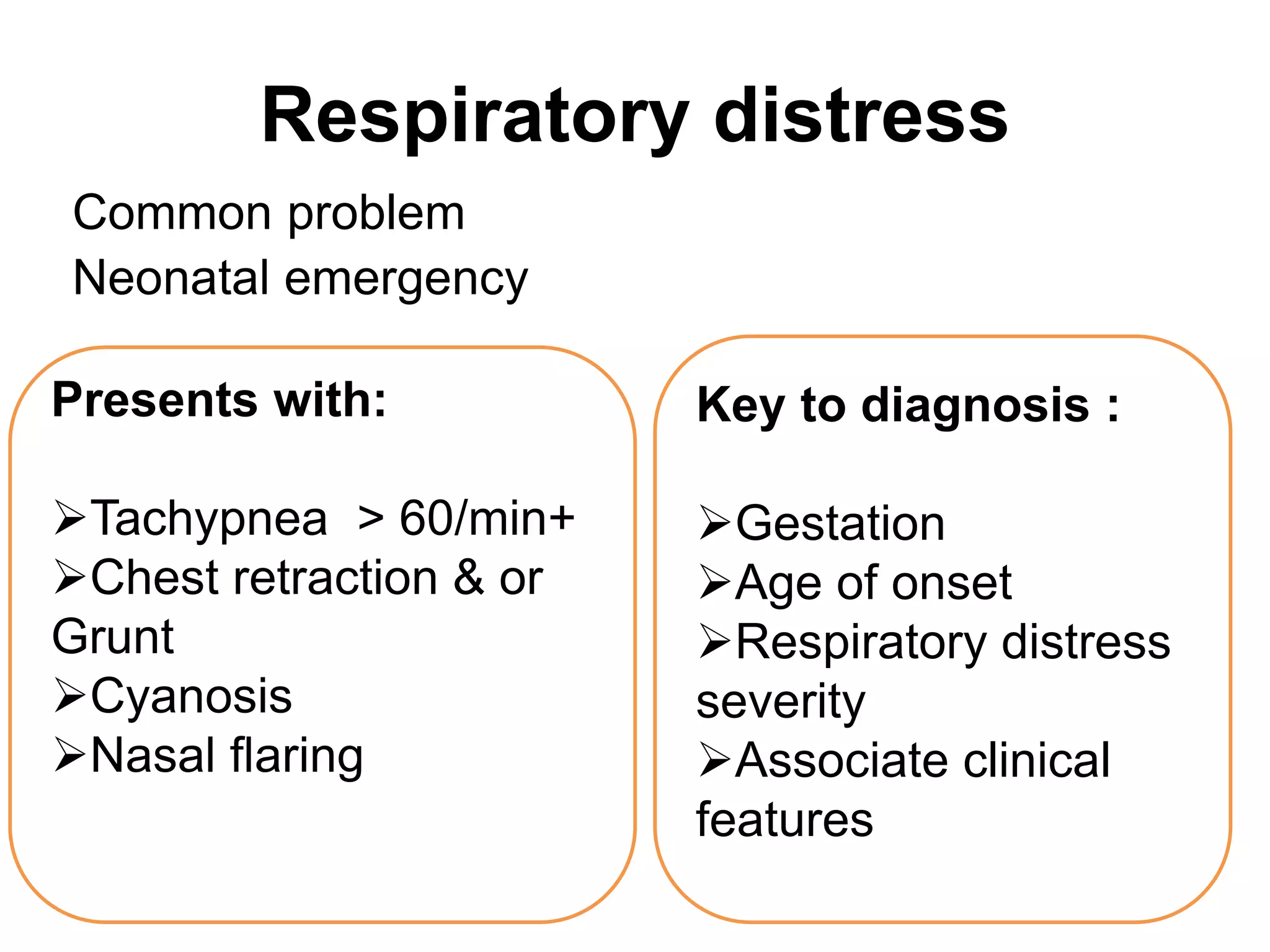
This document discusses respiratory distress in neonates, focusing on respiratory distress syndrome (RDS). It describes the signs, risk factors, pathophysiology, diagnosis, and management of RDS. Surfactant deficiency is the primary cause of RDS. Treatment involves oxygen, CPAP, mechanical ventilation if needed, and surfactant replacement therapy. With advances in care including antenatal steroids and surfactant replacement therapy, mortality from RDS has decreased.