OBJECTIVES
KNOW WHAT ISQUALITY?
KNOW WHAT IS QUALITY IMPROVEMENT.
UNDERSTAND THE DIFFERENCE BETWEEN QI AND INFORMAL
IMPROVEMENT.
IDENTIFY FOCUS PDCA AND ITS STEPS AS A QUALITY
IMPROVEMENT METHODOLOGY.
PRACTICE DIFFERENT TECHNIQUES AND TOOLS FOR FOCUS PDCA
3.
Introduction
Hospitals are complexsystems of many sum-processes, many
teams sharing the responsibility of maintaining high quality
of services. thus, quality issues better to be solved by teams.
Example: IV infusion pump(BME) used to infuse medicine(by
RN) Which was dispensed from (pharmacy) ordered (by a Dr.)
through HIS(IT) and charged to patient by (Finance).
4.
Hospitals are safe?
Thanksfor joining CQI teams, what you do is
important
http://www.youtube.com/watch?v=BFd54Yzg-
vo
5.
Quality is?
Thedegree to which health services for
individuals and populations increase the
likelihood of desired health outcomes and are
consistent with current professional knowledge.
IOM definition
6.
Quality Improvement
A processof innovation and adaptation designed
to bring about immediate positive changes in the
delivery of health care in particular settings
systematic
data-guided
multidisciplinary
7.
7
Continuous
Quality Improvement
A qualitymanagement model whereby
healthcare is seen as a series of processes and a
system leading to an outcome. QI strives to
make changes in the structural and process
components of care to achieve better outcomes.
8.
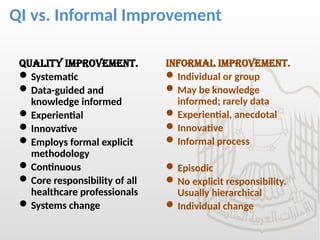
QI vs. InformalImprovement
Quality improvement.
Systematic
Data-guided and
knowledge informed
Experiential
Innovative
Employs formal explicit
methodology
Continuous
Core responsibility of all
healthcare professionals
Systems change
Informal improvement.
Individual or group
May be knowledge
informed; rarely data
Experiential, anecdotal
Innovative
Informal process
Episodic
No explicit responsibility.
Usually hierarchical
Individual change
9.
DIMENTIONS OF QUALITY
STEEP
Safe.
Timely.
Effective.
Efficient.
Equitable.
Patient centered.
Gap in any dimension=NEED IMPROVEMENT
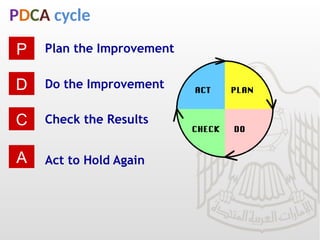
PDCA cycle
Plan theImprovement
Do the Improvement
Check the Results
Act to Hold Again
P
D
C
A
12.
WHEN TO DOPDCA
As a model for continuous improvement.
When starting a new improvement project.
When developing a new or improved design
of a process, product or service.
When implementing any change.
13.
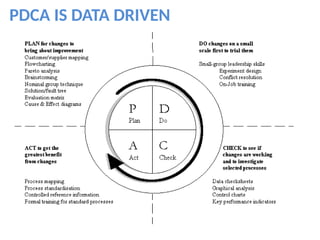
PDCA
The plan–do–check–act cycleis a four–step
model for carrying out change. Just as a circle
has no end, the PDCA cycle should be
repeated again and again for continuous
improvement.
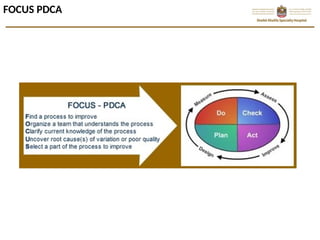
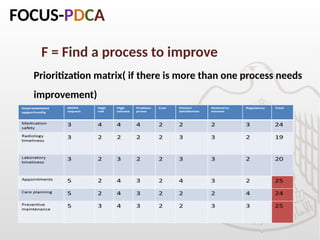
FOCUS-PDCA
F = Finda process to improve
Identify problems & desired outcomes
Review related standards & documents
Analysis of collected data
POSSIBLE SOURCES
Leadership decision.
KPI not meeting target.
OVRs.
Customer satisfactions.
Internal and external audits.
16.
FOCUS-PDCA
F = Finda process to improve
Prioritization matrix( if there is more than one process needs
improvement)
17.
ORGANIZE
O = Organizea team that knows the process
Identify & involve stakeholders (e.g. physicians, nurses, administrative …etc)
Cover all related departments to the improvement initiative
Select team members who best do or know the process to be improved
Involve front liners, they are experts of the process.
18.
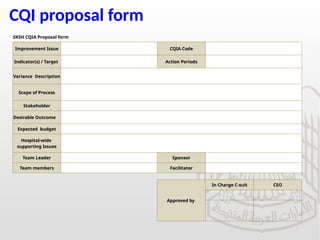
CQI proposal form
SKSHCQIA Proposal form
Improvement Issue CQIA Code
Indicator(s) / Target Action Periods
Variance Description
Scope of Process
Stakeholder
Desirable Outcome
Expected budget
Hospital-wide
supporting Issues
Team Leader Sponsor
Team members Facilitator
Approved by
In Charge C-suit CEO
19.
Team stages
Forming:Meet, define roles & targets, excitement, need to understand.
Storming: Conflict, challenge of authority, different working style, not comfortable with colleagues/workload
Norming: Resolve their differences, appreciate colleagues' strengths, and respect authority of a leader.
Performing: When hard work leads, without friction, to the achievement of the team's goal.
Adjourning: Task completed
20.
Team are fun
•Team work is fun.
• You learn little thing about
everything.
• Know your colleagues.
• Appreciate what other departments
are doing.
• Break intra departmental barriers.
21.
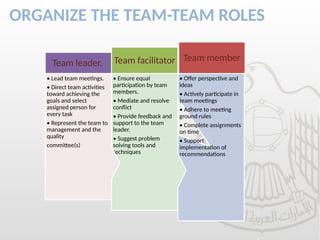
ORGANIZE THE TEAM-TEAMROLES
• Offer perspective and
ideas
• Actively participate in
team meetings
• Adhere to meeting
ground rules
• Complete assignments
on time
• Support
implementation of
recommendations
Team member
• Ensure equal
participation by team
members.
• Mediate and resolve
conflict
• Provide feedback and
support to the team
leader.
• Suggest problem
solving tools and
techniques
Team facilitator
• Lead team meetings.
• Direct team activities
toward achieving the
goals and select
assigned person for
every task
• Represent the team to
management and the
quality
committee(s)
Team leader.
22.
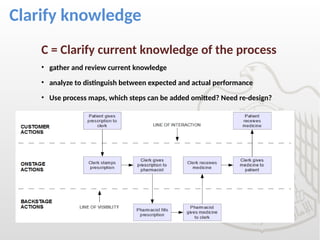
Clarify knowledge
C =Clarify current knowledge of the process
• gather and review current knowledge
• analyze to distinguish between expected and actual performance
• Use process maps, which steps can be added omitted? Need re-design?
UNDERSTAND
U = Understandvariable and causes of variation
Plan and implement data collection
Measure using appropriate indicators
What is wrong with the current process?
What are the root causes of this?
It is not enough to do your best; you must know w
hat to do, and then do your best.
W. Edwards Deming
25.
Find root causes
Brain storming: Share whatever come to your mind.
Avoid:
Arguing with each other
Laughing at other team members ideas
Judging other team members ideas
Group think
RCA(root cause analysis) also known as fish bone.
Multi-voting, nominal voting.
EXCERSIZE MULTIVOTING
26.
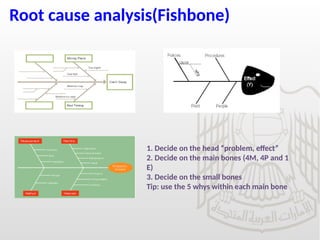
Root cause analysis(Fishbone)
1.Decide on the head “problem, effect”
2. Decide on the main bones (4M, 4P and 1
E)
3. Decide on the small bones
Tip: use the 5 whys within each main bone
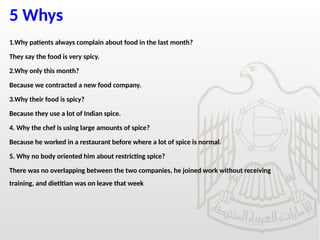
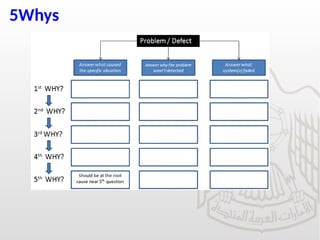
5 Whys
1.Why patientsalways complain about food in the last month?
They say the food is very spicy.
2.Why only this month?
Because we contracted a new food company.
3.Why their food is spicy?
Because they use a lot of Indian spice.
4. Why the chef is using large amounts of spice?
Because he worked in a restaurant before where a lot of spice is normal.
5. Why no body oriented him about restricting spice?
There was no overlapping between the two companies, he joined work without receiving
training, and dietitian was on leave that week
Practice RCA, 5Whys, multi-voting
PRACTICE
In October the hospital received 22 patient
complaints that they had hard time parking
their cars because of non availability of parking
lots
31.
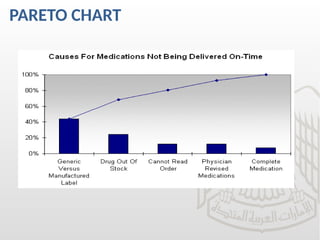
PARETO CHART
20:80Rule: 20% of the contributing factors lead to 80% of the
problems/defects.
Used to prioritize when there is many root causes.
You can know where to focus for efficient utilization of time and effort
Collect data on the causes of the problem
Construct the chart
Draw a line on the 80%
The reason found to the left side of the line are the 20% that cause 80%
of the problem
32.
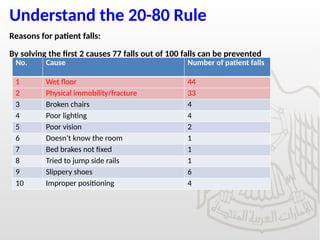
Understand the 20-80Rule
Reasons for patient falls:
By solving the first 2 causes 77 falls out of 100 falls can be prevented
No. Cause Number of patient falls
1 Wet floor 44
2 Physical immobility/fracture 33
3 Broken chairs 4
4 Poor lighting 4
5 Poor vision 2
6 Doesn’t know the room 1
7 Bed brakes not fixed 1
8 Tried to jump side rails 1
9 Slippery shoes 6
10 Improper positioning 4
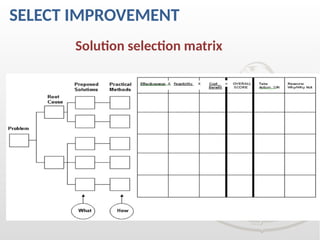
SELECT IMPROVEMENT
Select =the process improvement
Analyze alternative solutions related to process
improvement
Choose the best solution/action that will achieve desired
outcome
Develop approval with a summary of required
information about expected outcomes, resources needed,
time-frame, responsibilities ..etc
CHANGE THE PROCESS
Lessis more?
More is more?
Which step of the current process has no value?
Which step can be added and will add value to the process?
The process change can range from changing one step in one
process to redesigning whole process
38.
SELECT ACTIONS
Criteria forselection:
Leadership support
Practicality
Use friendly
Customer satisfaction
Time effective
Profitability
Cost effective
•Saving potentials
•Resource availability
•Use of tools
•Culturally sensitive
•Availability of team
•Data availability
•Feasibility
•Effectiveness
PDCA-Plan
Plan for improvementproject (initiative):
Assign tasks with agreed criteria checklist & set time
frame
Allocate resources, determine responsibilities & gain
support from all who will be affected by implementation.
Establish monitoring system to collect necessary data to
keep project on the track ( If it is a KPI, no need)
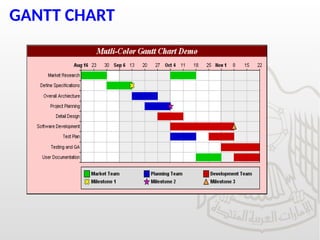
Specify timelines for DO, CHECK, ACT stages(Gantt
CHART).
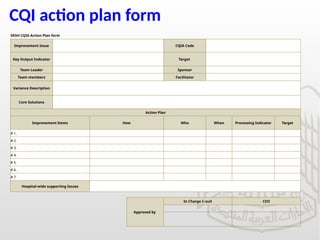
CQI action planform
SKSH CQIA Action Plan form
Improvement Issue CQIA Code
Key Output Indicator Target
Team Leader Sponsor
Team members Facilitator
Variance Description
Core Solutions
Action Plan
Improvement Items How Who When Processing Indicator Target
# 1.
# 2.
# 3.
# 4.
# 5.
# 6.
# 7.
Hospital-wide supporting Issues
Approved by
In Charge C-suit CEO
PDCA-DO
Do the improvementproject:
Implement the best solution stated in FOCUS process.
Empower all people involved by training, education & moral
support.
Collect data & update checklists.
Communicate new change in process-make it a focus.
Monitor compliance with new process (check sheet, audit tools)
In pilot range if possible.
45.
PDCA-CHECK
Check the results
If the desired outcome is obtained & lead expected
improvement.
Compare data collected from FOCUS process with that
during DO( before and after change)
Check for any unexpected, undesired consequences or
outcomes
46.
PDCA-CHECK
Monitor
Monitor theprocess: Staff compliance with the agreed
tool, staff knows the new process, availability of
resources, actions done on time.
Monitor the outcome: KPI target met, Higher customer
satisfaction, pain score within target. Is there any extra
outcome achieved?
THINK ABOUT IT FOR IMPROVEMENT OF PAIN
MANAGEMENT.
PDCA-ACT
Act to holdgains or re-adjust
If improvement initiative is reached; standardize the
process, adjust documents & empower people
Adjust policies, guidelines, process maps(COMMUNICATE)
If improvement initiative is not reached, repeat FOCUS-
PDCA cycle
For both situations, continue to monitor the process to
identify further improvement.
Celebrate the win
50.
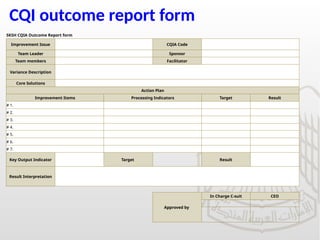
CQI outcome reportform
SKSH CQIA Outcome Report form
Improvement Issue CQIA Code
Team Leader Sponsor
Team members Facilitator
Variance Description
Core Solutions
Action Plan
Improvement Items Processing Indicators Target Result
# 1.
# 2.
# 3.
# 4.
# 5.
# 6.
# 7.
Key Output Indicator Target Result
Result Interpretation
Approved by
In Charge C-suit CEO
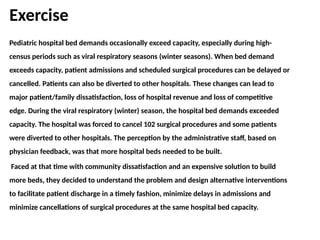
Exercise
Pediatric hospital beddemands occasionally exceed capacity, especially during high-
census periods such as viral respiratory seasons (winter seasons). When bed demand
exceeds capacity, patient admissions and scheduled surgical procedures can be delayed or
cancelled. Patients can also be diverted to other hospitals. These changes can lead to
major patient/family dissatisfaction, loss of hospital revenue and loss of competitive
edge. During the viral respiratory (winter) season, the hospital bed demands exceeded
capacity. The hospital was forced to cancel 102 surgical procedures and some patients
were diverted to other hospitals. The perception by the administrative staff, based on
physician feedback, was that more hospital beds needed to be built.
Faced at that time with community dissatisfaction and an expensive solution to build
more beds, they decided to understand the problem and design alternative interventions
to facilitate patient discharge in a timely fashion, minimize delays in admissions and
minimize cancellations of surgical procedures at the same hospital bed capacity.
REFERENCES
1. Evans andLindsay, the management and control of quality, 6th
edition.
2. James and Mona Fitzsimmons, Service management, 7th
edition.
3. Susan White, Essential recourses for health care quality professionals:
Quality and performance improvement, 3rd
edition.