Methods And BiopsyProtocols
IN
Upper Gastrointestinal Endoscopy
Dr. DINESH THAPA
3rd
year MDGP and EM Resident
2.
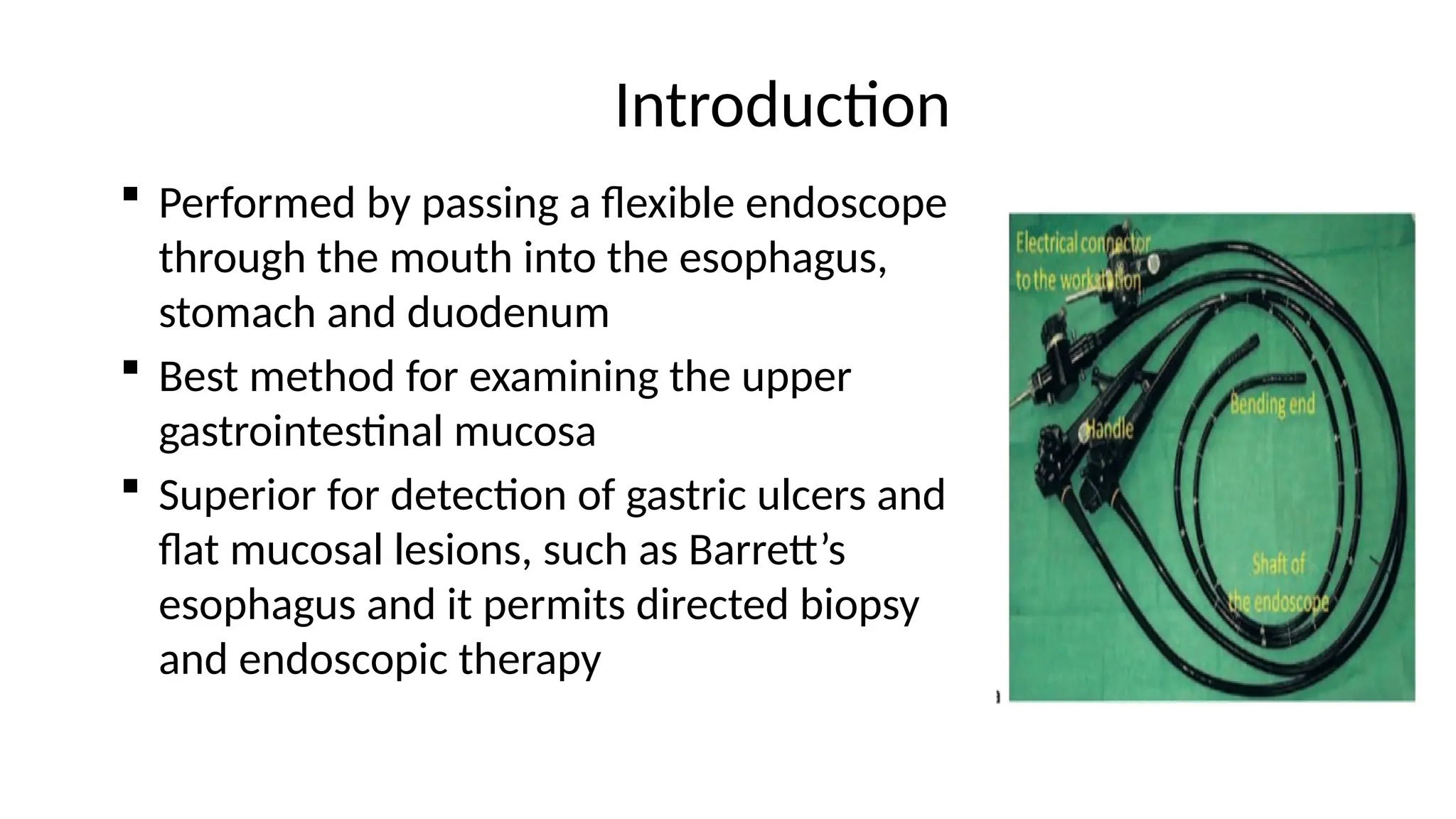
Introduction
Performed bypassing a flexible endoscope
through the mouth into the esophagus,
stomach and duodenum
Best method for examining the upper
gastrointestinal mucosa
Superior for detection of gastric ulcers and
flat mucosal lesions, such as Barrett’s
esophagus and it permits directed biopsy
and endoscopic therapy
3.
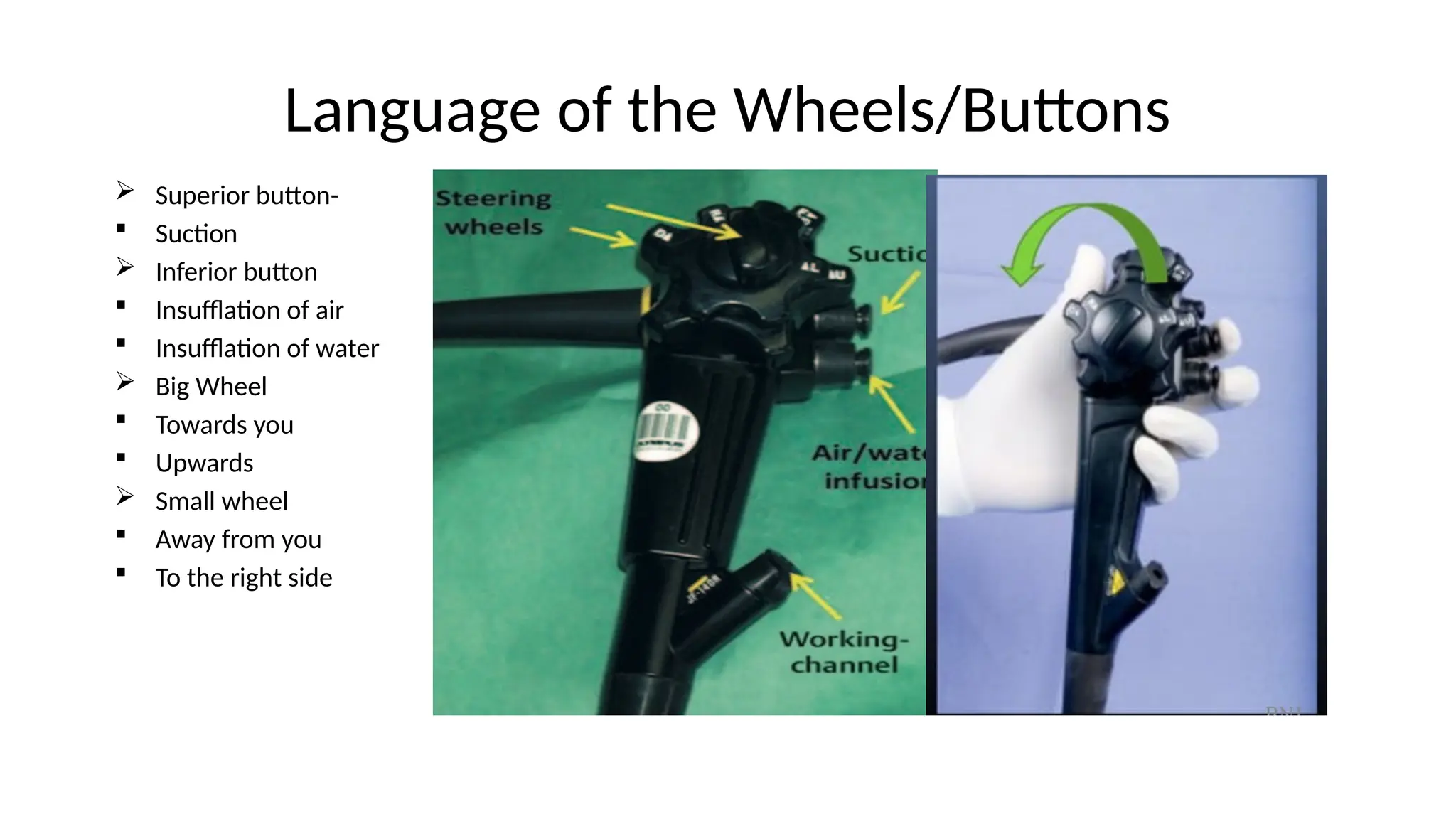
Language of theWheels/Buttons
Superior button-
Suction
Inferior button
Insufflation of air
Insufflation of water
Big Wheel
Towards you
Upwards
Small wheel
Away from you
To the right side
4.
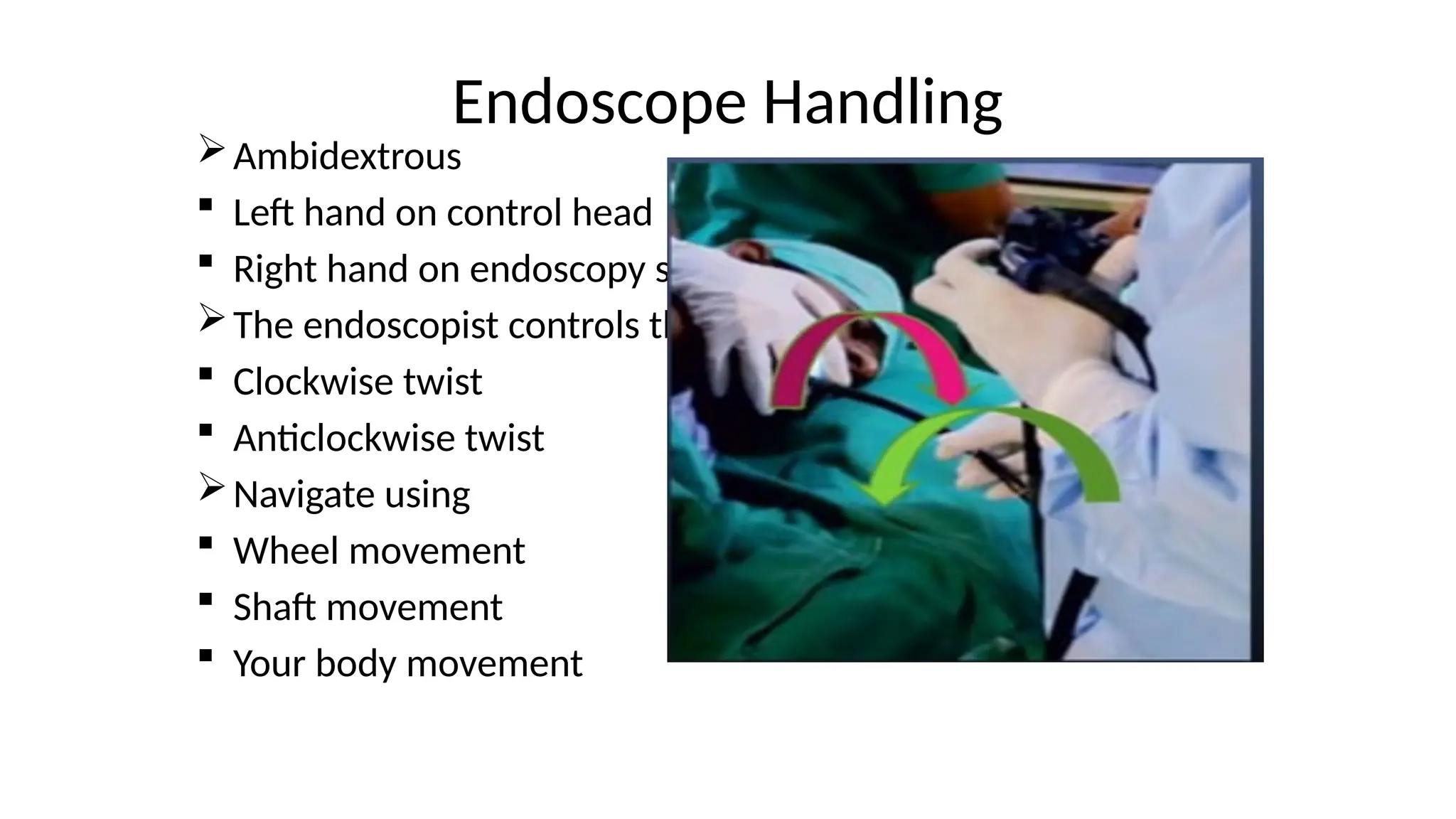
Endoscope Handling
Ambidextrous
Lefthand on control head
Right hand on endoscopy shaft
The endoscopist controls the shaft
Clockwise twist
Anticlockwise twist
Navigate using
Wheel movement
Shaft movement
Your body movement
5.
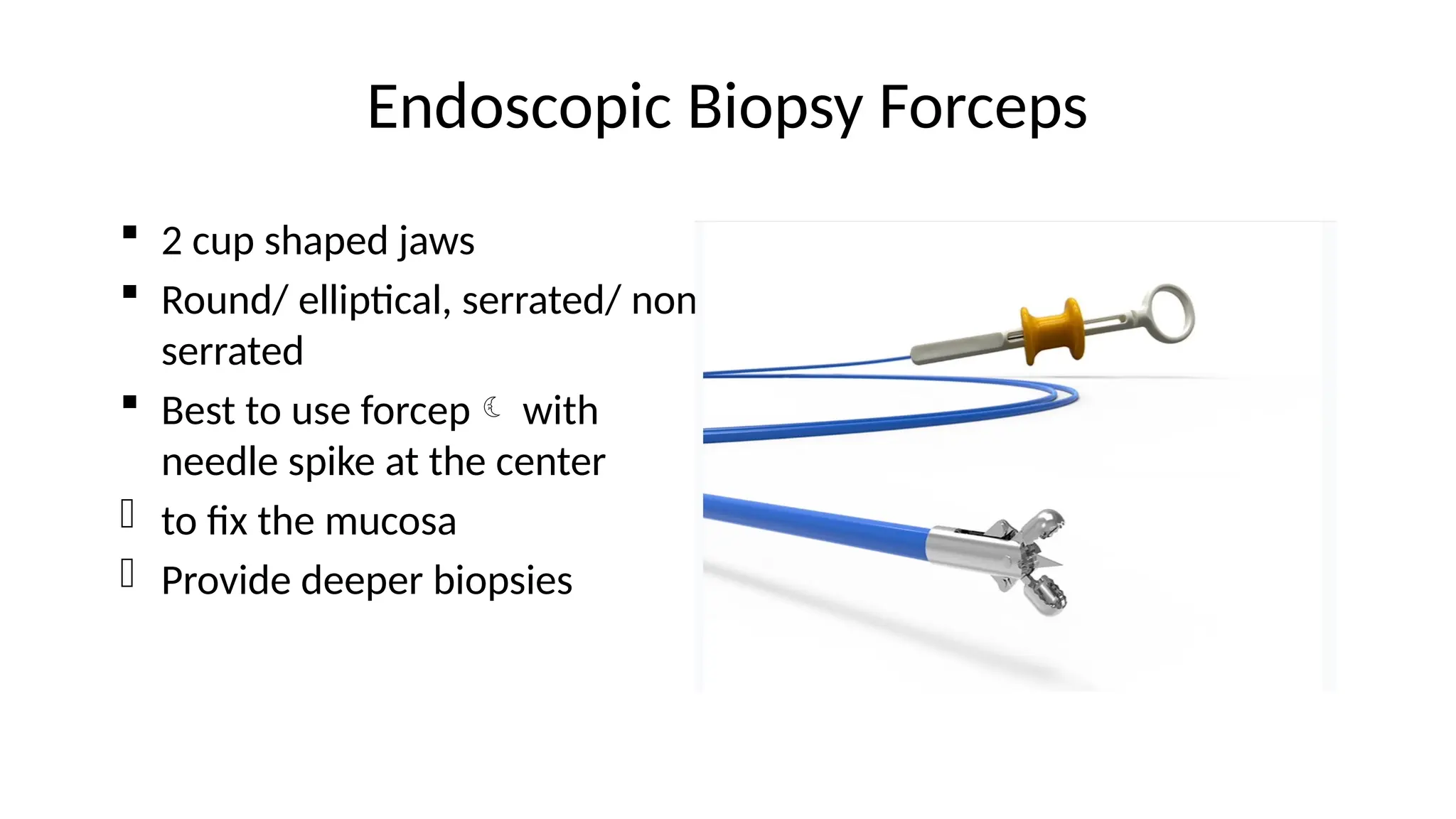
Endoscopic Biopsy Forceps
2 cup shaped jaws
Round/ elliptical, serrated/ non
serrated
Best to use forcep with
needle spike at the center
- to fix the mucosa
- Provide deeper biopsies
6.
Cleaning and Disinfection
Low-level disinfection
Non-critical accessories Come in contact with intact skin
Cameras and endoscopic furniture
Sterilization
Critical reusable accessories
Which enters body cavities and vasculature or penetrate mucous membranes
Biopsy forceps, sclerotherapy needles and sphincterotomes
High- level disinfection
Semi-critical accessories which come into contact with mucous
membranes
Endoscopes and esophageal dilators
7.
Cleaning and Disinfection
Manual disinfection
Soak the instrument and accessories in the chosen disinfectant
Glutaraldehyde – most popular disinfectant
The length of contact time needed for disinfection- 20 minutes
is commonly recommended
More prolonged soaking known or suspected mycobacterial
disease
Peracetic acid, chlorine dioxide, sterox – have also been used
8.
Golden Rules forEndoscopic Safety
• Do not push if you cannot see
• If in doubt, inflate and pull back
9.
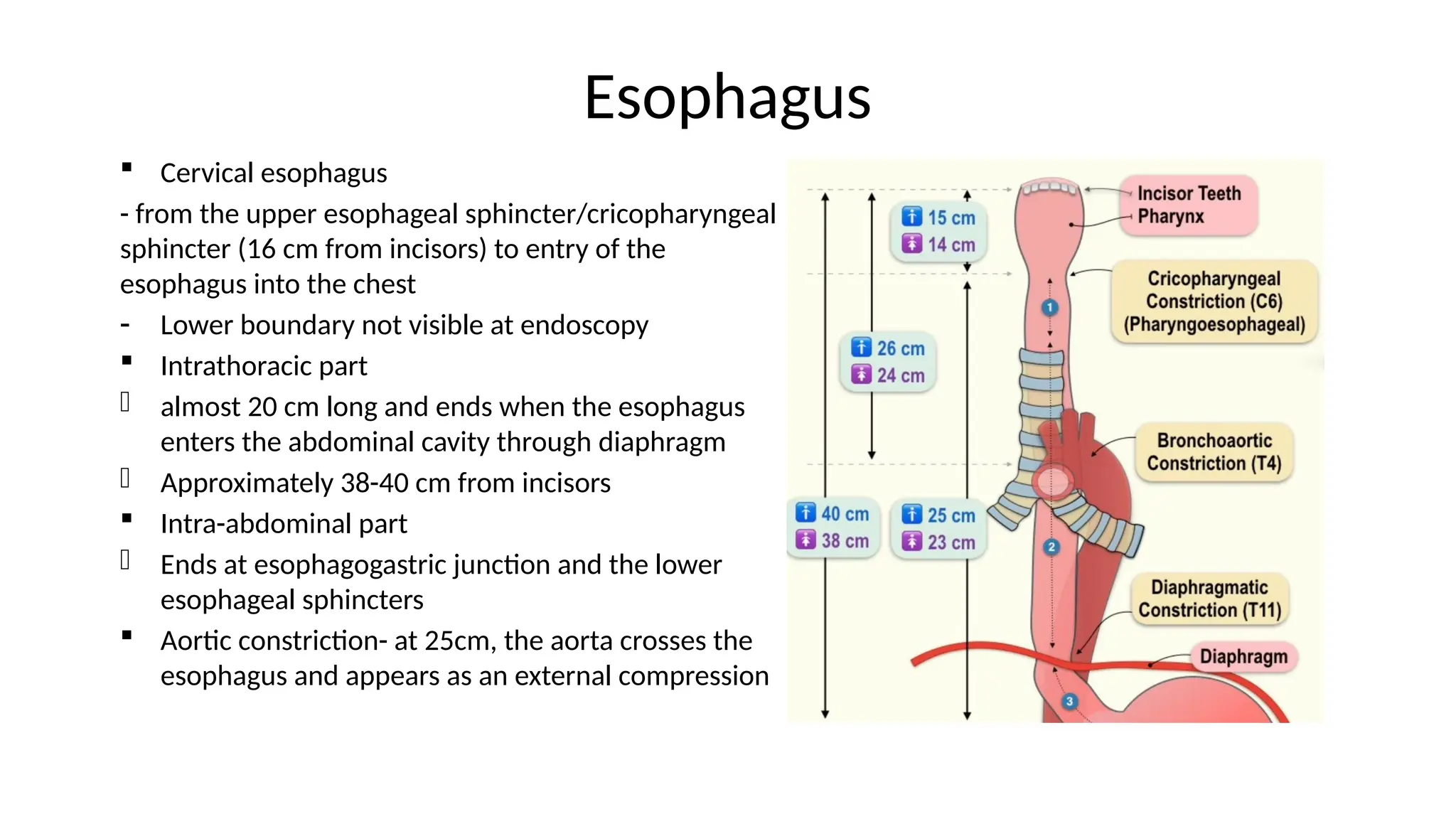
Esophagus
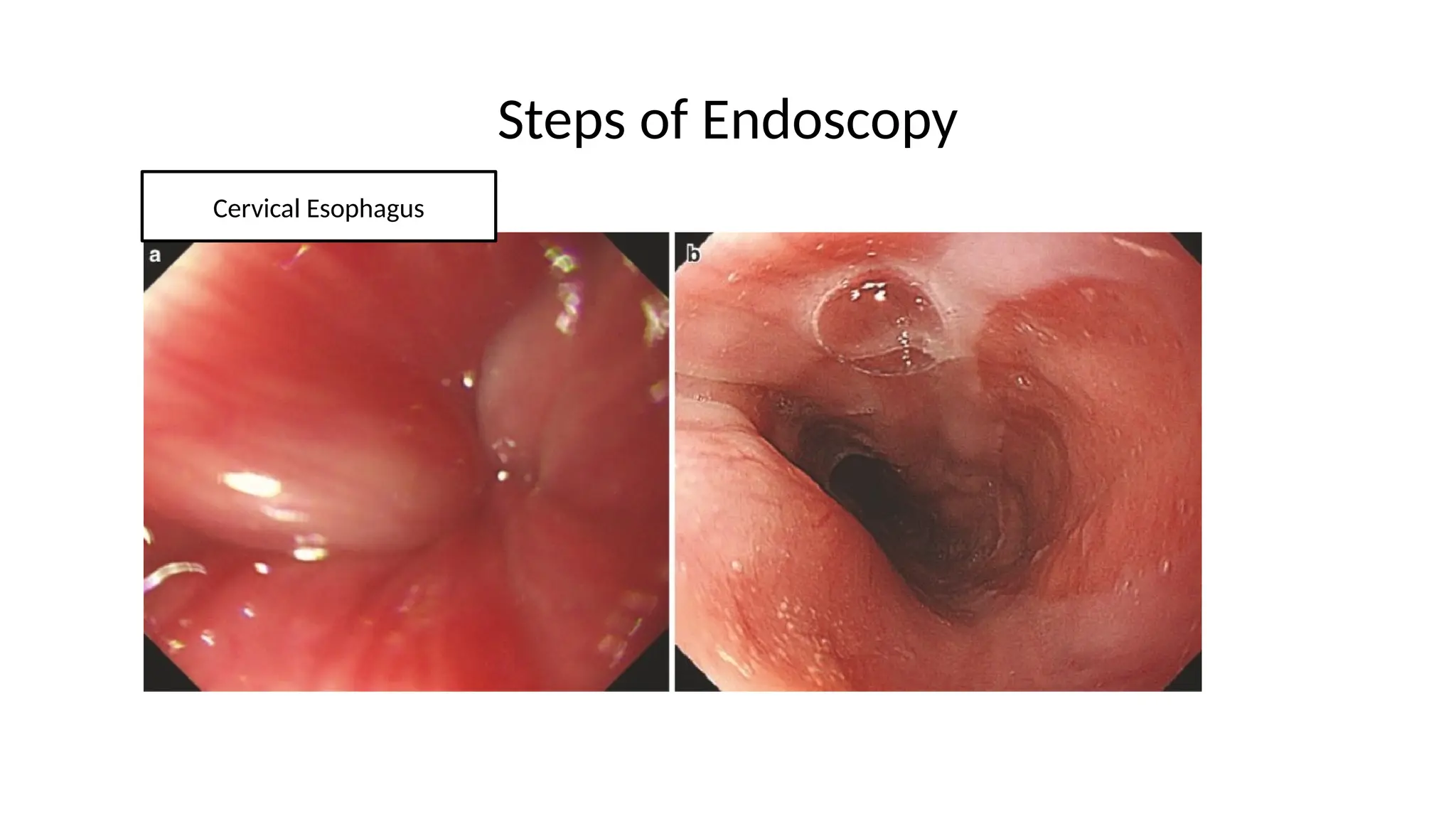
Cervical esophagus
-from the upper esophageal sphincter/cricopharyngeal
sphincter (16 cm from incisors) to entry of the
esophagus into the chest
- Lower boundary not visible at endoscopy
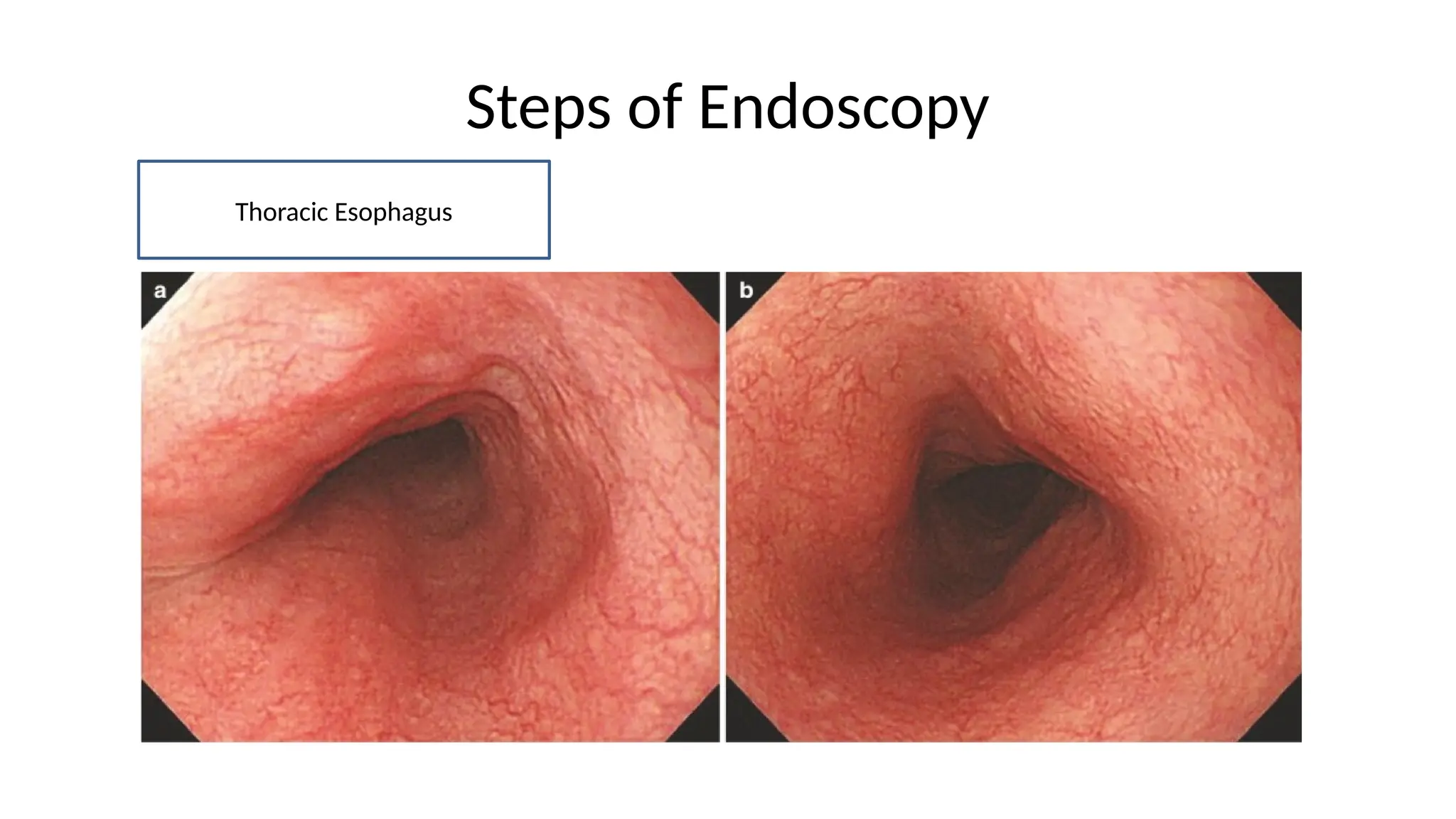
Intrathoracic part
- almost 20 cm long and ends when the esophagus
enters the abdominal cavity through diaphragm
- Approximately 38-40 cm from incisors
Intra-abdominal part
- Ends at esophagogastric junction and the lower
esophageal sphincters
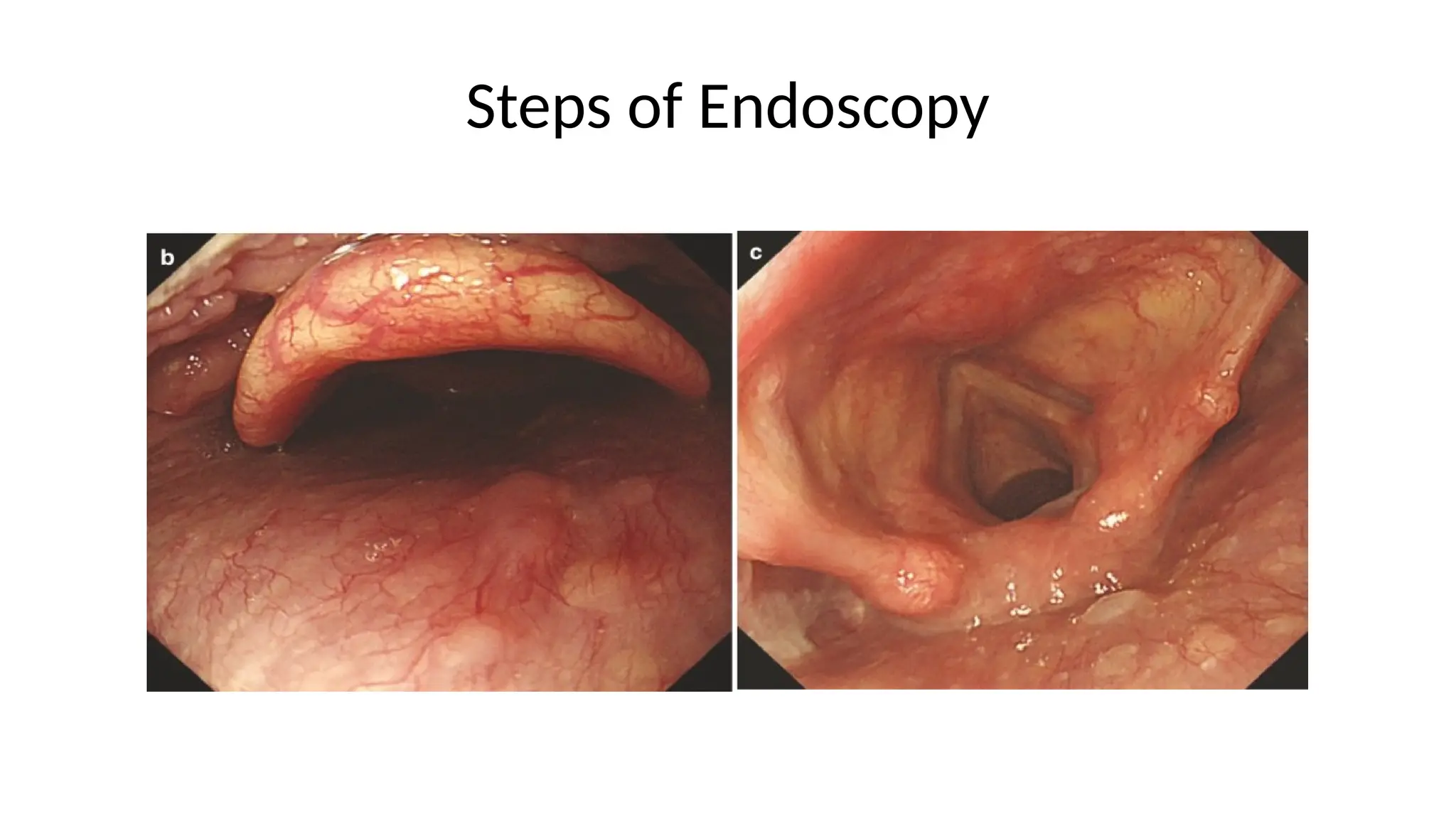
Aortic constriction- at 25cm, the aorta crosses the
esophagus and appears as an external compression
10.
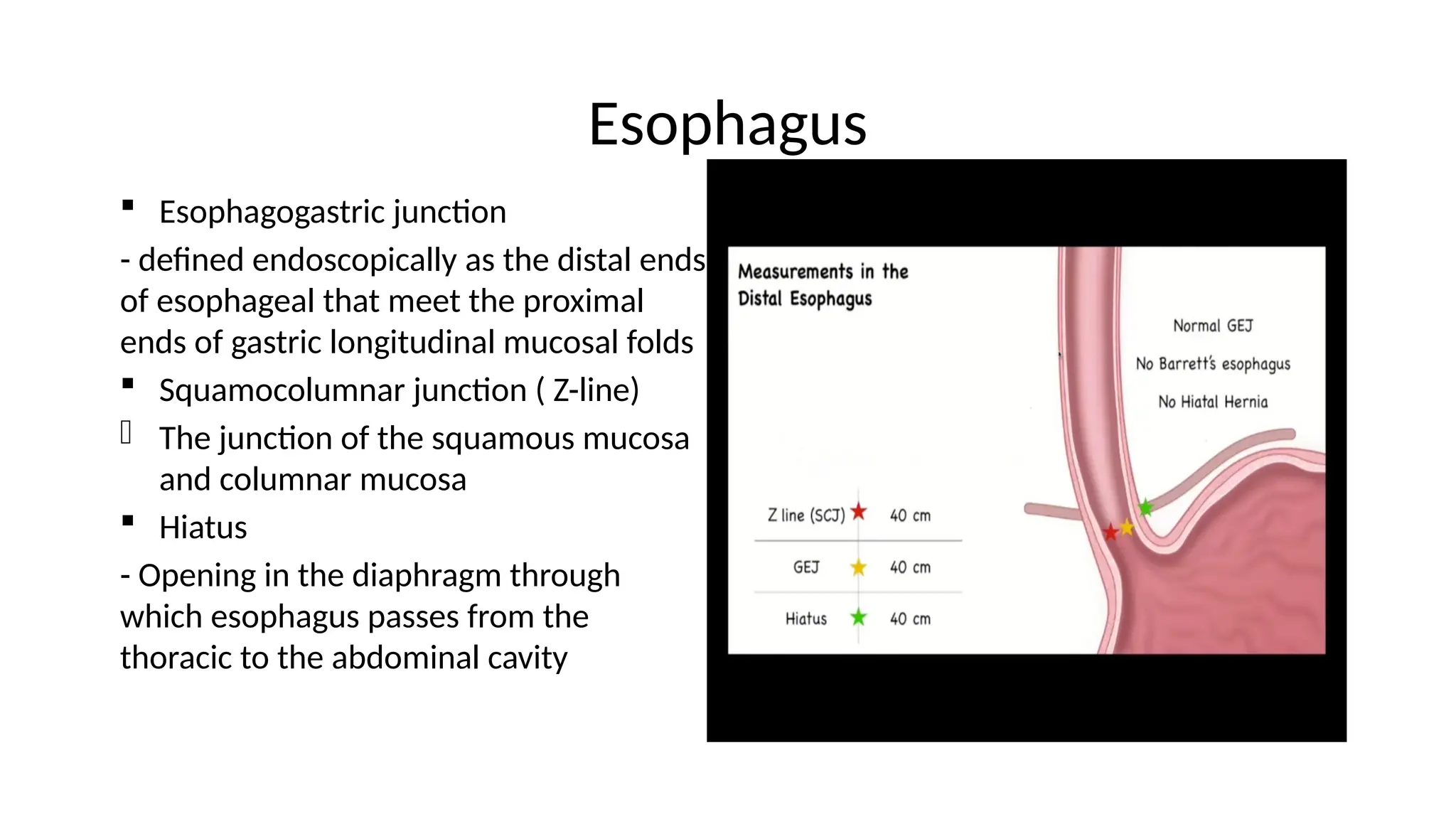
Esophagus
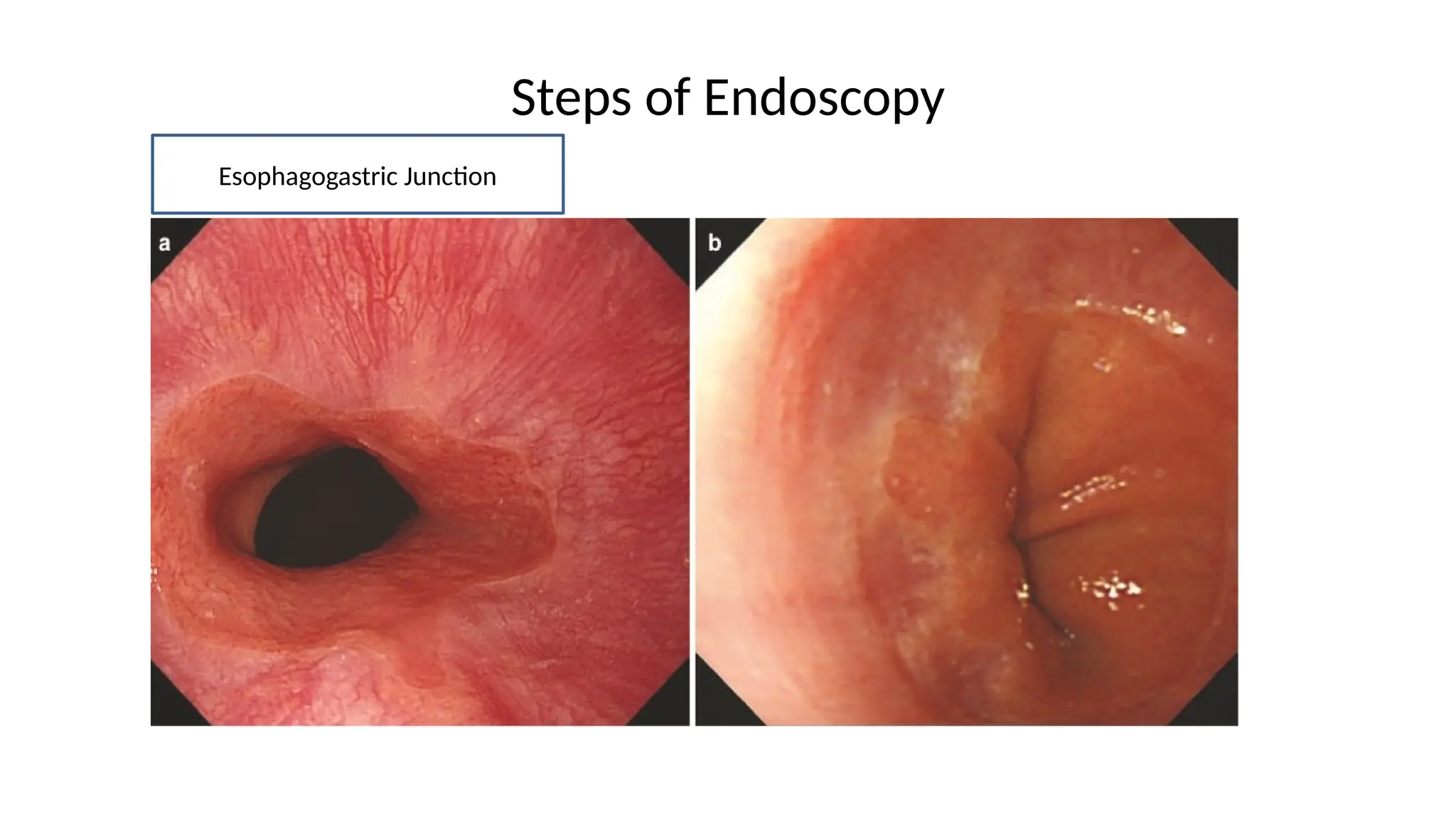
Esophagogastric junction
-defined endoscopically as the distal ends
of esophageal that meet the proximal
ends of gastric longitudinal mucosal folds
Squamocolumnar junction ( Z-line)
- The junction of the squamous mucosa
and columnar mucosa
Hiatus
- Opening in the diaphragm through
which esophagus passes from the
thoracic to the abdominal cavity
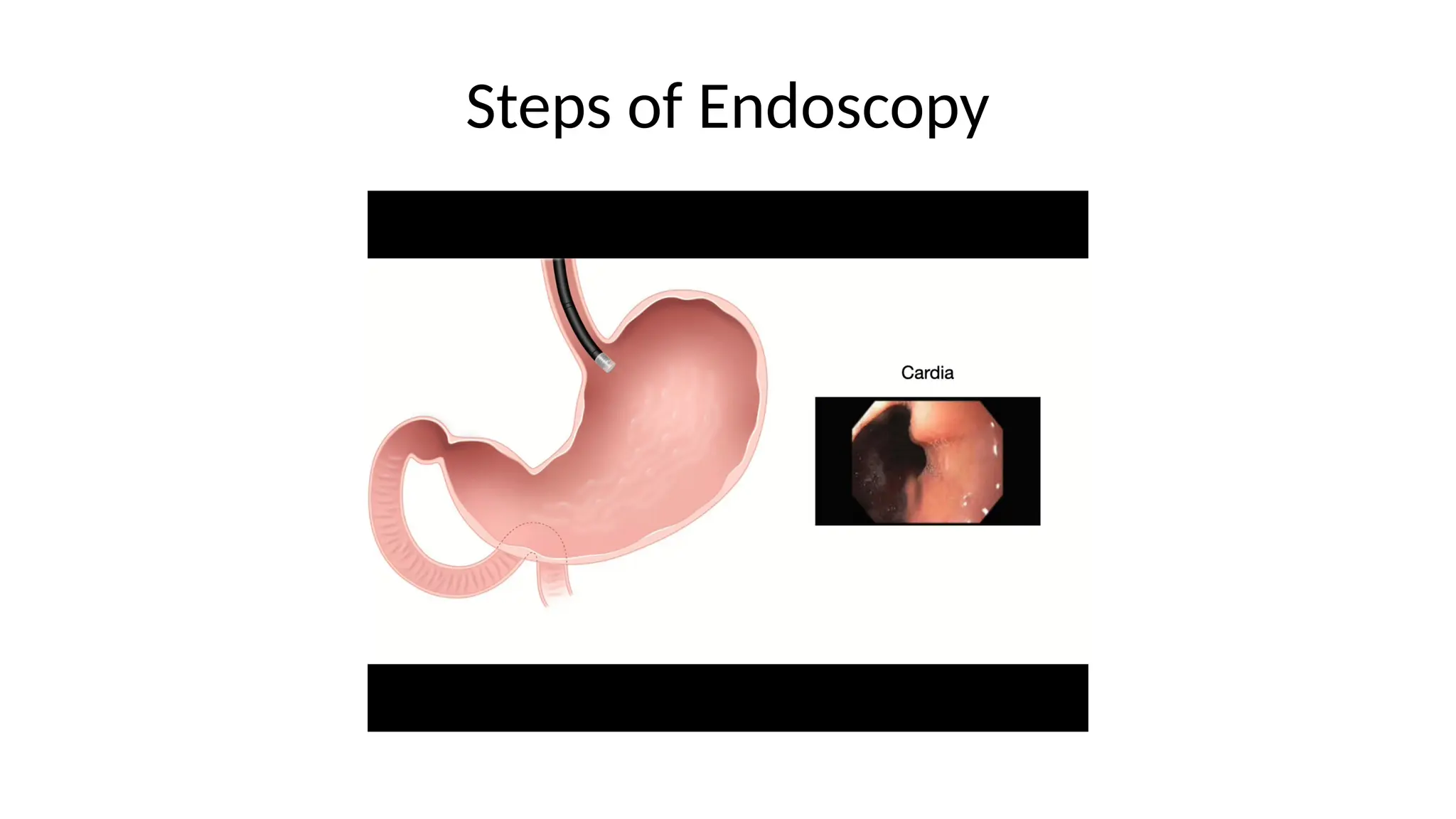
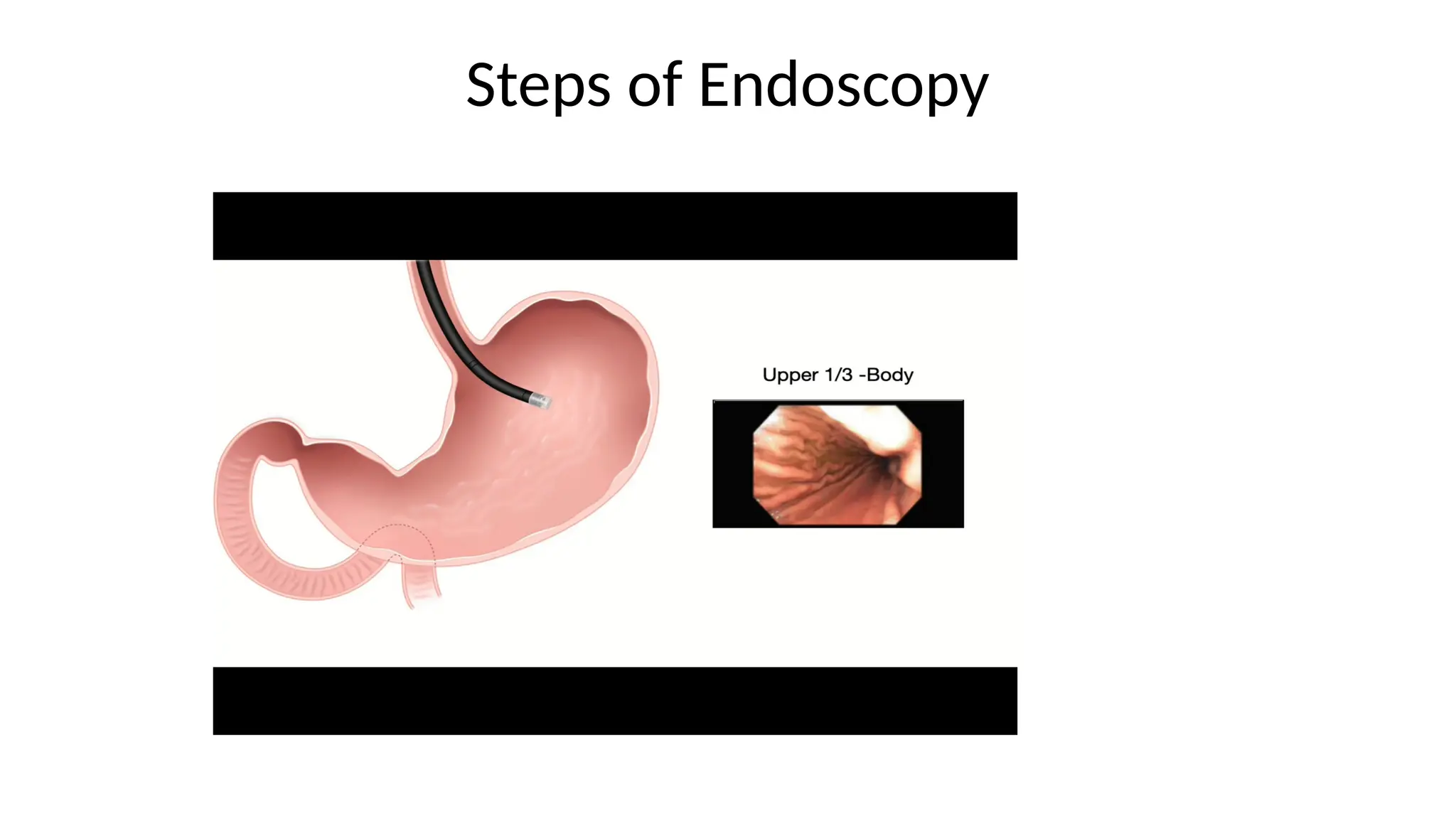
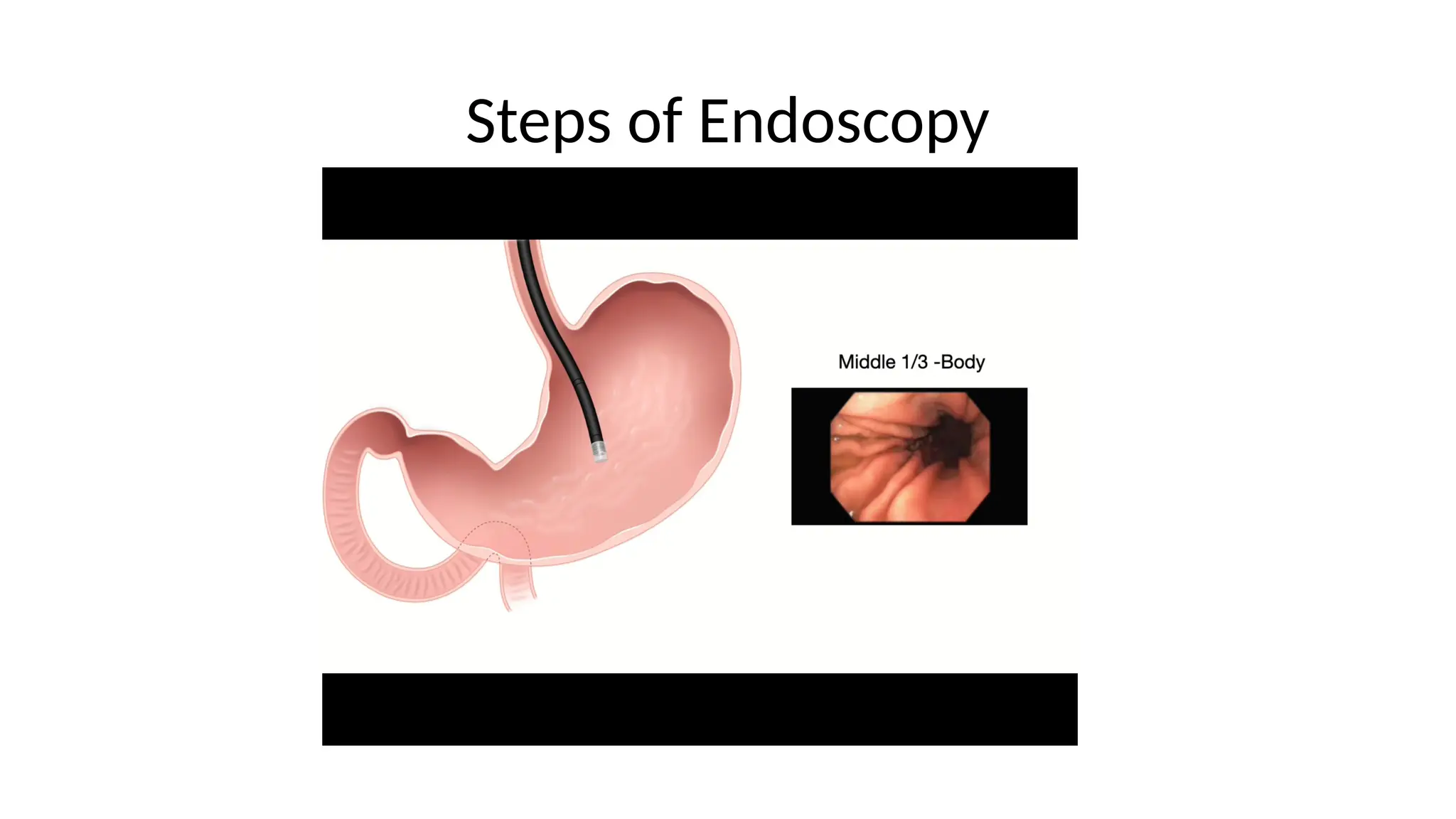
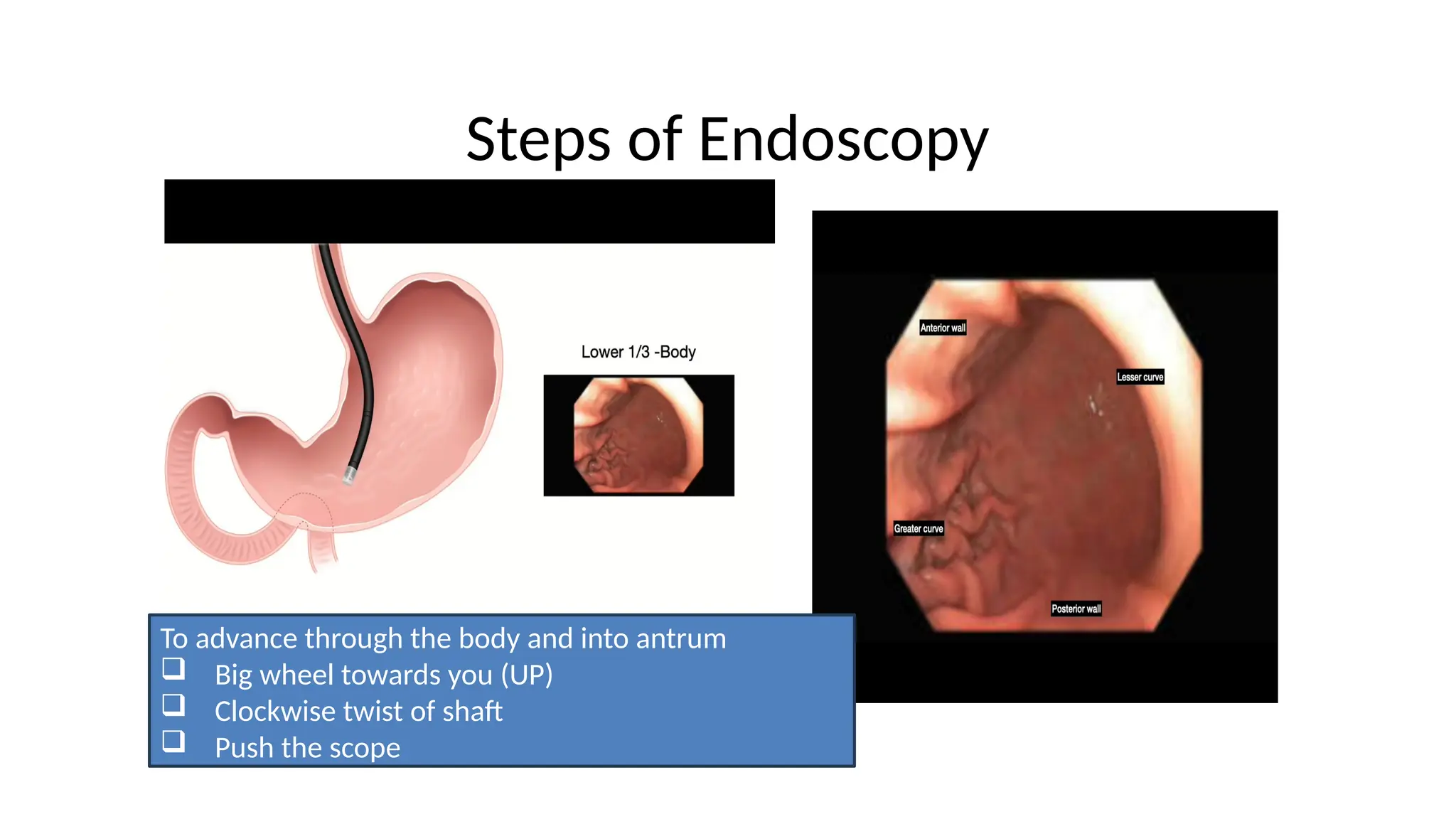
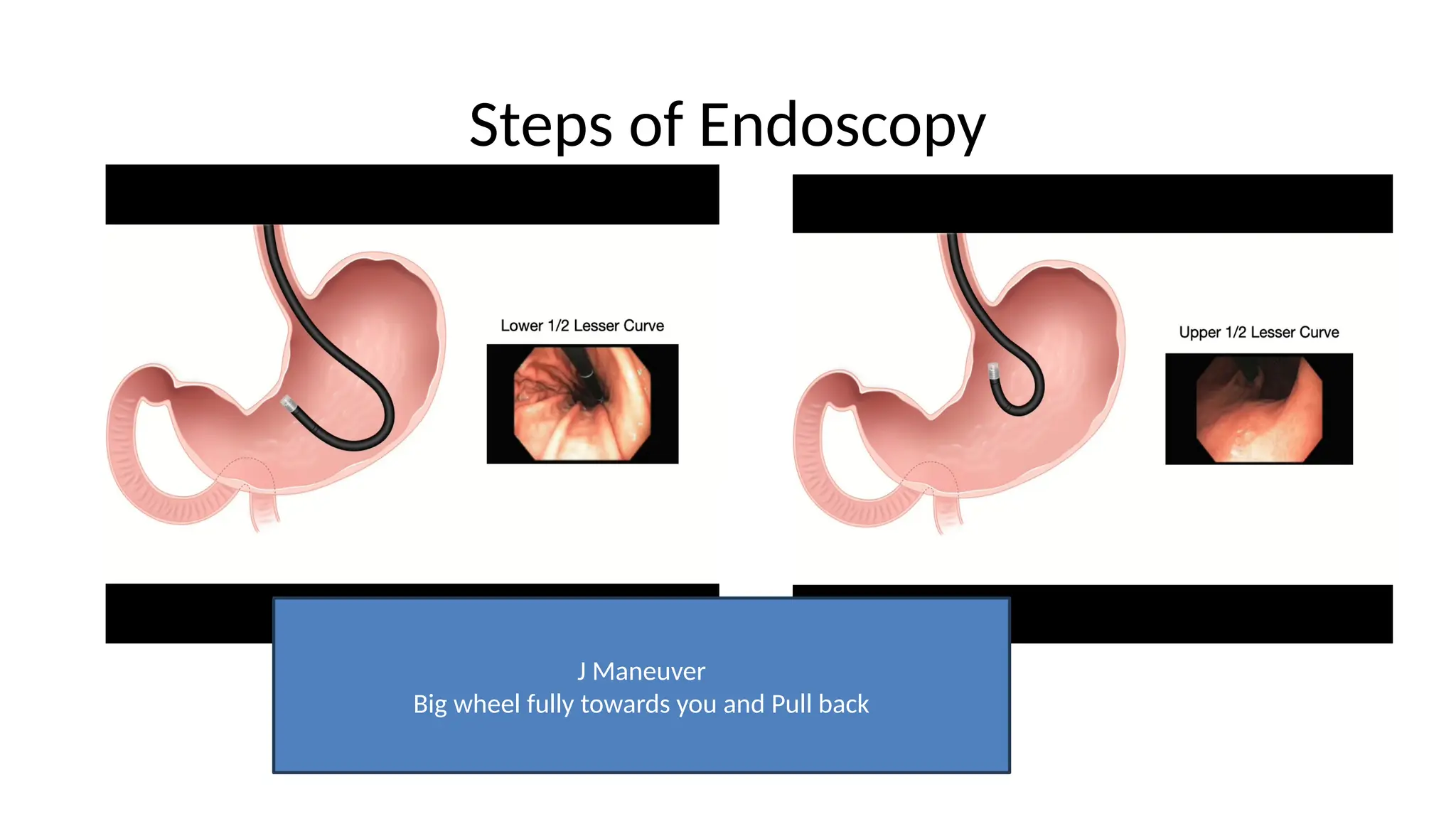
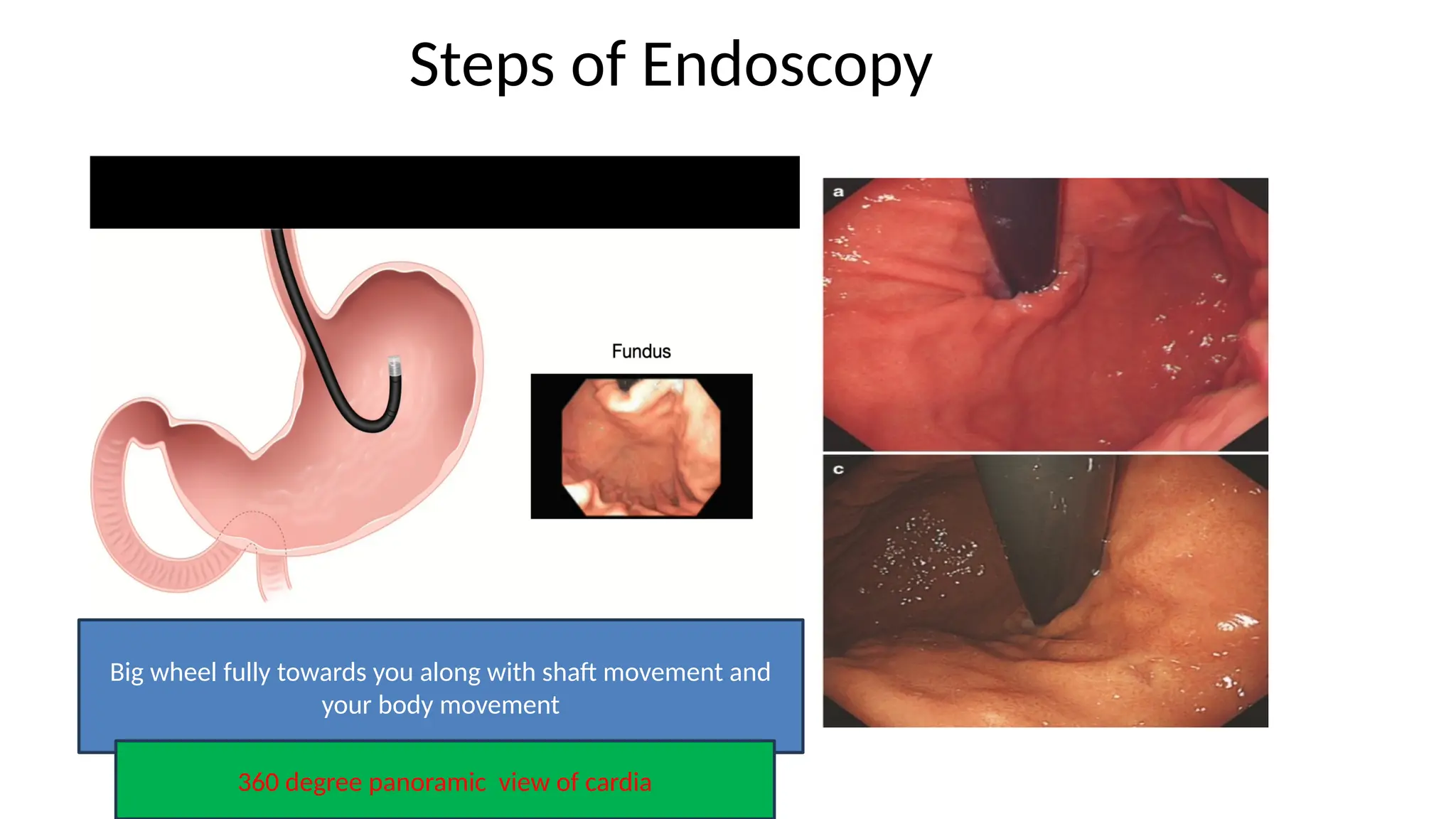
Steps of Endoscopy
Bigwheel fully towards you along with shaft movement and
your body movement
360 degree panoramic view of cardia
27.
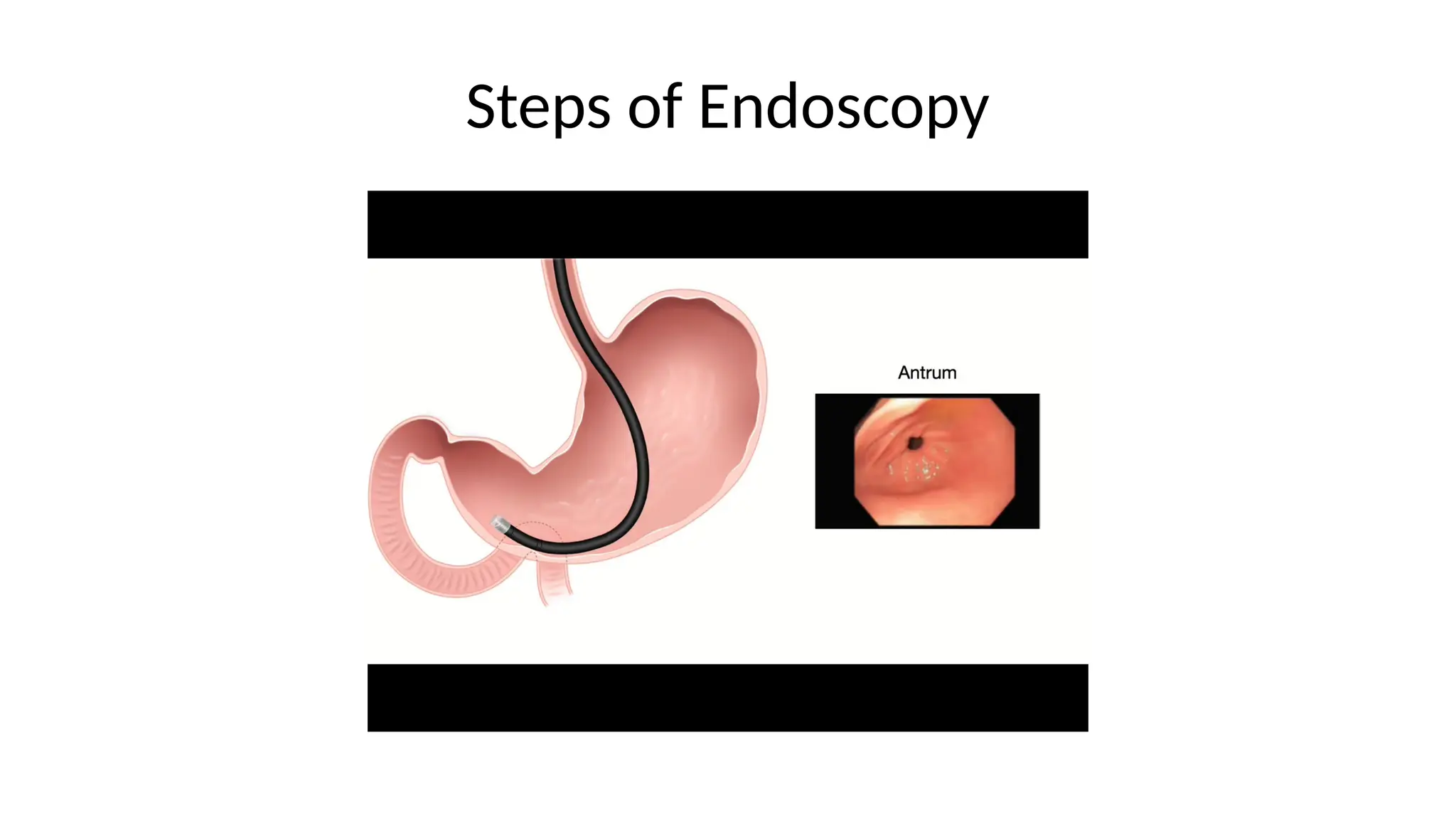
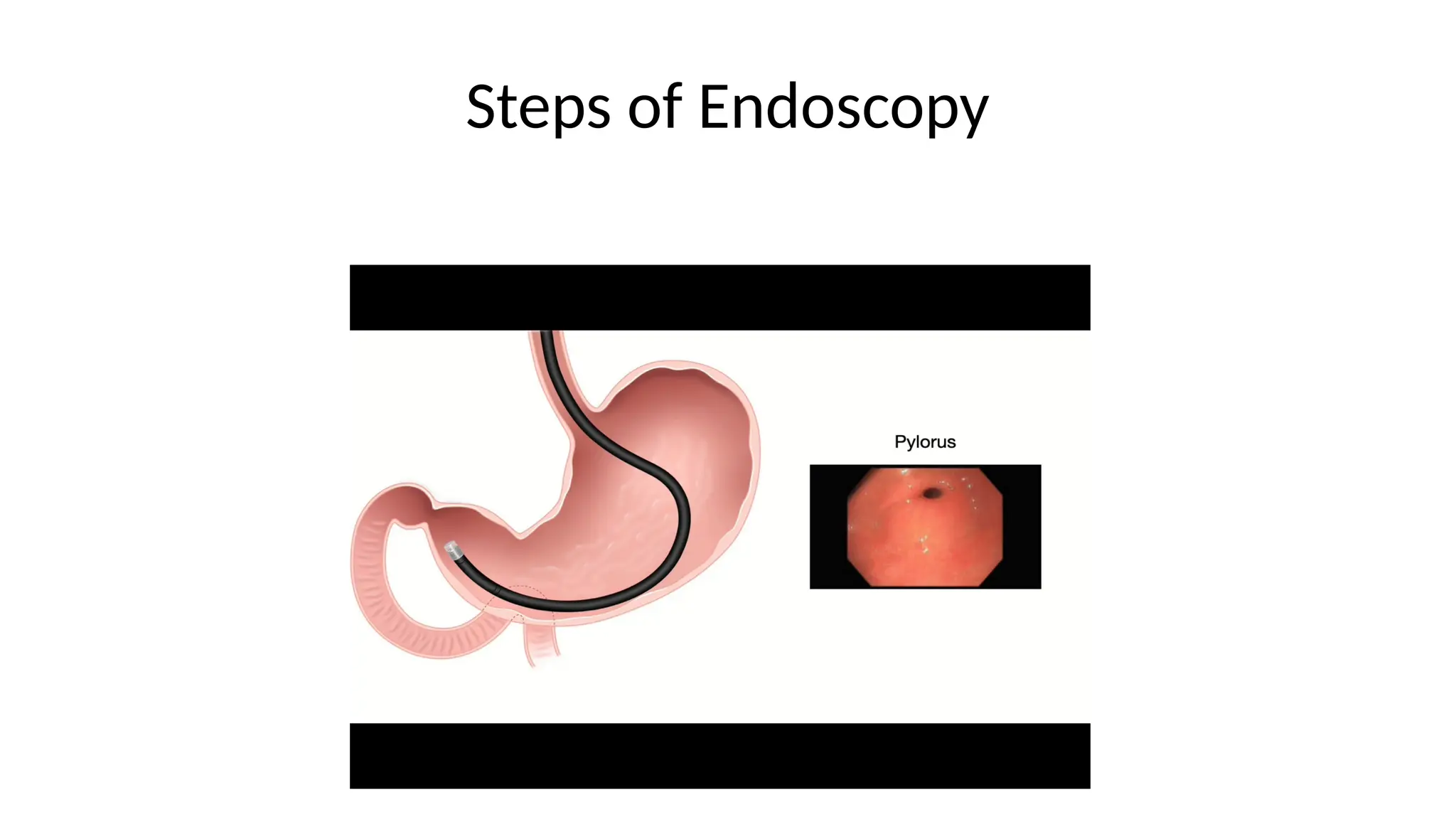
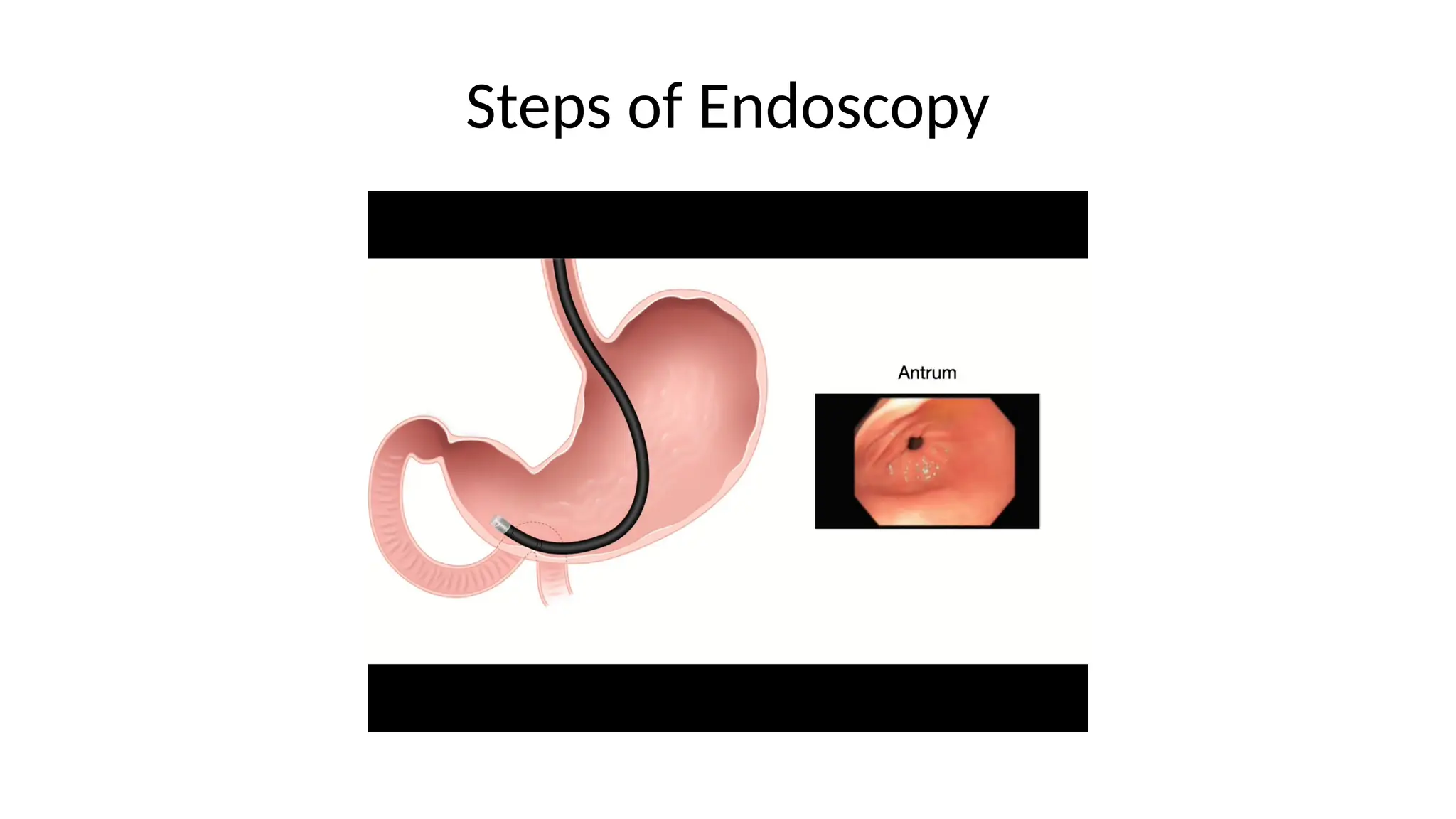
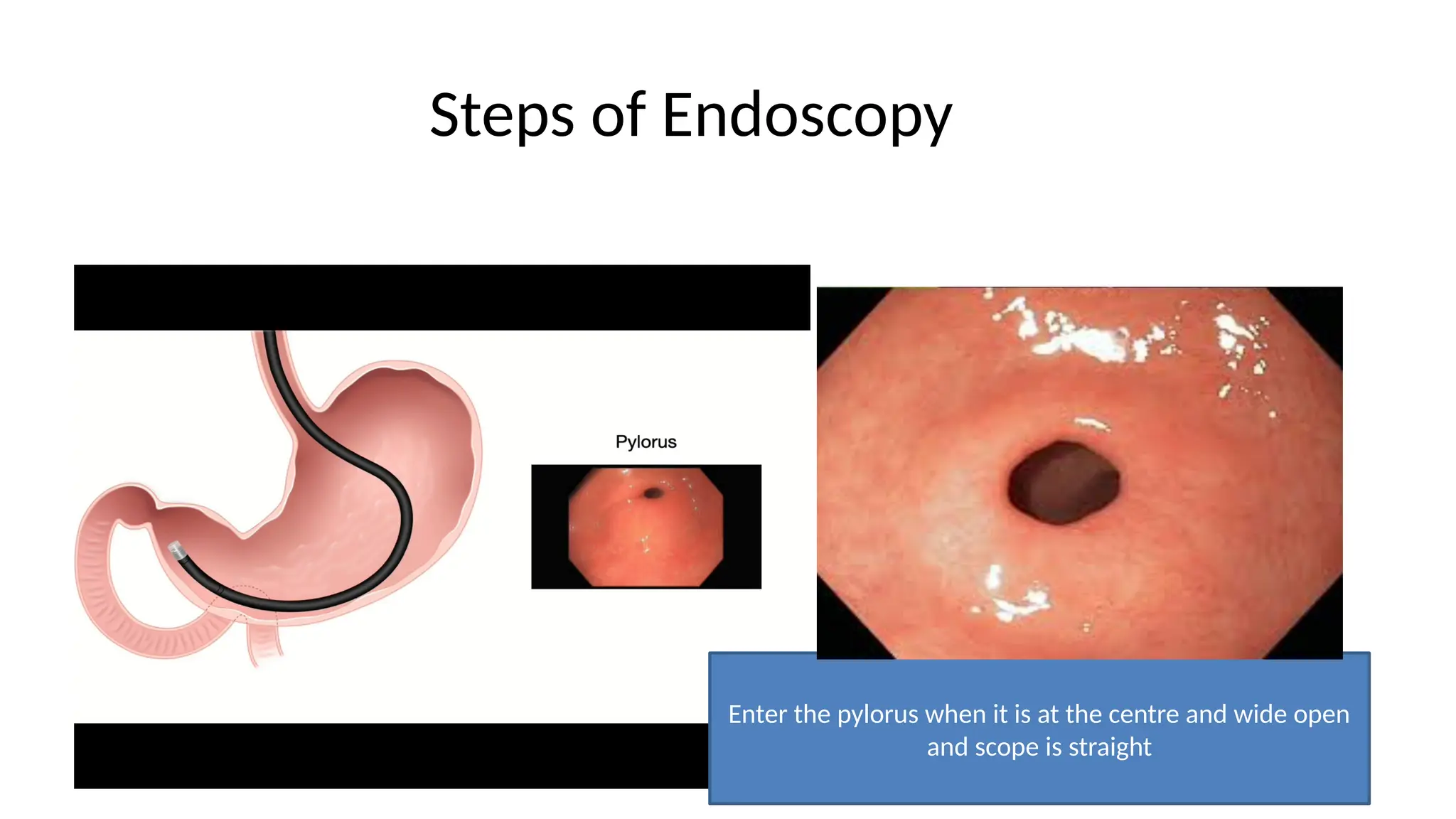
Steps of Endoscopy
Enterthe pylorus when it is at the centre and wide open
and scope is straight
28.
Steps of Endoscopy
Enter2nd
part: Do 3 maneuvers
Big wheel: towards U
Small wheel: away from U
Turn your body to right
29.
Removing the instrument
Mucosalviews are often optimal during instrument withdrawal
The proximal lesser curve, a potential “blind spot” merits
particular attention
Aspirate air from the stomach completely on withdrawal
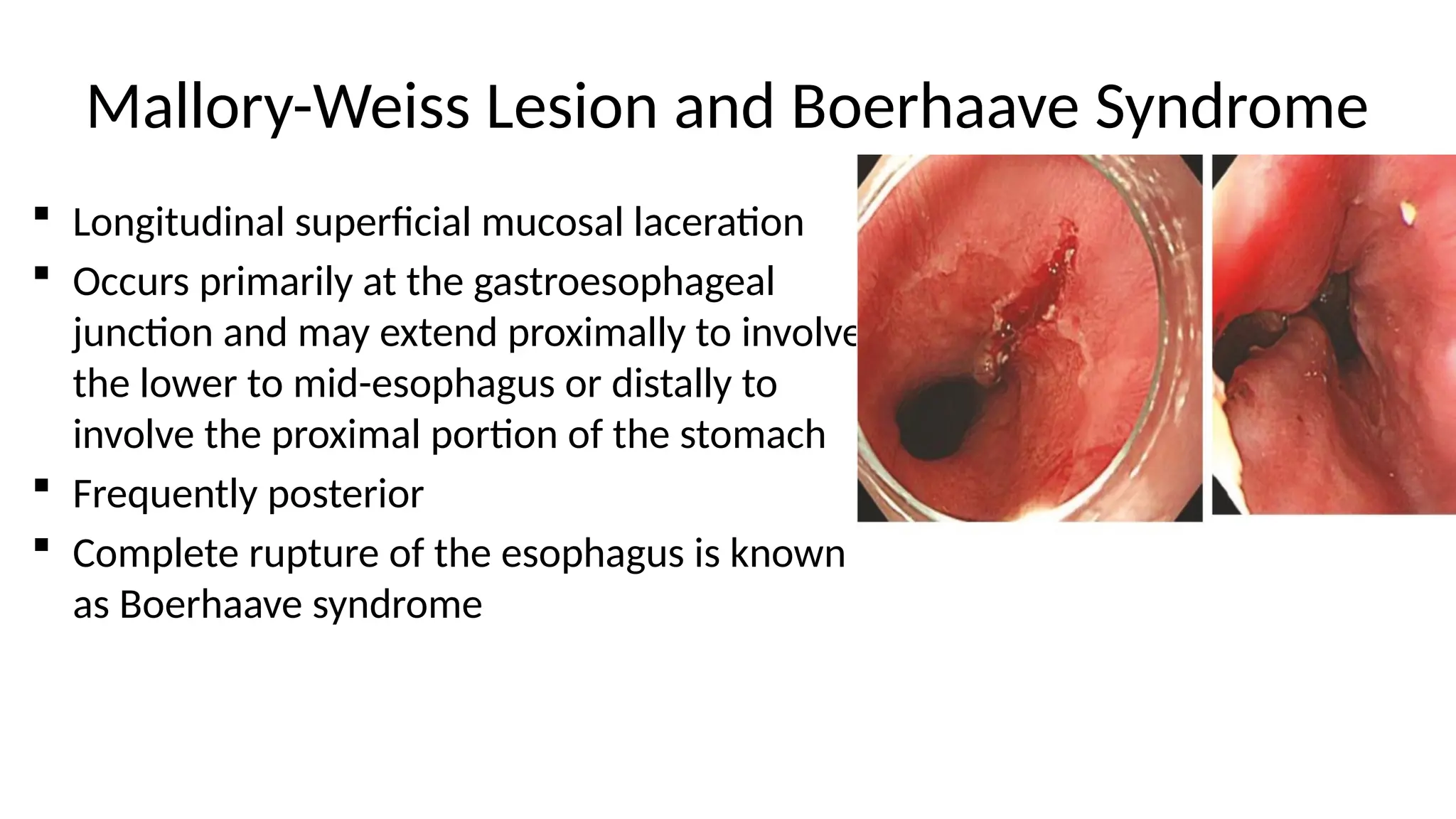
Mallory-Weiss Lesion andBoerhaave Syndrome
Longitudinal superficial mucosal laceration
Occurs primarily at the gastroesophageal
junction and may extend proximally to involve
the lower to mid-esophagus or distally to
involve the proximal portion of the stomach
Frequently posterior
Complete rupture of the esophagus is known
as Boerhaave syndrome
32.
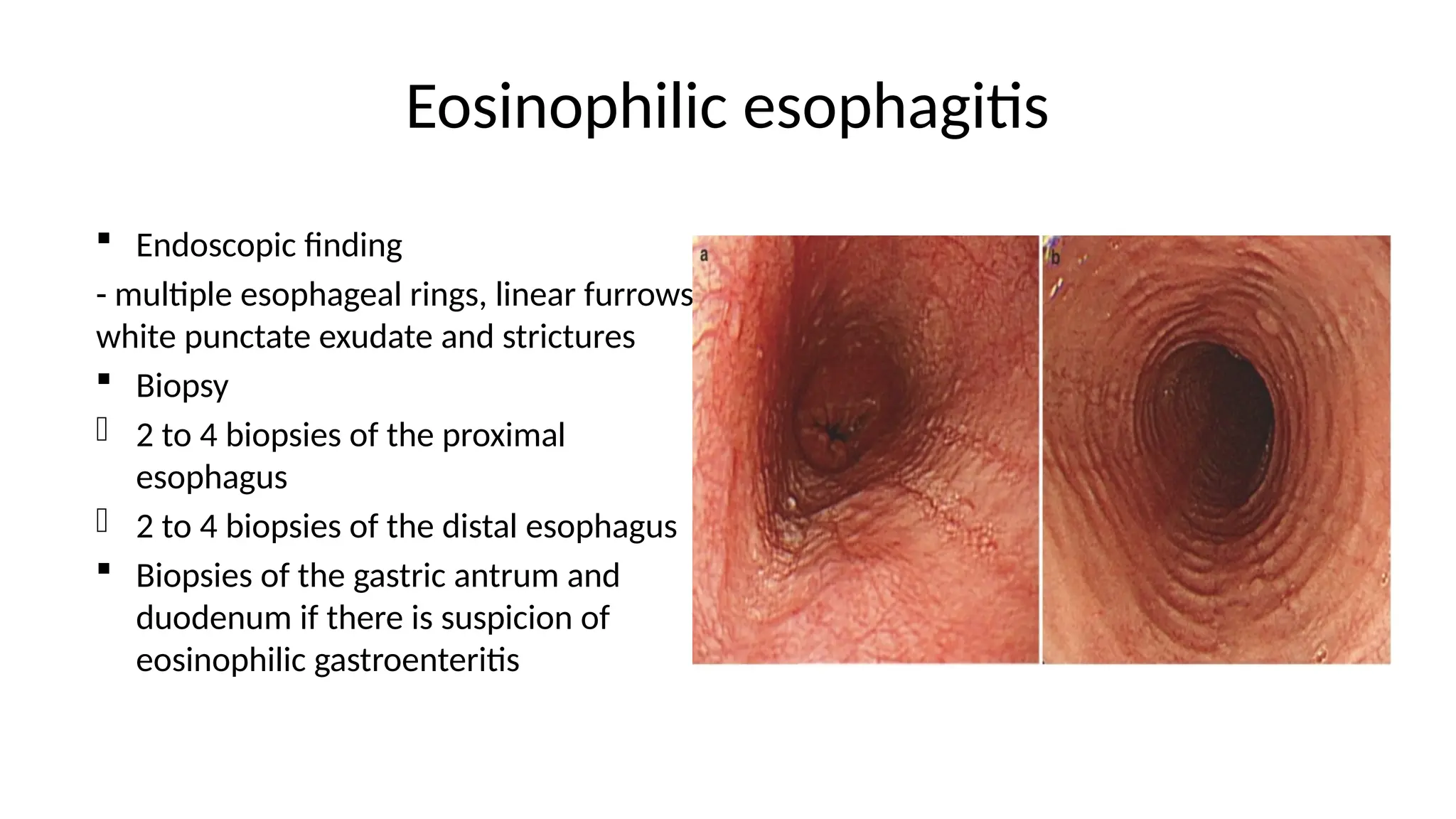
Eosinophilic esophagitis
Endoscopicfinding
- multiple esophageal rings, linear furrows,
white punctate exudate and strictures
Biopsy
- 2 to 4 biopsies of the proximal
esophagus
- 2 to 4 biopsies of the distal esophagus
Biopsies of the gastric antrum and
duodenum if there is suspicion of
eosinophilic gastroenteritis
33.
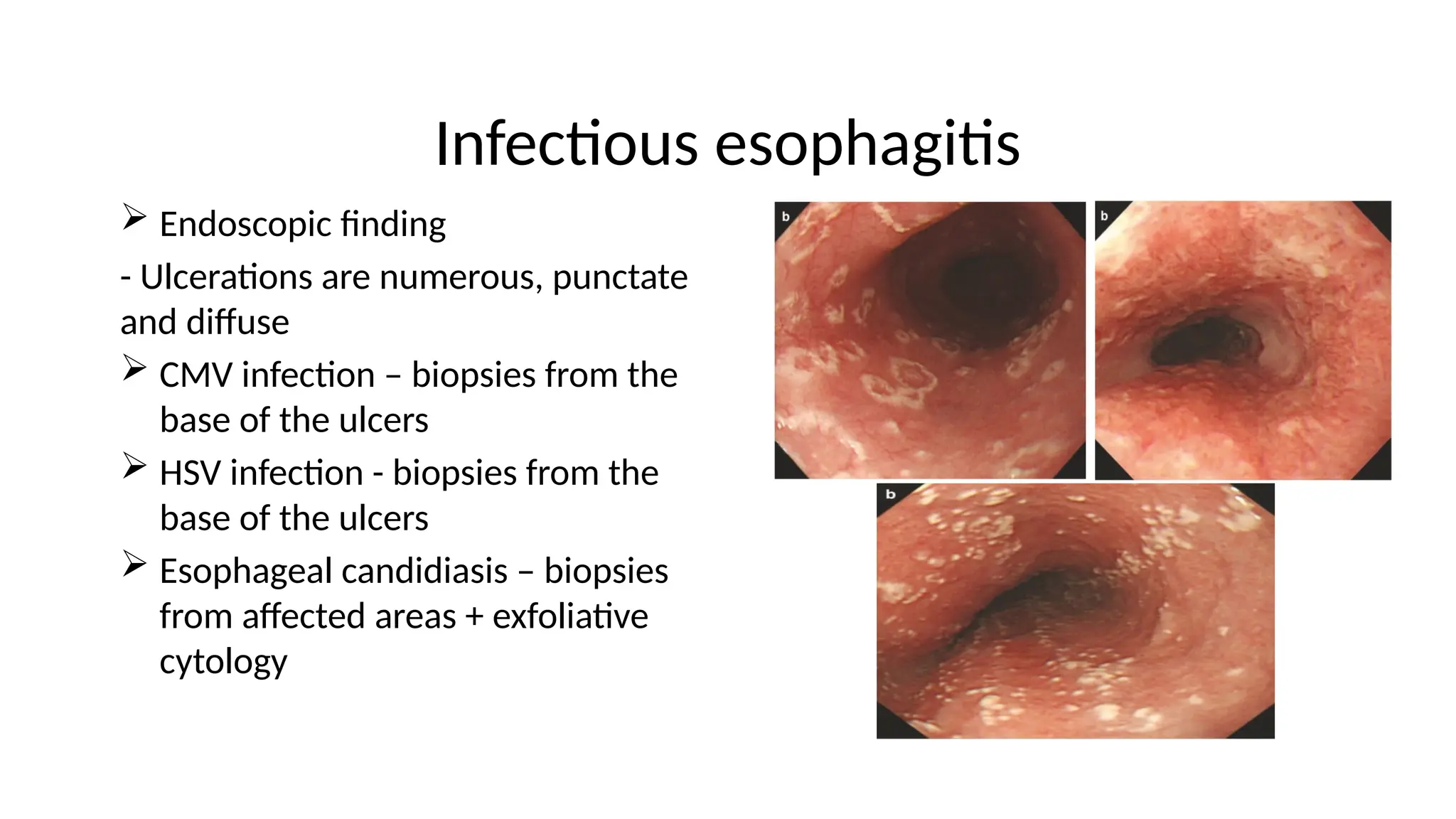
Infectious esophagitis
Endoscopicfinding
- Ulcerations are numerous, punctate
and diffuse
CMV infection – biopsies from the
base of the ulcers
HSV infection - biopsies from the
base of the ulcers
Esophageal candidiasis – biopsies
from affected areas + exfoliative
cytology
34.
Gastroesophageal Reflux andReflux Esophagitis
Endoscopic findings
Erosions and ulcerations are usually few and distal
Indications for endoscopy
For patients with GERD symptoms who also have alarm symptoms such as
• Dysphagia
• Weight loss
• Bleeding
• Vomiting
• Anemia
Diagnostic endoscopy should ideally be performed after PPIs have been
stopped for 2 weeks and perhaps as long as 4 weeks if possible
35.
Gastroesophageal Reflux andReflux Esophagitis
Esophageal biopsy should be taken to exclude other diagnosis, including
infectious etiologies and malignancy under the following condition
Immunocompromised patients
Irregular and deep ulceration
Presence of mass lesion or nodularity
Irregular or malignant appearing stricture
Biopsy
Targeted biopsies of irregular mucosa
36.
Modified Los AngelesClassification of GERD
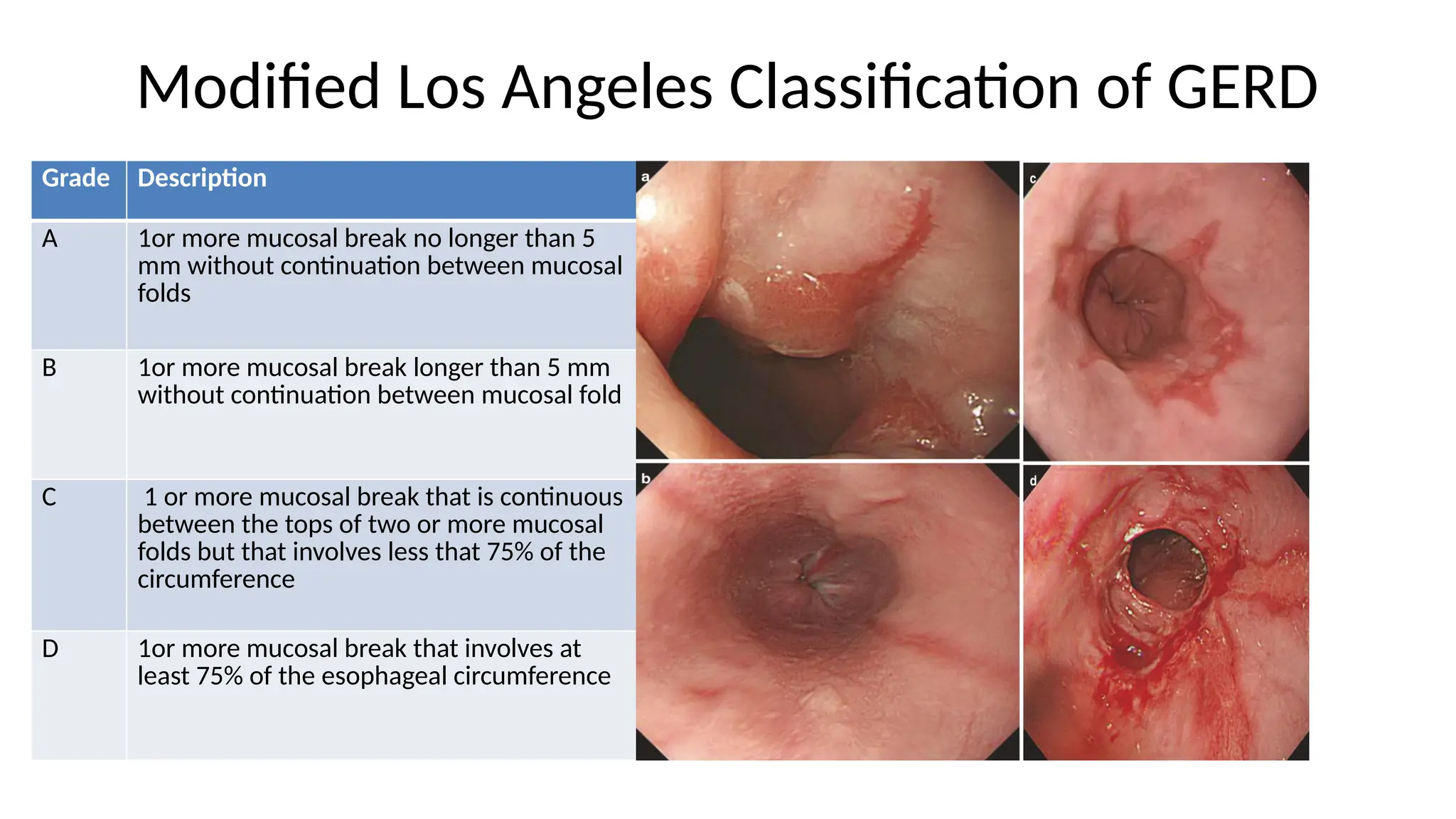
Grade Description
A 1or more mucosal break no longer than 5
mm without continuation between mucosal
folds
B 1or more mucosal break longer than 5 mm
without continuation between mucosal fold
C 1 or more mucosal break that is continuous
between the tops of two or more mucosal
folds but that involves less that 75% of the
circumference
D 1or more mucosal break that involves at
least 75% of the esophageal circumference
37.
Hiatial Hernia
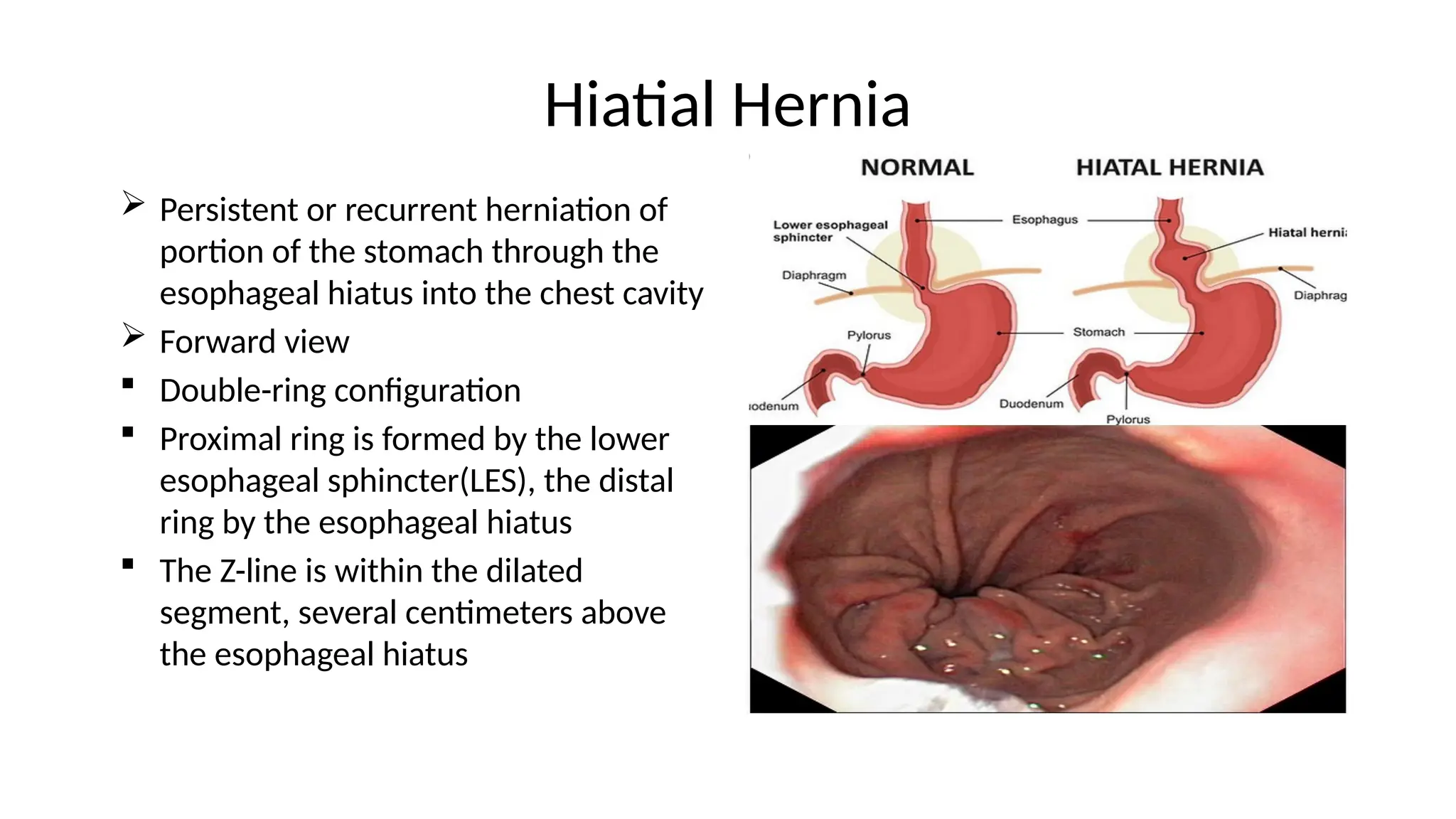
Persistentor recurrent herniation of
portion of the stomach through the
esophageal hiatus into the chest cavity
Forward view
Double-ring configuration
Proximal ring is formed by the lower
esophageal sphincter(LES), the distal
ring by the esophageal hiatus
The Z-line is within the dilated
segment, several centimeters above
the esophageal hiatus
38.
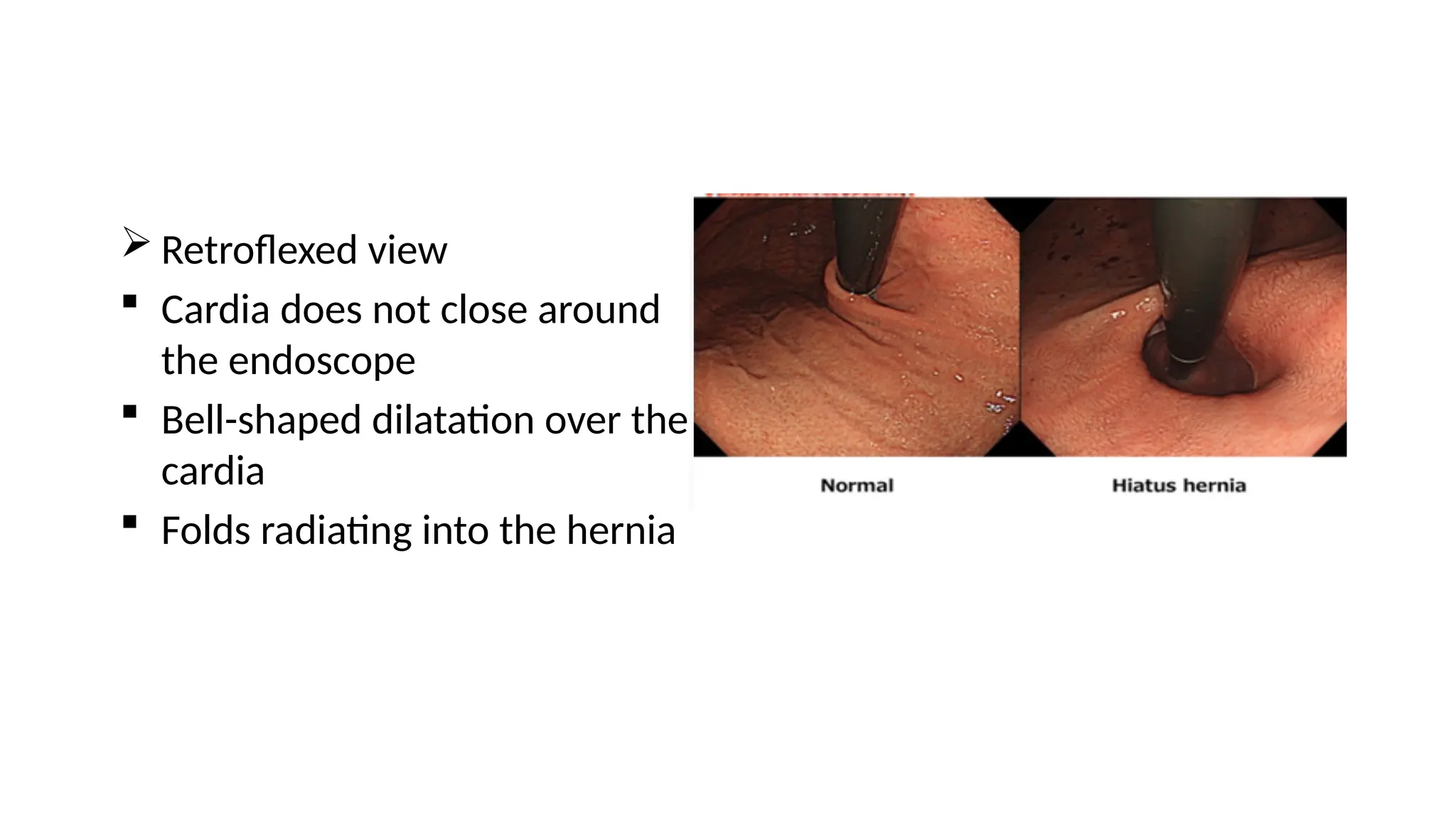
Retroflexed view
Cardia does not close around
the endoscope
Bell-shaped dilatation over the
cardia
Folds radiating into the hernia
39.
Barrett’s Esophagus
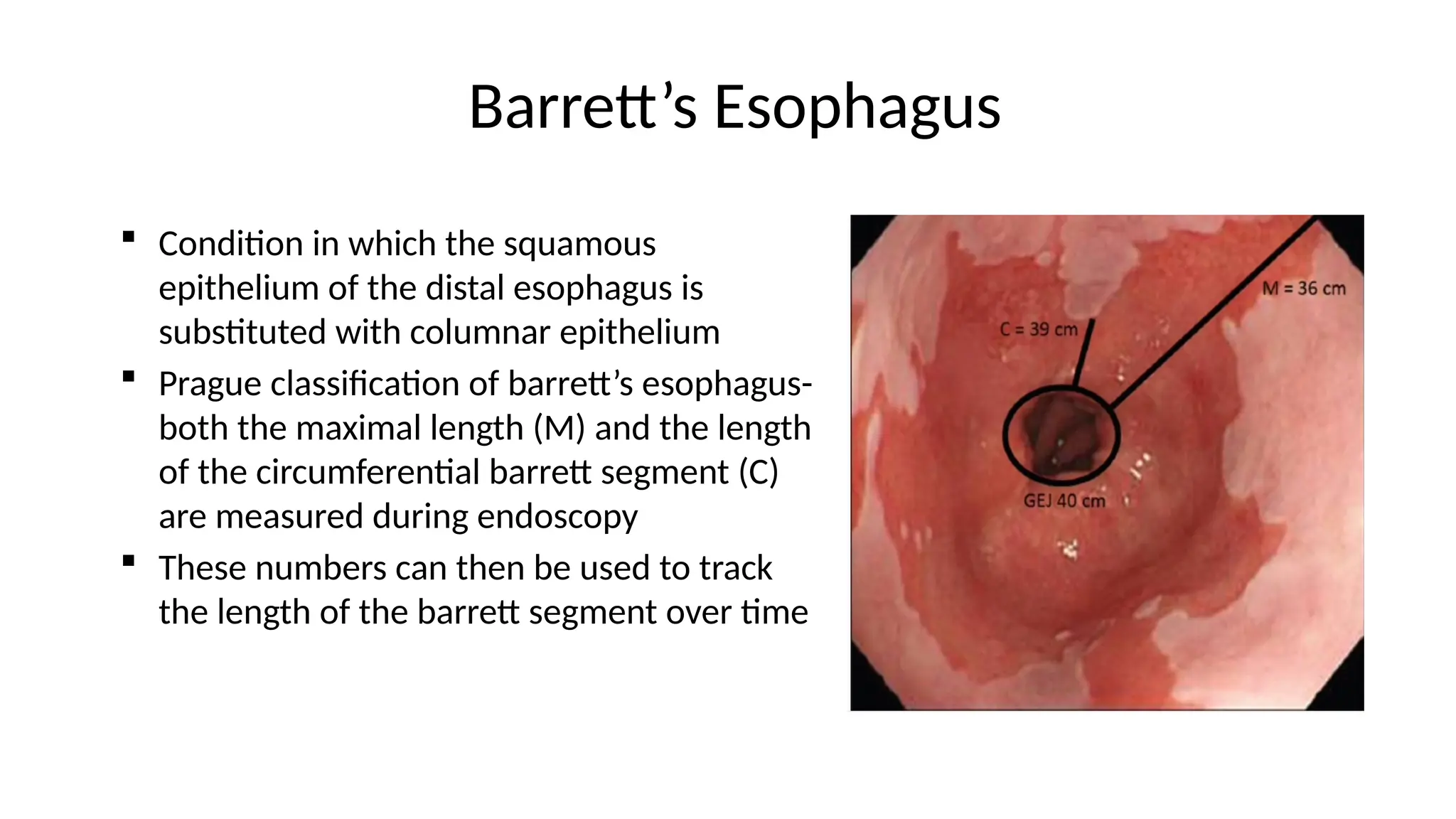
Conditionin which the squamous
epithelium of the distal esophagus is
substituted with columnar epithelium
Prague classification of barrett’s esophagus-
both the maximal length (M) and the length
of the circumferential barrett segment (C)
are measured during endoscopy
These numbers can then be used to track
the length of the barrett segment over time
40.
Barrett’s Esophagus
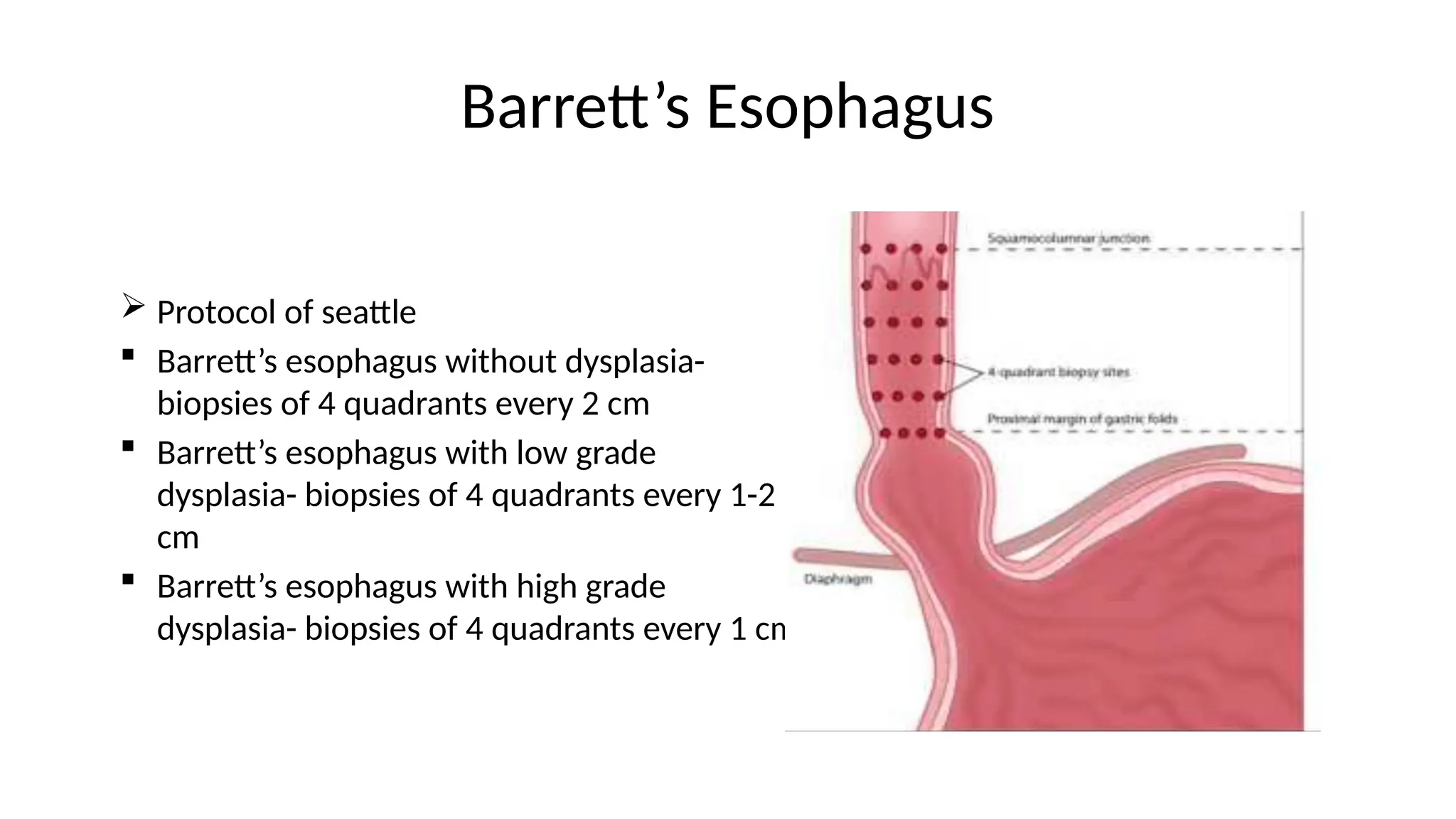
Protocolof seattle
Barrett’s esophagus without dysplasia-
biopsies of 4 quadrants every 2 cm
Barrett’s esophagus with low grade
dysplasia- biopsies of 4 quadrants every 1-2
cm
Barrett’s esophagus with high grade
dysplasia- biopsies of 4 quadrants every 1 cm
41.
Esophageal Varices
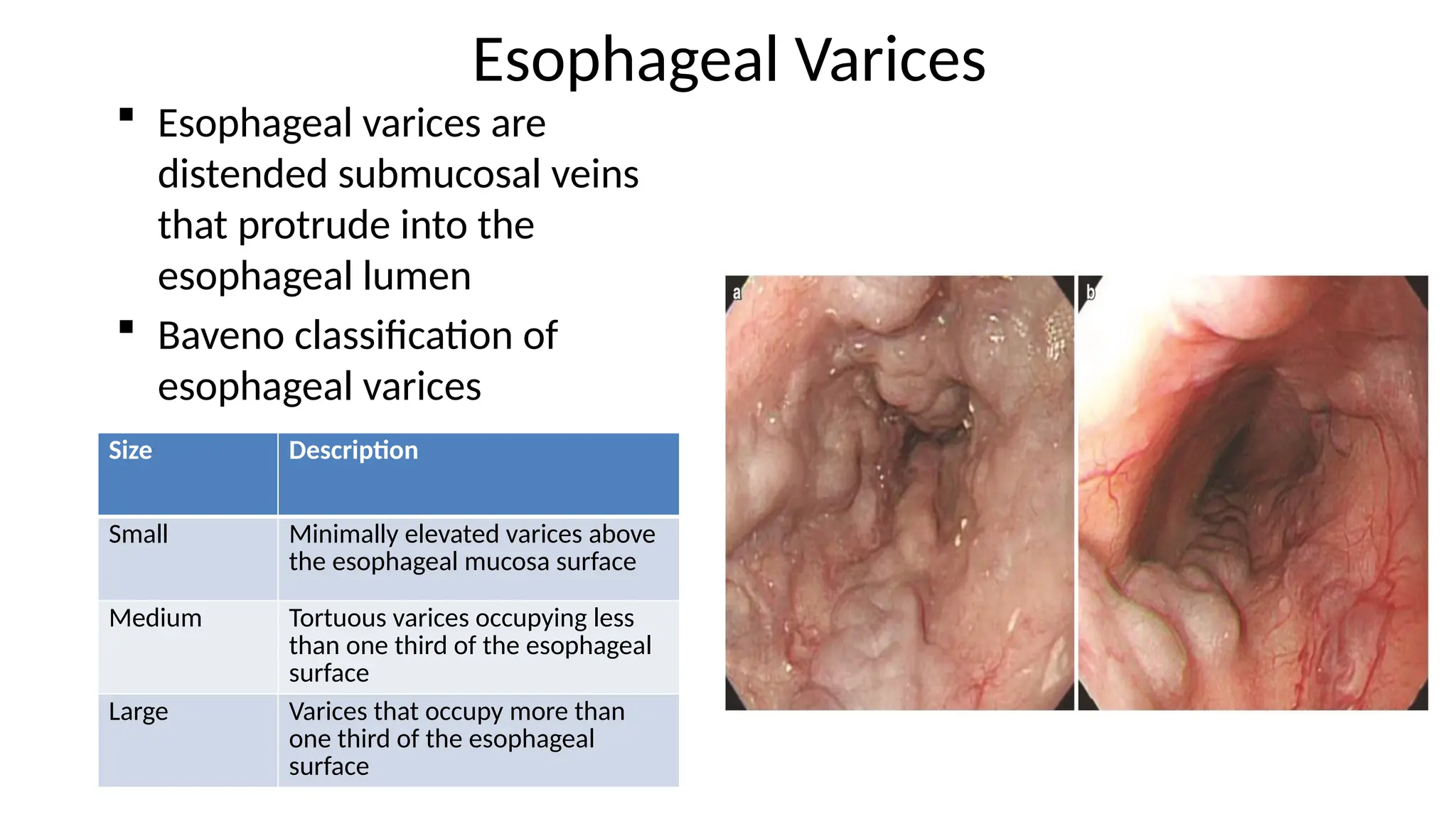
Esophagealvarices are
distended submucosal veins
that protrude into the
esophageal lumen
Baveno classification of
esophageal varices
Size Description
Small Minimally elevated varices above
the esophageal mucosa surface
Medium Tortuous varices occupying less
than one third of the esophageal
surface
Large Varices that occupy more than
one third of the esophageal
surface
42.
Esophageal Varices
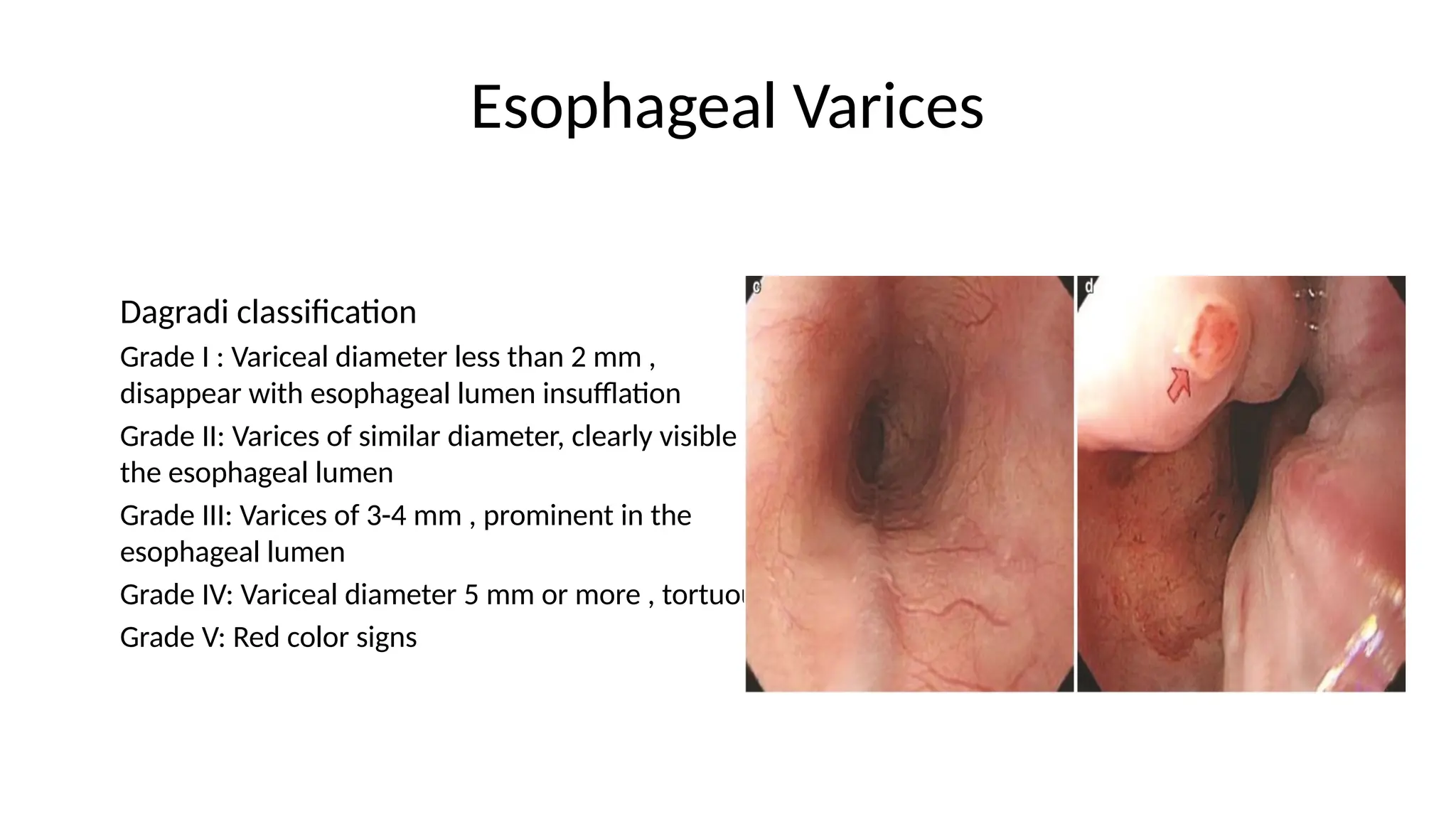
Dagradi classification
GradeI : Variceal diameter less than 2 mm ,
disappear with esophageal lumen insufflation
Grade II: Varices of similar diameter, clearly visible in
the esophageal lumen
Grade III: Varices of 3-4 mm , prominent in the
esophageal lumen
Grade IV: Variceal diameter 5 mm or more , tortuous
Grade V: Red color signs
43.
Gastritis
Endoscopic features:
-Edema
- Exudate
- Erythema
- Erosion
- Hemorrhage
Type A (Autoimmune gastritis)- Body
predominant
Type B ( Bacterial gastritis)- Antral
predominant
44.
Urease test
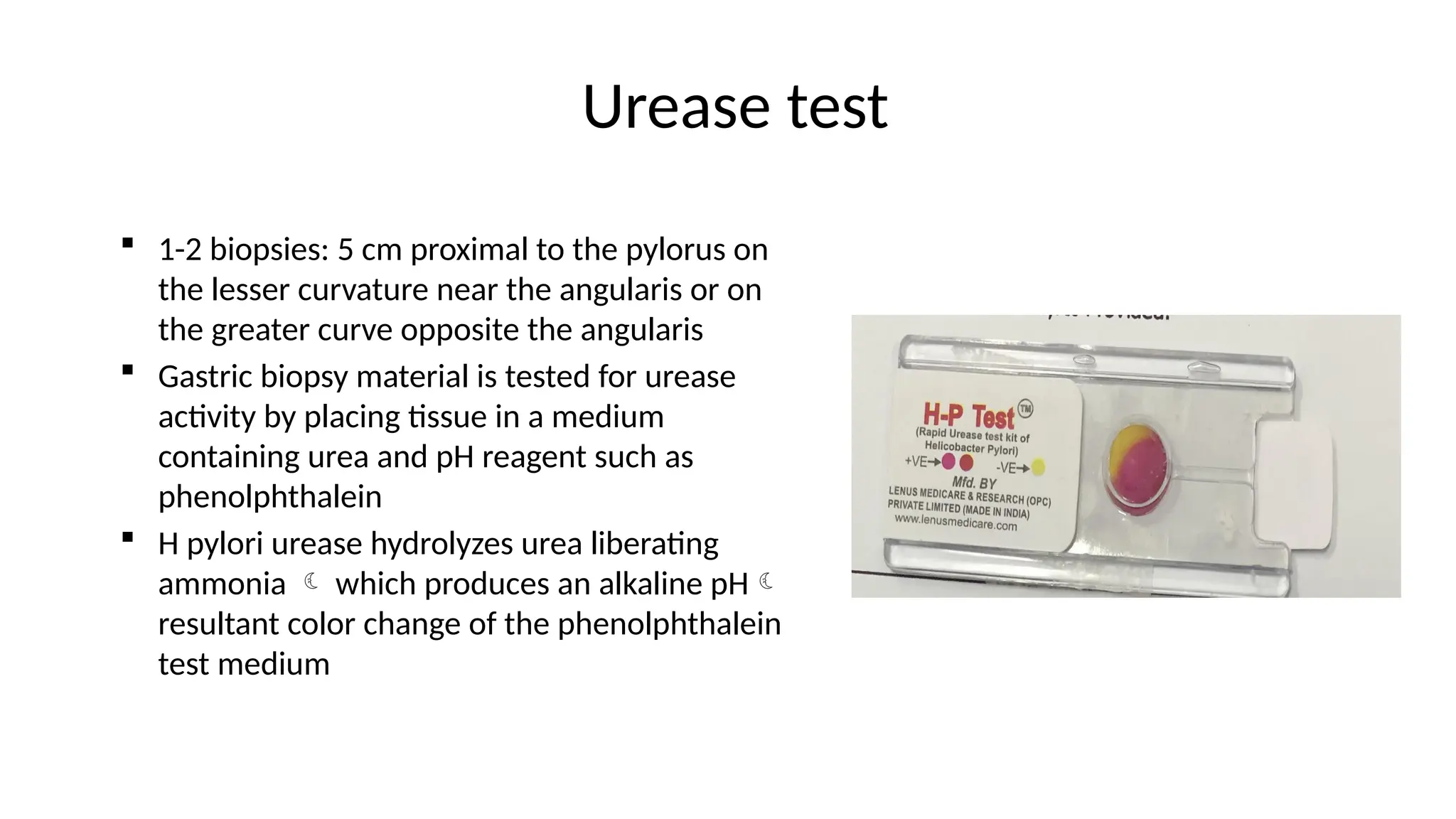
1-2biopsies: 5 cm proximal to the pylorus on
the lesser curvature near the angularis or on
the greater curve opposite the angularis
Gastric biopsy material is tested for urease
activity by placing tissue in a medium
containing urea and pH reagent such as
phenolphthalein
H pylori urease hydrolyzes urea liberating
ammonia which produces an alkaline pH
resultant color change of the phenolphthalein
test medium
45.
Urease test
Sensitivityand specificity of tests are 90% to 95% and 95% to 100%
Accuracy can be negatively affected by the blood in the stomach or
by the use of antibiotics, bismuth-containing compounds or acid
antisecretory drugs, especially PPIs.
Negative urease test does not exclude Hp infection in an individual
taking antisecretory medication
To improve sensitivity, stopping the potentially problematic
medication and delaying endoscopy for 2 weeks if possible
H. pylori eradication should be documented 4 weeks after
completing antibiotics and atleast 7 days off antisecretory agents
46.
Potential indication forgastroscopic biopsies
Gastric erosions or ulcer
Thick gastric folds
Gastric polyp or mass
For diagnosis of Hp infection
47.
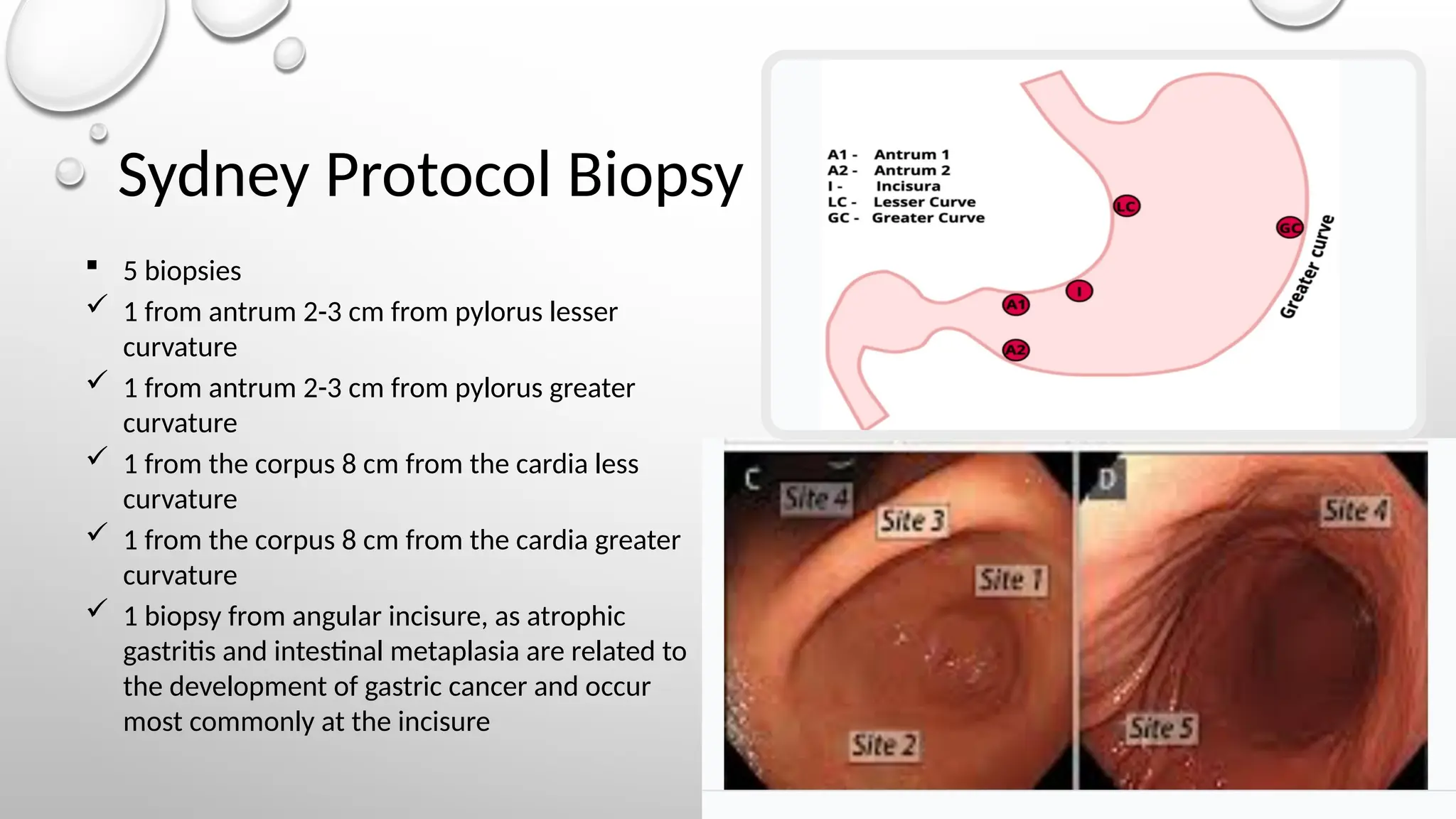
Sydney Protocol Biopsy
5 biopsies
1 from antrum 2-3 cm from pylorus lesser
curvature
1 from antrum 2-3 cm from pylorus greater
curvature
1 from the corpus 8 cm from the cardia less
curvature
1 from the corpus 8 cm from the cardia greater
curvature
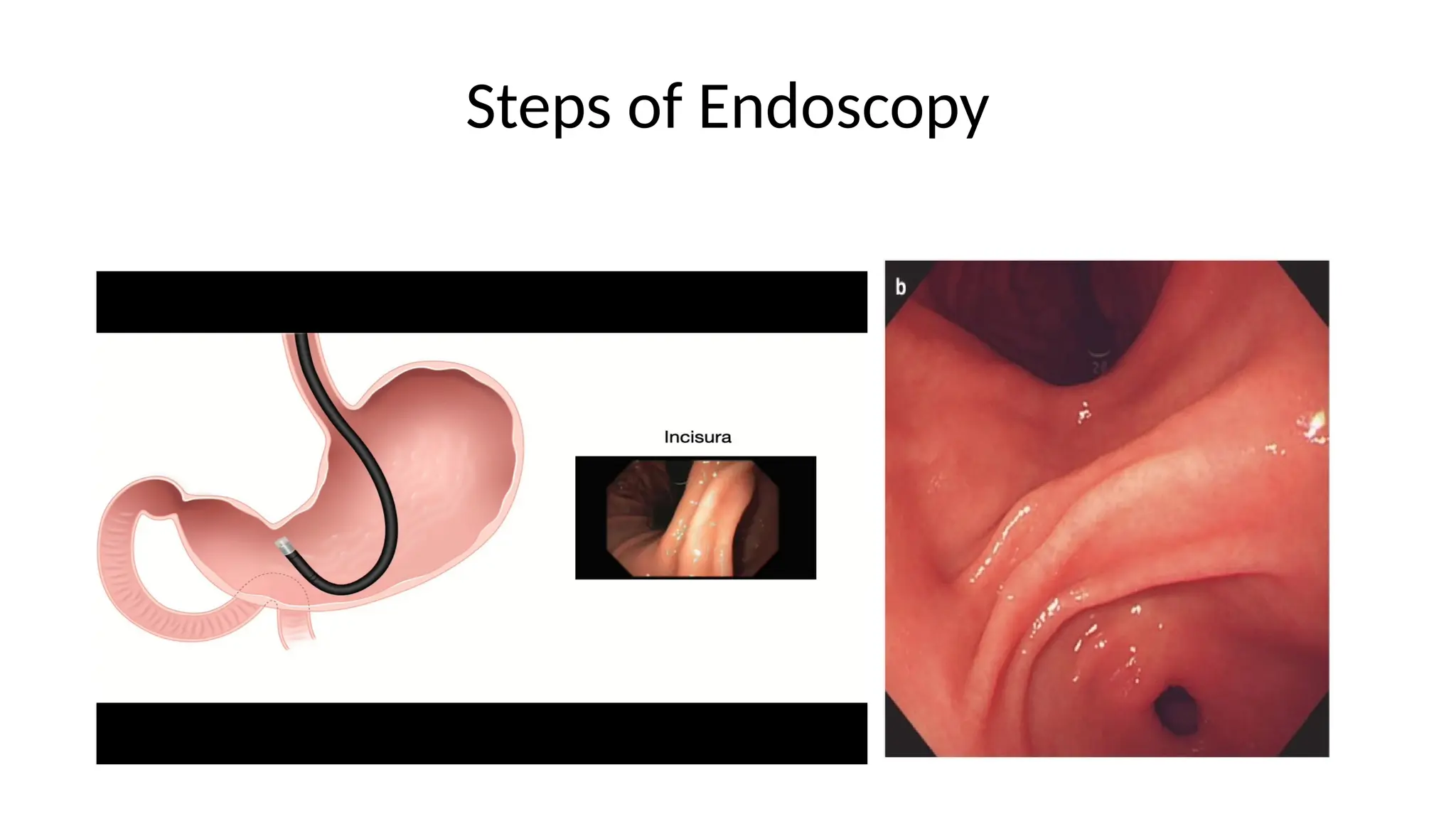
1 biopsy from angular incisure, as atrophic
gastritis and intestinal metaplasia are related to
the development of gastric cancer and occur
most commonly at the incisure
48.
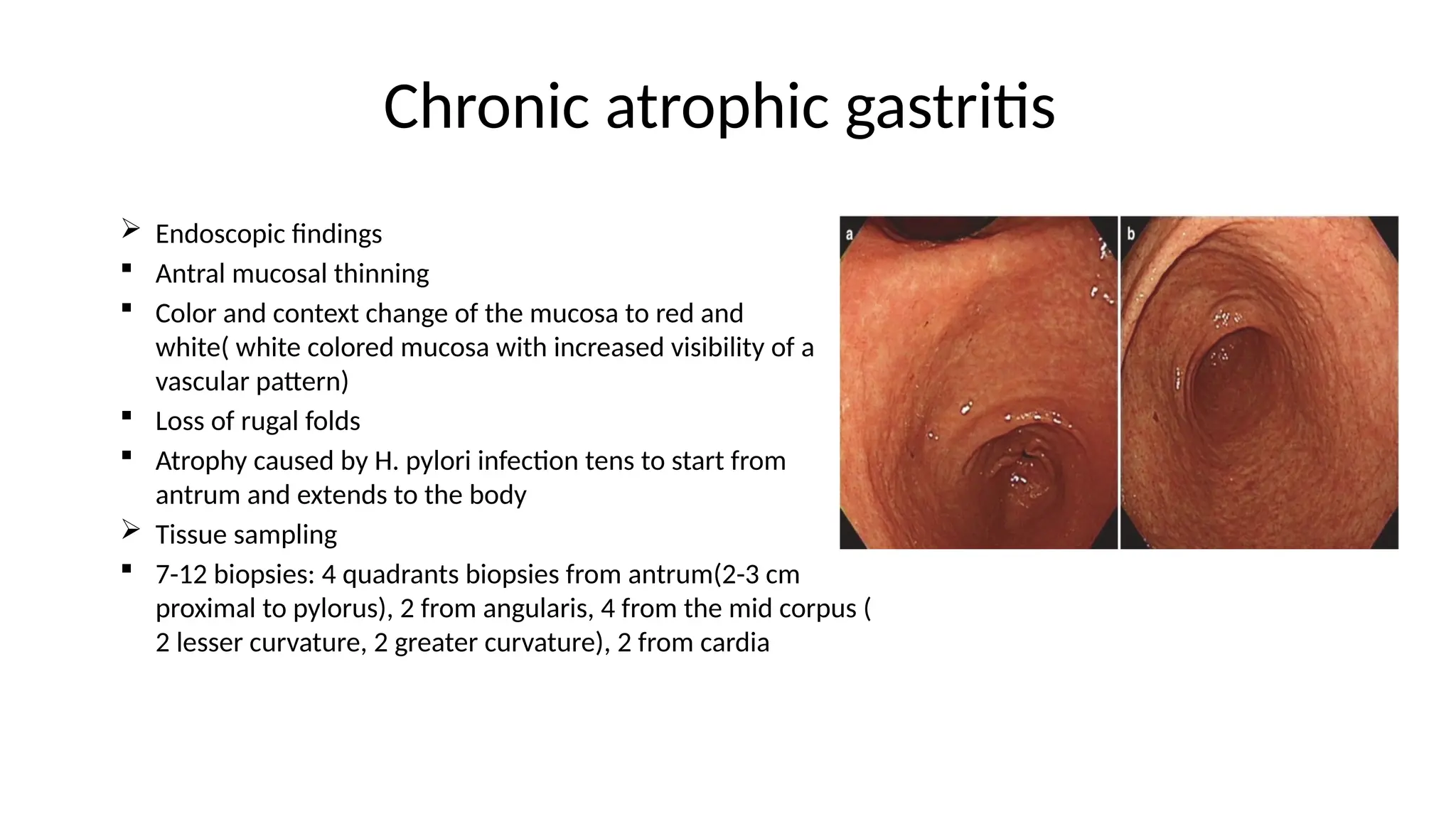
Chronic atrophic gastritis
Endoscopic findings
Antral mucosal thinning
Color and context change of the mucosa to red and
white( white colored mucosa with increased visibility of a
vascular pattern)
Loss of rugal folds
Atrophy caused by H. pylori infection tens to start from
antrum and extends to the body
Tissue sampling
7-12 biopsies: 4 quadrants biopsies from antrum(2-3 cm
proximal to pylorus), 2 from angularis, 4 from the mid corpus (
2 lesser curvature, 2 greater curvature), 2 from cardia
49.
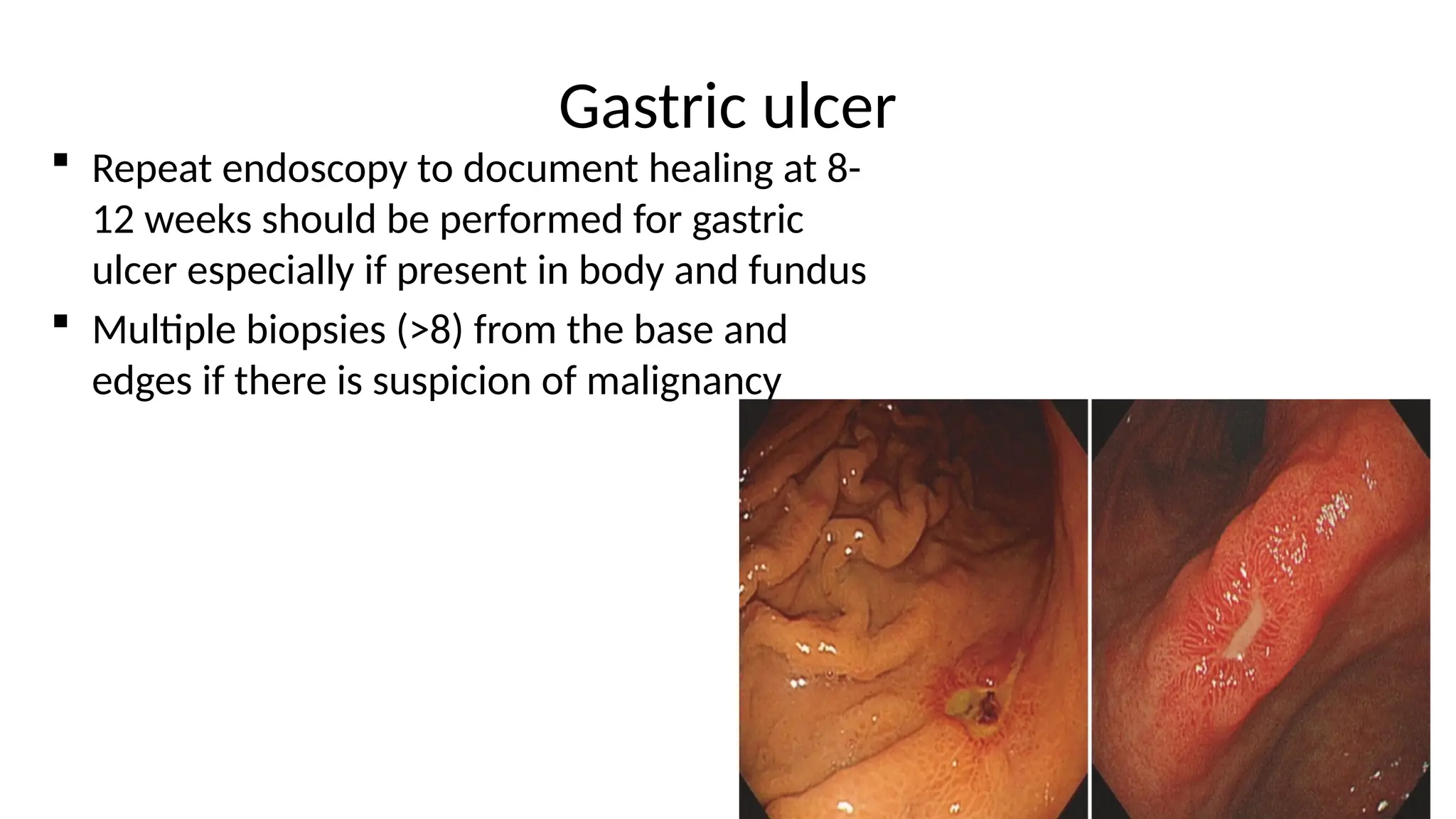
Gastric ulcer
Repeatendoscopy to document healing at 8-
12 weeks should be performed for gastric
ulcer especially if present in body and fundus
Multiple biopsies (>8) from the base and
edges if there is suspicion of malignancy
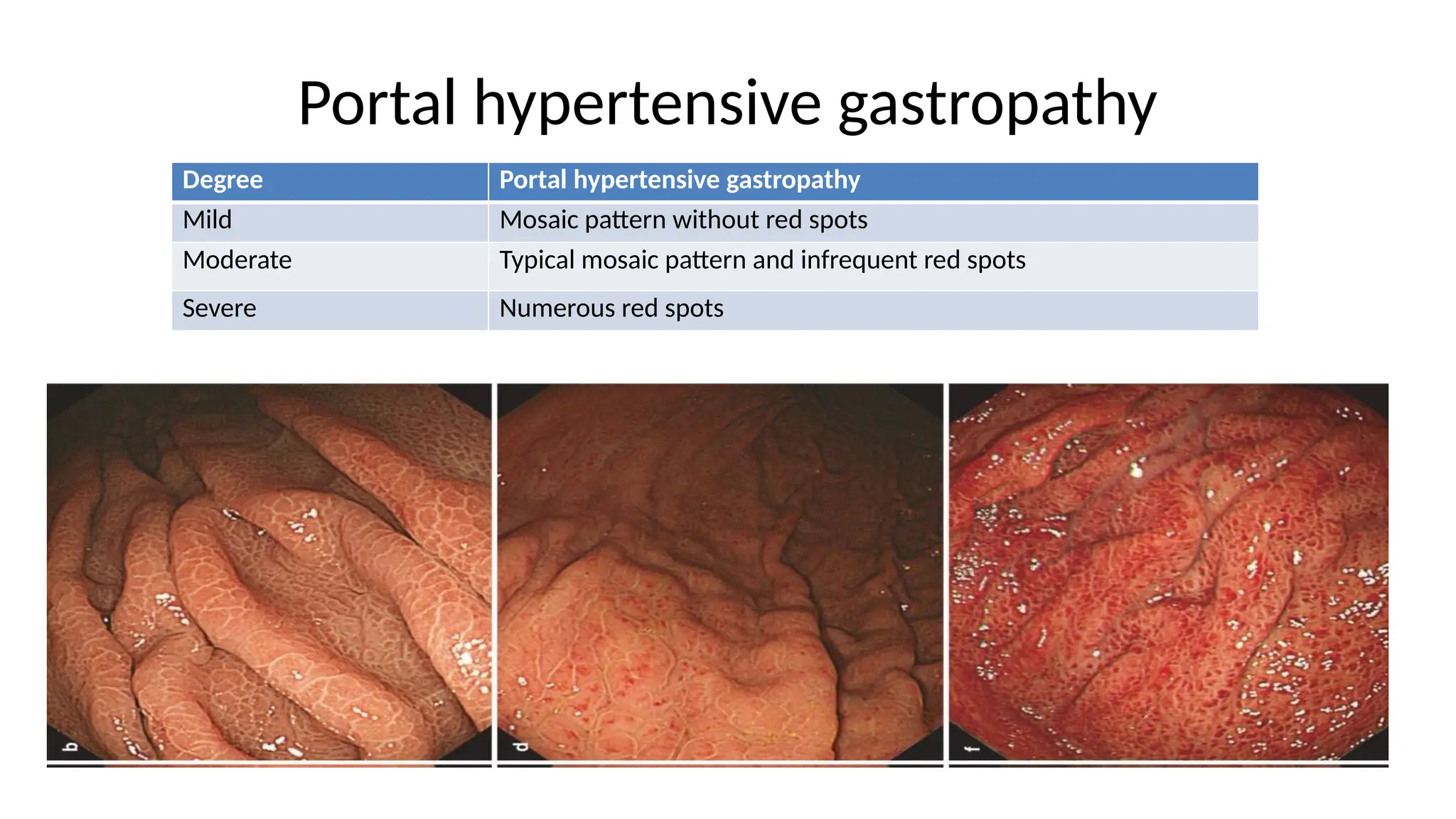
Portal hypertensive gastropathy
DegreePortal hypertensive gastropathy
Mild Mosaic pattern without red spots
Moderate Typical mosaic pattern and infrequent red spots
Severe Numerous red spots
52.
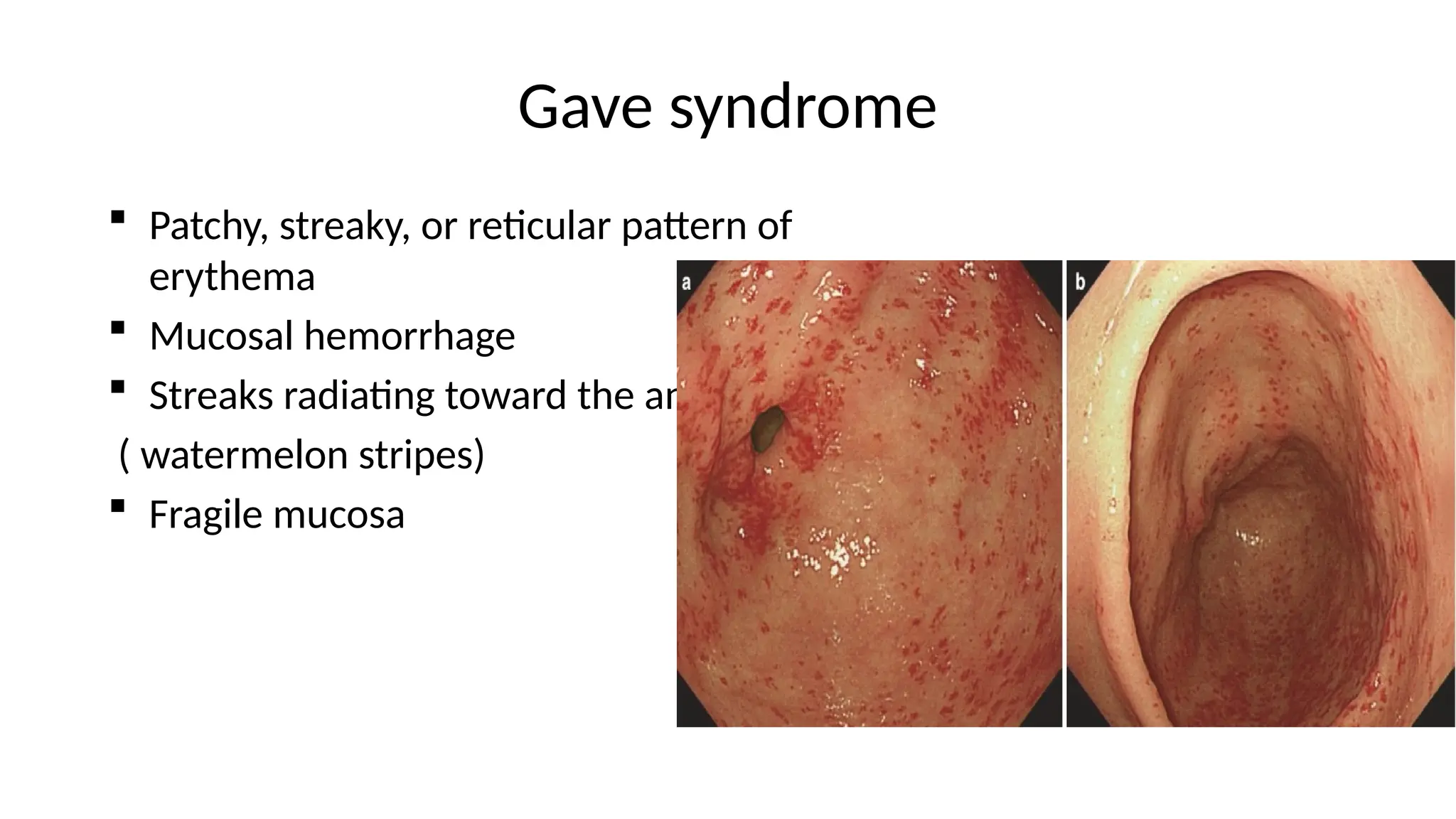
Gave syndrome
Patchy,streaky, or reticular pattern of
erythema
Mucosal hemorrhage
Streaks radiating toward the antrum
( watermelon stripes)
Fragile mucosa
53.
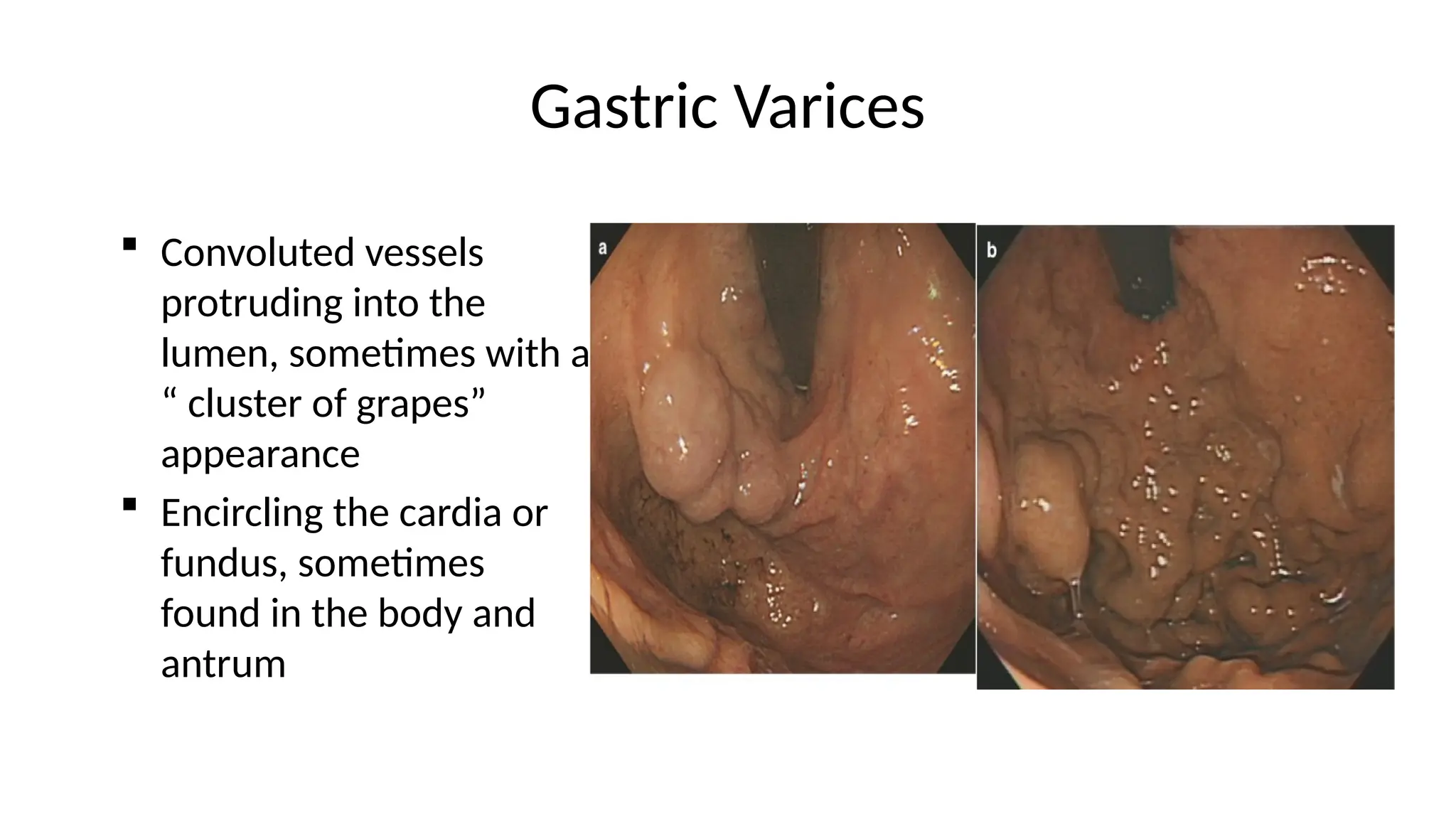
Gastric Varices
Convolutedvessels
protruding into the
lumen, sometimes with a
“ cluster of grapes”
appearance
Encircling the cardia or
fundus, sometimes
found in the body and
antrum
54.
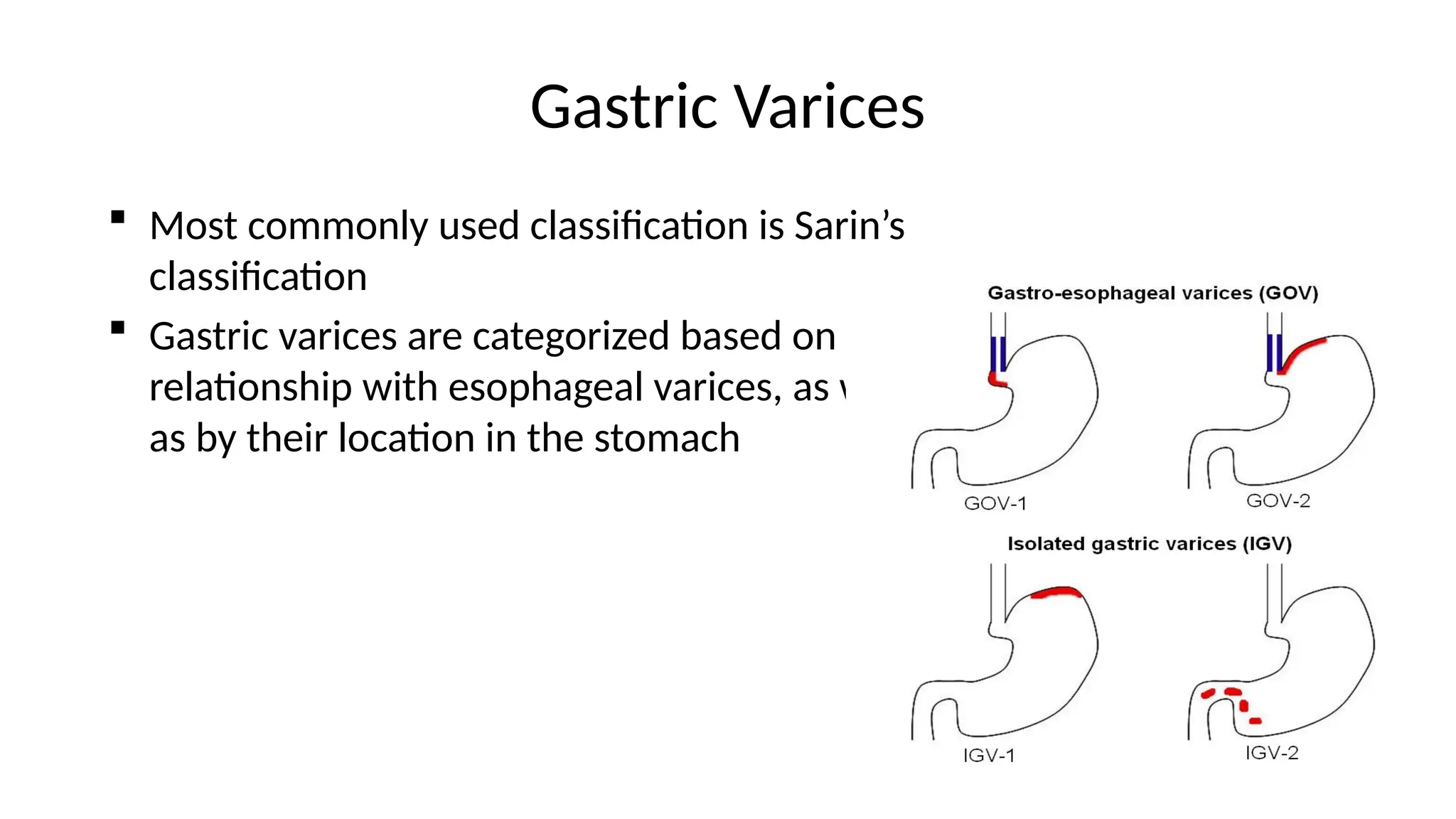
Gastric Varices
Mostcommonly used classification is Sarin’s
classification
Gastric varices are categorized based on the
relationship with esophageal varices, as well
as by their location in the stomach
55.
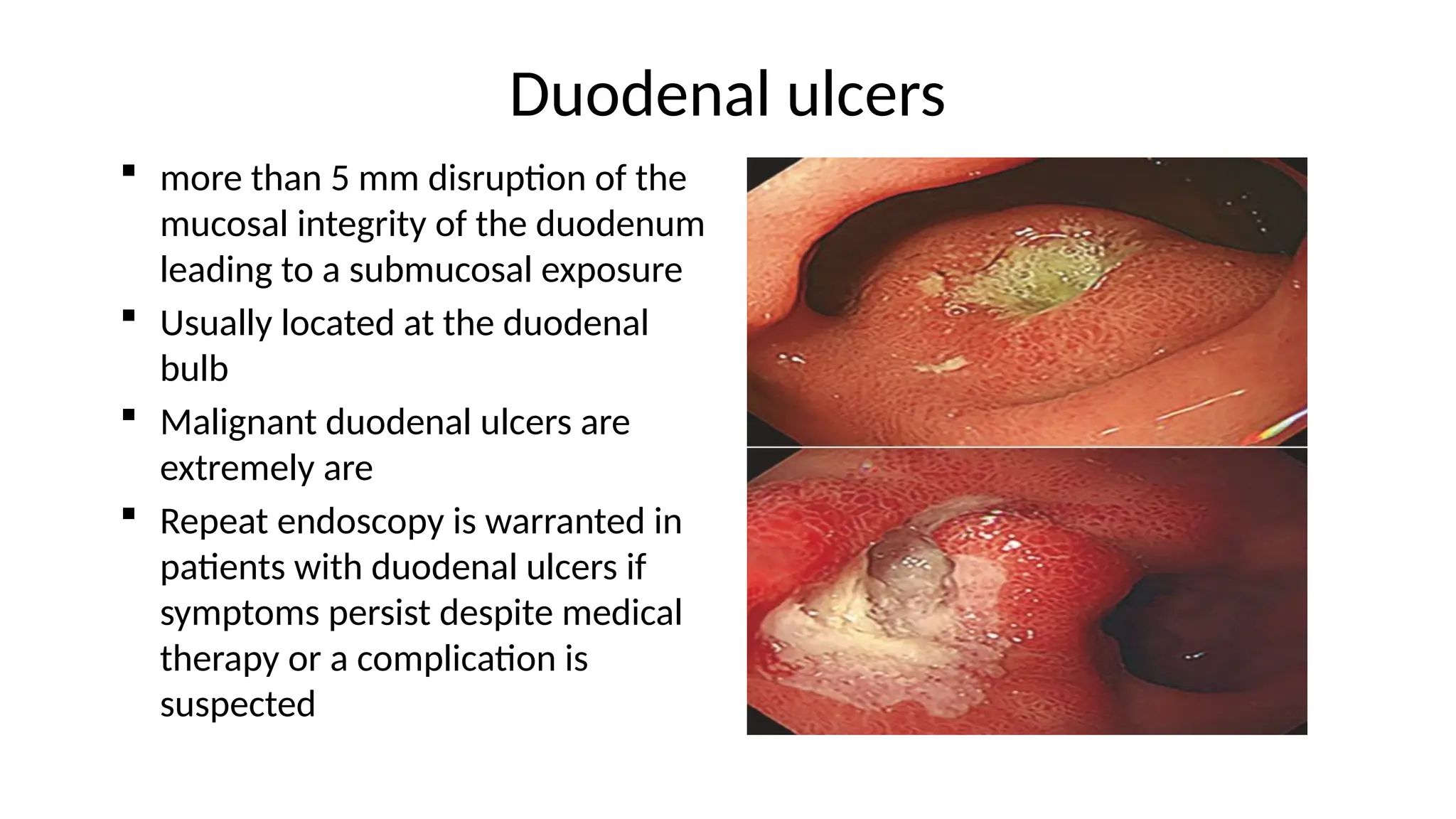
Duodenal ulcers
morethan 5 mm disruption of the
mucosal integrity of the duodenum
leading to a submucosal exposure
Usually located at the duodenal
bulb
Malignant duodenal ulcers are
extremely are
Repeat endoscopy is warranted in
patients with duodenal ulcers if
symptoms persist despite medical
therapy or a complication is
suspected
56.
Duodenal Biopsies
Chronicdiarrhea, iron deficiency anemia suspicion of celiac
disease
Tissue Sampling- 4-6 biopsies in the total from duodenal bulb
and distal duodenum
58.
References
Clinical GastrointestinalEndoscopy, 2nd
edition
Cotton and William’s Practical Gastrointestinal Endoscopy, 7th
edition
Endoscopic mucosal tissue sampling, American society for
gastrointestinal endoscopy, 2013