
Recommended
Recommended
More Related Content
Similar to Title of PaperYour nameHCA375– Continuous Quality Monito.docx
Similar to Title of PaperYour nameHCA375– Continuous Quality Monito.docx (14)
More from juliennehar
More from juliennehar (20)
Recently uploaded
Recently uploaded (20)
Title of PaperYour nameHCA375– Continuous Quality Monito.docx
- 1. Title of Paper Your name HCA375– Continuous Quality Monitoring and Accreditation Type Instructor Name Here Type Date HCA375 - WEEK 4 ASSIGNMENT PART 1 – DETAIL OF THE ADVERSE EVENT CHOSEN Refer to the instructions in the Week 4 Assignment of your online course to understand what is expected in each row. This completed template should be between eight to ten pages in length. Include APA citations within the description row where appropriate. List your references in APA format according to the Ashford Writing Center guidelines on the last page of this template. CONTENT DESCRIPTION ADVERSE EVENT HISTORICAL BACKGROUND LEGAL & ACCREDITING AGENCY REQUIREMENTS CQI TEAM COMMUNICATION OPERATIONAL OR SAFETY PROCESSES
- 2. IMPACT OF THIS EVENT WEEK 4 ASSIGNMENT PART 2 - GRAPH THE DATA You are tasked with graphing the data in Excel for your chosen event. The data is located in the classroom under the Week 4 Assignment Directions. Make sure to use only the data for your chosen event. The directions identify which columns of information to use depending on the chosen adverse event. Once you complete the graph in Excel, copy/paste your graph below. Include an analysis of the data in paragraph format. Discuss the frequency of the adverse event as compared to the increase or decrease of patient discharges. What is the data telling you? What possible factors in your opinion could be attributed to the change? WEEK 4 ASSIGNMENT PART 3 – CQI TOOL · Choose one of the CQI Tools listed below to illustrate the use of the tool with your chosen Adverse Event. · You will be responsible for creating the CQI Tool, completing the tool, taking a screenshot, and copying/pasting the screenshot into the space below. If you are unfamiliar with these tools, please refer to the recommended readings, specifically the article from Week 2, which is listed below. You can locate the article in the Ashford Library.
- 3. · In addition, as a learning resource, the CQI tools listed below are hyperlinked to the Institute for Health Care Improvement website, which discusses and illustrates examples of each type of tool. Siriwardena, A. (2009). Using quality improvement methods for evaluating health care. Quality in Primary Care, 17(3), 155-159. ISSN: 1479-1072 PMID: 19622265 · Choose a CQI Tool that best suits your chosen Adverse Event from the following list. · Fishbone (Cause and Effect) Diagram · Flowchart · Pareto Diagram WEEK 4 ASSIGNMENT PART 4 - FUTURE PREVENTION APPLYING PDSA - Worksheet PHASE PHASE ACTIVITIES EXPLANATION PLAN Problem Objective Team members Communication Data collected Pilot phase DO
- 4. Three possible solutions One solution to implement Result of pilot (create own scenario) Methods of communication STUDY Summarize data Observations and problems Comparison of pilot plan to pilot results Revisions needed to meet objective ACT Revised improvement plan How to Implement the plan hospital wide Plan for monitoring the improvement plan Checks and balance References Excluding your textbook or course readings include at least four scholarly sources in addition to the course text. The sources should be peer-reviewed sources; that were published within the past five years. All references must be cited within the rows where the referenced material was used to support your ideas. The citations and references must be in APA format per the 6th edition guidelines, which can be found at the Ashford Writing Center. These examples are correctly-formatted references. Note that they are in alphabetical order. You may NOT use these examples as your sources.
- 5. 223 What is Special Education? 1 iStockphoto/Thinkstock Pre-Test 1. You can use the terms disability and handicap interchangeably. T/F 2. The history of special education began in Europe. T/F 3. The first American legislation that protected students with disabilities was passed in the 1950s. T/F 4. All students with disabilities should be educated in special education classrooms. T/F 5. Special education law is constantly reinterpreted. T/F Answers can be found at the end of the chapter. 8Real-World Aspects of Quality Improvement iStock/Thinkstock Learning Objectives After reading this chapter, you should be able to do the following: • Summarize the impacts—economic, sociological, safety, and ethical—that a quality improvement project can have on an organization. • Relate the importance of communication and teamwork to a quality improvement project.
- 6. • Examine the ways that organizations can help their employees adapt to change and why this is critical in quality improvement. • Contrast how continuous PDSA is used in quality improvement with other methods described in the book. • Evaluate the principles of continuous quality improvement (CQI) and its importance in healthcare. • Describe the role that social media can play in quality improvement. fin81226_08_c08_223-246.indd 223 10/30/14 7:30 PM Section 8.1 Decision-Making Considerations Introduction Quality improvement is a science that involves close examination of practical concepts that can be widely applied. Much like building a house, quality improvement requires pre- and post-project stages. Every quality improvement project, regardless of scope, will require some investment of time and resources. Just as a contractor would do, a quality improvement team must consider whether available resources are sufficient to complete the proposed project scope and timeline. If the scope is too expansive or the timeline is insufficient, the project may be doomed to fail before it starts. It is also important to consider the sociologic impacts
- 7. and safety issues ahead of time, much like a contractor would do. Thus, a great deal of pre- planning must occur to ensure quality improvement project success. In the post-project stage, quality improvement efforts must be ongoing to ensure long-term sustainability of gains achieved. This is part of an organization’s continuous quality improve- ment program. When building a house, a contractor cannot walk away as soon the home is constructed. There are tests and several rounds of walk-throughs with code inspectors to ensure everything is in working order and up to city standards. The same principle can be applied to quality improvement. There should be continuous monitoring of progress and fine- tuning of quality even after desired improvements are put in place. Lastly, even after a home is sold and occupied it is possible that additional issues (i.e., plumb- ing, electrical) may arise over the long term, prompting the need for additional attention. These types of issues are bound to occur over the lifetime of any home and a contractor would need to revisit the situation and help resolve it. The same is true of quality improvement efforts in healthcare organizations. The task of quality improvement never really ends and remains a continuous process over the lifetime of the organization as its members strive for effective, efficient, safe, patient-centered care. This chapter will review some of the pre- and post-planning efforts that must be part of every quality improvement effort.
- 8. 8.1 Decision-Making Considerations Quality improvement efforts are intended to lead to change and significantly impact the day- to-day operations and interactions in a healthcare setting. This includes the obvious and intended effects of improving a current process or service, but it is also important to con- sider the spillover effects, which are less obvious and possibly unintended impacts from a sociologic, economic, or safety viewpoint. Prior to embarking on a new quality improvement initiative, it is important for the team to closely consider the risks and benefits of proposed changes, which are unique to each project. There are a number of decision-making models that healthcare organizations can use. One is a 10-step process that includes the following steps (Hammond, Keeney, & Raifa, 1999): 1. Identify problems. Collect and analyze facts of what, where, when, how, who, and why (i.e., 6Ws). Describe the impact of a do-nothing approach. Quantify priority and impact of the problem using decision support information. fin81226_08_c08_223-246.indd 224 10/30/14 7:30 PM Section 8.1 Decision-Making Considerations Stockbyte/Thinkstock Cost effective means demonstrating that a
- 9. substantial improvement can be achieved relative to the associated cost or with little costs, such as using trained nurses, instead of pharmacists, who will call to remind patients about the importance of medication compliance. 2. Define objectives. Prioritize potential for improvement in qualitative and quantitative terms. Determine 6Ws. Make them realistic, understandable, measurable, behav- ioral, and achievable (RUMBA). 3. Identify alternatives. Be creative and exhaustive. Define the 6Ws and the contribu- tions to the objectives. Consider benchmarking or comparison to another business entity. Consider economic and legal implications. Define costs and feasibility of each alternative, using decision support information. 4. Understand consequences. Clearly understand the pros and cons of each alterna- tive identified. Decision support systems may help with micro simulation and mock scenario outcomes. Establish potential implementation and problem solving time frames. 5. Assess tradeoffs. Determine the give and take of decision making. Identify the win- ners and losers in a decision process. 6. Clarify uncertainty. Identify the possibilities of changes in the basis of which a deci- sion was made. Decision support systems to identify “what if ” scenarios may help.
- 10. 7. Identify risk tolerance. Determine the amount of, or willingness to take, risks. Avoid common pitfalls of decision making. Try to share risk or seek risk-reducing decision support information. 8. Consider linked decisions. Consider how one decision may affect other decisions or require other decisions to be made. Look at the problem history or healthcare trends that may affect the process. 9. Evaluate and choose an alternative. Based on steps 2 through 8, it must remedy the problem and remain consistent with mission statements, philosophy, and organiza- tional policies. 10. Implement the decision. Follow up on the results and degree of goal achievement. Reorganize, reverse, replace, or revise any lack of problem solution. Hold your gains. Economic Impacts Economic impacts of quality improve- ment projects are important to appre- ciate in current times. Rising medical costs remain a national concern and many healthcare organizations are struggling to decrease medical costs of care (Porter & Lee, 2013). Thus, the quest to improve quality in healthcare must go hand-in-hand with consider- ation of all associated costs.
- 11. For feasibility and sustainability over the long term, a quality improvement project must either be cost saving or cost effective. Cost saving means demonstrating that money can be saved over the long term. Cost effec- tive means demonstrating that a sub- stantial improvement can be achieved relative to the associated cost or with fin81226_08_c08_223-246.indd 225 10/30/14 7:30 PM Section 8.1 Decision-Making Considerations little costs. For example, one way to determine whether a quality improvement initiative is cost effective is to weigh the expected gain against the associated cost. For example, one way for a nursing home to help prevent resident falls is to install a new lighting system for all bathrooms that automatically turns on when the door is opened. Purchasing the lighting sys- tem will cost money, but will make the facility safer for residents. On the other hand, hiring a round-the-clock monitor for each patient at risk for falls is expensive and not sustainable over the long-term. Consider an example in an outpatient medical clinic where the goal is to improve blood pressure control among patients with high blood pressure or hyperten- sion. It’s estimated that 67 million Americans have high blood pressure and only half of them have their condition under control (CDC, 2014a). Yet high blood pressure contributes to over
- 12. 360,000 deaths each year in the United States. The National Committee for Quality Assurance (NCQA) developed Healthcare Effectiveness Data and Information Set (HEDIS) to measure the performance in care and service of health insurance plans and included a measure to deter- mine whether blood pressure is controlled in patients ages 18 to 65 with a diagnosis of hyper- tension. According to a February 2014 report, only 64% of adult patients with diagnosed high blood pressure who are enrolled in HEDIS-reporting health plans had documentation that their blood pressure was controlled (CDC, 2014b). It is no wonder that healthcare organiza- tions are working to improve. An outpatient medical clinic’s quality improvement team may consider a variety of initiatives but may not have the resources to implement more than one initiative per year. Choosing the measure that would have the most impact on patient health and at the same time be the most cost effective initiative would be one way to decide among the list of possible interventions. One intervention that has shown promise is involving nurses or pharmacists to follow up with patients on their treatment plans. For example, pharmacists at the medical clinic may call patients to remind them of the importance of taking their high blood pressure medica- tion. This may prompt more patients to take their medication as prescribed, but it comes with added costs of hiring and maintaining pharmacists in the clinic. Pharmacists typically com- mand high salaries. Therefore, the clinic may consider less costly options: training individu-
- 13. als with a different medical degree and with enough medical background to review medica- tions, such as nurses, or automating the process by using recorded messages or sending text messages. Nurses, for example, could make the same type of reminder phone call, but at a lower wage than pharmacists, which would be more cost effective. Therefore, if both options were thought to improve blood pressure control and medication compliance to a similar degree, it would be most logical to choose the more cost-effective method. In summary, some key questions regarding economic issues include: • What is the cost of proposed change(s)? • Does the cost change over time? • Is there a way to lower cost while achieving the same outcome? • Is this change cost effective or cost saving while achieving the same outcome? In order to answer these questions, it is important to have a budget and detailed overview of project finances as a team is making decisions. Examples of items that must be included in a budget are costs for salaries, training, IT/computer systems, and supplies/materials needed fin81226_08_c08_223-246.indd 226 10/30/14 7:30 PM Section 8.1 Decision-Making Considerations
- 14. to support proposed quality improvement changes. As noted in Chapter 7, many quality improvement teams in large healthcare organizations include financial analysts to help with these types of decisions. Sociologic Impacts In addition to economic impacts, it is also important to consider the sociologic impact of qual- ity improvement initiatives. Examples of sociologic effects include how proposed changes might affect the culture of the organization, the well-being and satisfaction of staff, and the interaction among staff members. A particular solution, although improving a process or ser- vice, can have a negative impact on staff satisfaction or well- being. Consider an example in an outpatient medical clinic where the goal is to improve patient wait times. A proposed change could include increasing the work hours of the clinic physicians by adding mandatory weekend shifts. Clinic staff may prefer the traditional Monday through Friday hours and resent being forced to work on weekends, leading to unanticipated negative impacts, such as poor morale. This may result in increased conflict in the work setting (i.e., if there is disagreement on coverage of holiday shifts) or increased staff turnover. Ironically, this could also negatively impact patient wait times if the clinic were to become short-staffed because of turnover. Thus, it is important to consider the social impact of proposed changes over the short and long term.
- 15. Another example of sociologic impact may involve the need to eliminate employee jobs while making a process more efficient. If a process is automated, then the number of employees required to complete the work may be reduced. This reduction may lead to cost savings and increased efficiency but can significantly impact the social system, or group of employees, within the organization. Will other employees fear for their jobs? Will they resent managers for laying off their colleagues? Will they feel the hospital administration cares only about money and not its workers? Safety and Ethical Issues In addition to economic and sociologic impacts, it is critical that quality improvement teams closely consider safety and ethical issues prior to initiating proposed changes. This is particu- larly true in healthcare systems where patients’ lives are at risk. Consider the previous exam- ple in which physician work hours are increased to reduce patient wait times. If physician work hours are increased so much that they become more fatigued and work continuously without intermittent days off, the likelihood of medical errors may increase. Thus, it would be important to consider how physician hours can be increased within reason, or alternatively, if new physicians can be hired to cover the additional after-hours or weekend shifts. Additional examples of safety issues could include: • Safe deployment of new systems: a new automated medication
- 16. order entry system would need additional checks in place before it can go live through a health system. • Data security issues: ensuring patient privacy is of utmost concern and will have legal implications if data is not properly stored and transmitted. fin81226_08_c08_223-246.indd 227 10/30/14 7:30 PM Section 8.1 Decision-Making Considerations The consideration of ethical issues is also important to keep in mind when conducting quality improvement work. Ethical issues focus on moral behavior and concepts of right and wrong. For example, ethical concerns can arise when quality improvement efforts result in any of the following: 1) harm to patients, staff, or resources; 2) unfair or inequitable care (i.e., a certain group or type of patients receiving benefit over others); or 3) an increase in the self-interest of the healthcare provider or organization (as opposed to the interest of the patients) (Nelson & Gardent, 2008). Most large healthcare organizations have an institutional review board (IRB) or an ethics committee that can resolve any potential ethical issues or concerns that may arise (Nelson & Gardent, 2008). Quality improvement does not occur in a vacuum. It is important that both anticipated and unanticipated ramifications of proposed changes are considered. The risks versus the ben-
- 17. efits of each potential initiative must be weighed carefully so that quality improvement teams can identify the most appropriate initiative. The Patient Voice An emphasis on patient-centered care, or care that is focused on the needs of the patient, and a decision-making process that involves patients and families, is also important (Barry & Edgman-Levitan, 2012). In almost all instances, having the patient voice included in the decision-making process helps ensure that proposed initiatives are appropriate. Patients bring a unique and critical perspective to the decision-making process because they ultimately have the most at stake when healthcare organizations consider change. In many hospitals, patient advisory boards are used to guide quality improvement work. Patient volunteers can also be part of a quality improvement project team. Consider, for example, a pediatric unit that provides care to very ill children. There is a great deal of anxiety that parents feel when their child is admitted to a hospital. Physicians and nurses are aware of this, but parents who have had ill children have lived through the experi- ence and may be in the best position to suggest areas for needed improvement. The input of parents can guide hospital staff as they think through issues such as facilitating the admis- sion process and decreasing the anxiety parents experience. The overall goal of ensuring higher quality care is one of the main areas of emphasis in
- 18. patient-centered care. Patient-centered healthcare organizations are adopting various practices to respond to the needs and preferences expressed by patients and their families. The idea of a patient-centered culture is to try to satisfy what patients are looking for in their healthcare experience. One component is the environment of care itself. Patients often enter the doors of a healthcare facility with heightened feelings of stress, anxiety, and vulnerability. What they find inside can help allay or exacerbate those emotions. Is there a desk manned by a friendly person who can direct them to the laboratory or mammography center? Is the facility clean and safe? Does the physical arrangement help guard patient privacy? Take, for instance, the fact that many patient-centered hospitals have rid themselves of clut- tered corridors. They’ve created solutions (storage areas at the end of hallways or little used closets) to remove clutter and improve patient safety. It’s not only aesthetics at work here. fin81226_08_c08_223-246.indd 228 10/30/14 7:30 PM Section 8.2 The Importance of Communication and Teamwork One of the most frequently cited standards in Joint Commission surveys is a life safety code standard that requires hospitals to maintain the integrity of the means of exit. The fear is that
- 19. medical equipment will block corridors in a fire or emergency, making it difficult to evacuate patients in beds and wheelchairs and putting lives in danger. Questions to Consider 1. You are leading a quality improvement initiative to decrease emergency room wait times. A detailed analysis of the current state and extensive discussion with the emer- gency room staff has led to two proposed initiatives, but hospital leadership has asked you to choose the best option. What are some things to consider in making this type of decision? 2. The team ultimately decides one of the key solutions to reducing wait times in the emer- gency department is to accelerate the receipt of laboratory results. If physicians don’t have to wait as long for lab results, they can diagnose patients and either send them home or admit them into the hospital. This will free up beds for other patients waiting to be seen in the emergency department. What are some of the economic, sociologic, and safety issues surrounding the decision to ensure staff members receive lab results in a more timely manner? 8.2 The Importance of Communication and Teamwork The overwhelming majority of quality improvement work is conducted by groups of people who come together to work on a specific project. These are often referred to as interdisci- plinary teams. Multiple healthcare professionals, administrative
- 20. personnel, and people inter- ested in an issue who volunteer are often represented on these teams. Anytime collaboration occurs, there are two elements that can significantly impact the success of the group project. These elements involve how information is exchanged among group members (communica- tion) and the cohesiveness of the group as a whole (teamwork). When teams come together, they typically go through a number of stages, which are some- times referred to as form, storm, norm, and perform. In the initial stage, forming happens when people first come together. This is the typical “honeymoon” period, where people are initially polite, finding out about one another and the work they will focus on. It’s important to introduce people to each other and ensure people who are naturally quiet are included. The next phase, storm, can occur as the initial politeness wears off, people get more into the work of the team, and start to argue. There may be more than one person who wants to lead the group and asserts dominance. It’s important to resolve differences that can splinter the team. A third phase is the group norm. Roles and personal conflicts are sorted out and people focus on the task at hand. Feeling they are a team, people help one another more. The last phase is perform, in which the team reaches an optimal level of performance. fin81226_08_c08_223-246.indd 229 10/30/14 7:30 PM
- 21. Section 8.2 The Importance of Communication and Teamwork Communication Communication is the way in which individuals exchange information. Communicating effec- tively with patients and families is critical in providing quality healthcare. It’s considered a cornerstone of the patient-centered care discussed earlier. Patients need to understand their health problems and treatment options, know what medications they are being prescribed, and understand any follow-up instructions. Patients should feel free to ask questions about their care and feel that they have a firm grasp of what’s going on with their health. In medicine, ineffective or inaccu- rate information exchange about a patient’s medical case may result in serious injury or even death. During an average four-day hospital stay, a patient may see as many as 50 differ- ent healthcare staff members, includ- ing physicians, nurses, and technicians (O’Daniel & Rosenstein, 2008). It is important for staff to communicate information to patients about their condition, lab results, and tests. It is important to appreciate that com- munication extends beyond words or verbal exchanges. People can use a combination of words, sounds, signs, or nonverbal behaviors to communi- cate with others. In fact, the majority of
- 22. information exchange depends heavily on nonverbal cues, tone, and body language (O’Daniel & Rosenstein, 2008). This is true between staff and patients. Does a physician give a patient her full attention or is she distracted? Does a nurse make eye contact and seem receptive to questions from a patient? Communication is also a key to effective multidisciplinary quality improvement teams. Team members must be able to agree on goals and tackle the tasks at hand. After developing initial trust, team members must be comfortable expressing their differing opinions and challeng- ing others when they don’t agree. It’s important, however, that team members aren’t unpleas- ant and unprofessional. Team members must be able to resolve their differences and allow everyone on the team to participate in the decision-making process. It’s important everyone feels they can express their opinions and views. Teamwork Teamwork is also a critical component of both medical care and quality improvement activi- ties. All improvement methodologies require that a group of individuals come together to work on a quality improvement project. For example, if an organization uses the Six Sigma method (described in Chapter 7), the team may consist of one or more Six Sigma Black Belts iStock/Thinkstock It is critical that effective communication take place between the patient and all of the health providers
- 23. she interacts with. fin81226_08_c08_223-246.indd 230 10/30/14 7:30 PM Section 8.2 The Importance of Communication and Teamwork or experts and one or more Six Sigma Green Belts working closely with a group of provid- ers at the front line (i.e., physicians, nurses, technicians, etc.). Applying lean methodology (described in Chapter 7), the team may consist of a group of front line providers who have come together for a Kaizen event, where the team will collaborate on an improvement project. Or a healthcare organization may not use one of these particular methodologies. It may decide that it wants to pull together a quality improvement team to address a specific prob- lem and includes a variety of people who can help come up with solutions. Members of the team depend on the issue at hand. For instance, a hospital decides it wants to integrate traditional social work functions with the case management department so it can improve discharge planning for patients ready to leave the hospital. As with most changes, initiating such a merger comes with challenges. The hospital forms a broad-based committee that includes supervisors, as well as case managers, who are typically registered nurses, and social workers. It also includes “transitions of care” staff who help patients plan for discharge from the hospital and
- 24. representatives from outside agencies from the community who collaborate with the hospital to ensure patients have the services they need when they get home. It includes the medical director and hospital leaders, including the chief medical officer. In each of these quality improvement scenarios, communication and teamwork are key pre- dictors of ultimate success. If group members do not communicate effectively about data regarding the current situation, it could lead to an inability to identify the true problem(s), the associated root causes, and the ultimate solution. For example, in the case of combining social work and case manage- ment into one department, the team should look at the facility’s average daily patient census, payer mix, demographics, and emergency department use. What is the right mix in terms of the number of social workers and case managers that are needed in the facility? A hospital with a high number of low-income patients may need more social workers. A facility with many elderly patients on Medicare may need an equal number of case managers to deal with medically complex cases and social workers to provide frail elderly patients with community resources when they are discharged from the hospital. Additionally, if the group members are unable to work cohesively, as a team, toward a com- mon solution for the problem at hand, it is unlikely that the project will be completed success- fully (O’Daniel & Rosenstein, 2008). For instance, the last
- 25. thing a hospital trying to merge two departments wants to do is create a battleground between its social workers and case manag- ers. It’s important to bring all parties together to fairly determine the new roles of both social workers and case managers. Ultimately, many staff members will see their responsibilities change, and they must integrate new team members and allow them to take on new duties. The importance of teamwork is heavily emphasized in quality improvement methodologies for these reasons. A list of components of successful teamwork for quality improvement activities include (O’Daniel & Rosenstein, 2008): • Open and effective communication; • Non-punitive environment/avoidance of the blame game; fin81226_08_c08_223-246.indd 231 10/30/14 7:30 PM Section 8.2 The Importance of Communication and Teamwork • Clear and known roles and tasks for group members; • Appropriate balance of member participation for the task at hand; • Respectful atmosphere; • A common goal or direction; • Acknowledgment and processing of conflict; • Clear and known decision-making procedures; and • Regular and routine communication and information sharing. Different quality improvement projects will require various
- 26. team members and range from smaller groups of 1–2 individuals to very large groups of 10 or more members. It’s worth- while to mention that larger teams may not always lead to speedier project completion. This is highlighted by the Mythical Man Month analogy, which states that certain tasks can’t be divided (i.e., they must occur sequentially) so bringing on additional team members does not always add speed (Kim, 2013). In fact, team dynamics may be more complicated as the size and personalities of team members increase. In this and prior chapters, the importance of communication has been emphasized in great detail. In Chapter 7, the importance of a non-punitive organizational culture and avoidance of the traditional “blame-game,” or tendency to identify and punish one individual for a par- ticular error, was also discussed. Clear roles/tasks and balanced participation are also high- lighted by Six Sigma (e.g., Black Belt levels) and lean (e.g., identification of team leaders and clear assignment of medical staff to a Kaizen event for one week as opposed to routine clini- cal duties). A respectful atmosphere and unifying goal are also key components of quality improvement activities, and explicitly discussed as part of lean methodology in Chapter 7. The acknowledgment and attempted resolution of any conflict, clear procedures for making decisions, and routine communication are also just as critical to the success of any quality improvement project. Effective group meetings should include all three of these additional
- 27. components of teamwork. In order to have an effective quality improvement team meeting, it is important to set an agenda for the session; designate member roles, such as who will take minutes; agree on how decisions will be reached; document action items or to-dos; and assure that all members are heard and can play a role in overall project progress (Langley et al., 2009). In other words, effective meetings are those in which decision making follows a delineated process and includes several previously agreed upon steps, providing an avenue for identification and resolution of conflict. Communication and teamwork are critical to any and all quality improvement projects. As such, quality improvement methods emphasize the importance of both as integral to the suc- cess of all quality improvement efforts. fin81226_08_c08_223-246.indd 232 10/30/14 7:30 PM Section 8.3 Adapting to Change 8.3 Adapting to Change Innate to the study and improvement of processes is the need to make change. Understanding and appreciating the human side of change is critical in quality improvement. According to experts, the human side of change helps us understand the motivations of people, how they interact with one another, and how they will react to a specific change in order to gain com- mitment (Langley et al., 2009). Change usually elicits some
- 28. kind of reaction, ranging from total agreement to animosity (Langley et al., 2009). In many situations, change can feel uncomfort- able and may be unwelcomed despite the promise that it will lead to improvements in quality. Consider the case of a hospital pharmacy responsible for processing all inpatient medication orders. A quality improvement project focused on increasing the efficiency by which pre- scriptions are filled may lead to changes in the day-to-day pharmacy operations, such as the order and nature of tasks handled by the pharmacists. Steps the pharmacists routinely fol- lowed may be removed or a series of new steps may be added. The new flow in pharmacy operations will feel foreign to the pharmacy staff and possibly even uncomfortable. Although the pharmacists might appreciate the need to improve efficiency, they are also bound to have a range of reactions to the changes taking place. Thus, preparing the pharmacists for upcom- ing change will be critical to the success of this quality improvement project. The acceptance and commitment to change is critical to the ultimate success of any given quality improvement project. If employees on the front lines do not embrace the proposed change(s), the quality improvement initiative is unlikely to impact day-to-day operations and lead to improvement. Committing to Change To help employees commit to change more readily, organizations should: 1) inform employees
- 29. why change is needed, 2) include them in the way change is created, and 3) notify them of the progress being made after the change (Langley et al., 2009). The first concept involves letting employees know why change is needed so they can understand why a quality improvement project is going to take place. It is important to do this as soon as possible—even before the Questions to Consider 1. In communicating with patients and their family members, it’s important to establish a connection. Providers can fail to do that when they do not truly listen to a patient before responding, don’t introduce themselves to a patient, or don’t acknowledge the patient by name. Can you think of other ways that providers fail to establish communication? Can you establish some guidelines to assist caregivers in establishing effective commu- nication? 2. When a team collaborates on a quality improvement, it is conceivable that conflicts may arise among group members. Consider a scenario where two team members have identified two potential solutions for the problem at hand. What are some components of effective teamwork in resolving this type of conflict in the context of ongoing quality improvement activities? fin81226_08_c08_223-246.indd 233 10/30/14 7:30 PM
- 30. Section 8.3 Adapting to Change quality improvement project team is fully assembled. This way, employees will appreciate why a change is taking place and have as much time as possible to get used to the idea of change. In the case of the hospital merging its social work and case management departments, staff members should know why this change is critical to the organization. It may help to explain that while many hospitals have traditionally separated the two functions, there is a strong movement in the case management field toward a collaborative model that recognizes the partnership of social work and nursing. The change will allow the hospital to use resources more effectively and meet its goals and objectives, such as improving length of stay numbers, reducing readmissions, and increasing patient flow by increasing patient capacity. Including employees in the way change is created can range from asking for their input about a particular step in a process to asking for their participation as a full member of the quality improvement project team. The importance of engaging all employees within the organiza- tion in quality improvement activities was discussed in the context of both Six Sigma and lean methodologies. Gathering input from those who will be most affected by change, such as the pharmacists in the previous example, is critical for several reasons. First,
- 31. the pharmacists have the best understanding of the pharmacy workflow. Their input would therefore provide the most relevant opportunities for making improvements and identifying what problems they expe- rience with existing processes. A project team that does not have a solid understanding of the existing pharmacy system may create a solution that is difficult to implement, possibly leading to further inefficiencies in day-to-day operations. However, by getting input from the pharmacists, or even including them on the project team, it is more likely that the proposed solution(s) will be feasible on the front lines and lead to improvements in efficiency. Once change is being tested and is in place, it is important to inform employees of the ongoing progress. This serves several purposes. The first is a constant reminder of the common goal that everyone is working together to achieve. This helps to decrease any continued resistance and unify the front line staff affected by change. The second is the avoidance of reverting back to the old way of doing things. If everyone is aware progress is being made, there is motivation to continue with change. Lastly, updates on ongoing progress serve as a check that the team is headed in the right direction. If the changes were not leading to the anticipated results, this would be a signal to re-evaluate the new process and consider further adaptations until the desired success is achieved. For example, it is important that hospital leaders support the transition of social workers and
- 32. case managers into one department. It is well and good to plan for a change, but actual imple- mentation may not go as anticipated. Leaders should expect the case management depart- ment will run into obstacles when it actually starts doing the work with combined teams of case management and social workers. It’s important to be flexible and to change processes as needed if issues arise. Quality improvement teams should not be firmly committed to an idea if it does not work. For example, the discharge planning process may work differently on some hospital units. Social workers may provide more services on some units that affect their caseload. So, the quality improvement team may not have foreseen every obstacle or may find that what they expected to happen didn’t work in reality. It’s important that quality teams are prepared to revise their process down the road. fin81226_08_c08_223-246.indd 234 10/30/14 7:30 PM Section 8.3 Adapting to Change The cooperation of front line employees is essential to make effective change (Langley et al., 2009). Front line employees will naturally be concerned about how the change will affect their responsibilities, tasks, and roles within the organization. In our pharmacy example, pharmacists may be asked to give up control of a step in the medication processing flow. It is important for the team to recognize and deal with these concerns (Langley et al., 2009).
- 33. The quality improvement team should listen to these concerns and come up with solutions if possible to ensure the pharmacists are not negatively impacted by the proposed changes. Per- haps they can agree to modify pharmacy staff work hours and improve satisfaction. Or in the case of merging social workers and case managers into one department, the hospital should be prepared to help staff transition into their new roles. In the 1960s, Everett Rogers, professor of communication studies, first described his Diffu- sion of Innovation theory, which includes four main elements (Rogers, 2003): • Innovation: the change or the new idea/practice/object • Communication channels: how information about the innovation is spread • Time: the rate of adoption or the speed with which adoption of an innovation occurs • Social system: the group or related units that are involved in communication, adop- tion, and diffusion In this model, adoption refers to what happens at an individual level, such as when one employee decides to accept a new process (Rogers, 2003). Diffusion, on the other hand, is the spread of change across a group of people, or the collective decision among a group of employees to adopt a change (Rogers, 2003). Within a social system, there are different categories of adopters of change, which vary based on their degree of innovativeness and speed of adoption. There
- 34. are the first individuals to adopt change, or innovators, followed by the second group of early adopters, followed by the early majority, late majority, and finally the laggards (Rogers, 2003). The laggards are the slowest to adopt change and need the most convincing. It is important that organizations understand the varying degrees with which their employees may be committed to the idea of change and willing to adopt new ideas or practices. In doing so, they can outline strategies to help staff adopt change and spread its use more seamlessly across organizations. It’s also important for organizations to be aware of people’s subconscious resistance to change. The subconscious mind wants to keep a person safe and is very resistant to change. So, even if the possibility of change consciously seems exciting and new, the subconscious works against that, doing its utmost to keep people firmly rooted where they currently are because it is safe and familiar. People feel the benefit of staying where they are now, even if consciously they want to move forward and change. Consequently, successful change agents or leaders must always create and communicate to people what’s been referred to as WIIFMs (What’s In It For Me) in order to sustain behavioral changes in employees. Employees who believe they will personally benefit from a change are more likely to accept a new way of doing things. fin81226_08_c08_223-246.indd 235 10/30/14 7:30 PM
- 35. Physiological Needs Breathing, food, water, shelter, clothing, sleep Safety and Security Health, employment, property, family, and social stability Love and Belonging Friendship, family, intimacy, sense of connection Self-Esteem Confidence, achievement, respect of others, the need to be a unique individual Self- Actualization Morality, creativity, spontaneity, acceptance, experience, purpose, meaning, and inner potential Section 8.3 Adapting to Change Motivating Behavior When it comes to motivating behavior, including change, another well-established theory that deserves mention is American psychologist Abraham Maslow’s hierarchy of needs (Maslow, 1943). Maslow (1943) describes a hierarchy of needs that begins with the most fundamental needs, such as food and water, and moves up toward less tangible needs, such as esteem and
- 36. self-confidence. This hierarchy is shown in Figure 8.1. What motivates behavior? According to Maslow, actions are motivated in order to achieve certain needs. Fundamental needs must be met first before a person can transition to higher level needs. This is another framework for consideration when creating and spreading change within an organization. It is important to ensure that change does not hinder basic needs for employees and can promote the attainment of these whenever possible. Changes that threaten employees’ basic needs, such as work breaks and wages, or safety needs, such as job security, seniority, or pensions, will be met with resistance. Figure 8.1: Maslow’s hierarchy of needs Higher order needs can only be achieved once the lower order needs have been met. Source: Maslow, Abraham H., Frager, Robert D., & Fadiman, James. Motivation and Personality, 3rd Edition, © 1987. Printed and electronically reproduced by permission of Pearson Education, Inc., Upper Saddle River, New Jersey. Physiological Needs Breathing, food, water, shelter, clothing, sleep Safety and Security Health, employment, property, family, and social stability Love and Belonging Friendship, family, intimacy, sense of connection
- 37. Self-Esteem Confidence, achievement, respect of others, the need to be a unique individual Self- Actualization Morality, creativity, spontaneity, acceptance, experience, purpose, meaning, and inner potential fin81226_08_c08_223-246.indd 236 10/30/14 7:30 PM Section 8.4 Continuous Use of PDSA 8.4 Continuous Use of PDSA Plan-Do-Study-Act (PDSA) provides a framework and sequence with which quality improve- ment can take place. The four PDSA steps were discussed in detail in Chapter 6. (Just as a reminder, you may sometimes see this described as Plan-Do- Check-Act [PDCA]. However, as this quality improvement model evolved it has been changed to PDSA to encourage organiza- tions to study or analyze the information from its improvement project and determine the success or failure of the interventions undertaken.) With PDSA, it is unlikely that the desired improvement may be achieved in just one cycle (Jain, 2005). It is generally the case that several back-to-back
- 38. cycles of PDSA will occur before a project is completed. In the rare instances where the desired changes are achieved in just one cycle, it is possible that new goals or areas for further improvement will arise, requiring additional cycles (Jain, 2005). Social needs can include a sense of belonging in one’s relationships with others, and can be met with participation in work groups, teamwork, and encouraging participation in the orga- nization. Based on Maslow’s theory, once those needs are met, people can pursue the needs of self-esteem. A worker appreciates recognition for a job well done and recognition will moti- vate them to continue working hard for an organization. Organizations should recognize qual- ity work in many ways, from praise in the presence of peers to promotions. Self-actualization is the highest level in the hierarchy of needs. People are seeking personal growth and are interested in fulfilling their potential. Organizations can do that by providing challenges and encouraging creativity, including problem-solving and quality improvement activities. While a change may be ultimately good for healthcare organizations and their patients, mak- ing a change isn’t always easy for people. Healthcare organizations implementing quality improvement projects need to make it clear why they are making changes and make efforts to get everyone on board. Questions to Consider
- 39. 1. Consider a scenario in an outpatient clinic where an increase in patient dissatisfaction has led to the initiation of a quality improvement project aimed at identifying the exist- ing problems, associated root causes, and potential solutions. What are some key things to consider when discussing the proposed project with the clinic staff ? What should be emphasized to those most affected by the project? 2. In the example provided in Question 1, how would you a) inform the staff why change is needed, b) include the clinic staff in the way change is created, and c) potentially notify the clinic staff of progress being made after change? fin81226_08_c08_223-246.indd 237 10/30/14 7:30 PM Section 8.4 Continuous Use of PDSA With each additional PDSA cycle, it is expected that knowledge about a particular process will increase. Therefore, PDSA cycles are meant to occur in a repeating manner, which is also referred to as iterative—that is, building on the knowledge gained from the previous cycle. In fact, the “A” in PDSA, which usually stands for “Act,” is sometimes also referred to as “Adjust” in order to illustrate the need for additional cycles. Questions to ask in the “A” step of PDSA include: • What have we learned from this test? • Have we achieved the desired effect (ideal state)?
- 40. • Is there room for further improvement? • What other changes could lead to further improvement? • How can we spread the improvement to other areas? Once a PDSA cycle is complete, it is important to assess what was learned and whether the desired goals have been met. If the goals have not been met, which is usually the case after one or two cycles, the project team will need to conduct further cycles. With each PDSA cycle, the team should be planning and testing additional changes to move closer and closer to the ideal desired state. When the desired goals are met, additional cycles may still be required to spread the change. Spreading the change may entail more widespread implementation of the initial test conducted. Recall the pharmacy example from the previous section to help illustrate this further. Suppose the project team plans an intervention to increase the time it takes to process medication orders, replacing the traditional handwritten orders in the patient’s chart with a new com- puter order entry system. Since computer programs are prone to glitches and pharmacists need to learn how to use the new system, a small test incorporating simulated patients is an ideal first step. If glitches in the computer order entry system are not caught and resolved prior to widespread implementation across the entire hospital, the results could be disastrous. If the desired effects are achieved with the small test, the next PDSA cycle could involve real patients but only those in a small section of the hospital. An
- 41. ideal choice for the test would be a unit or floor with patients requiring less acute care. In that case, medication changes are not likely to occur as frequently or be as urgent. Again, if the desired effects are achieved, then testing can be expanded to an even larger section of the hospital until widespread implemen- tation is achieved. Once desired effects are achieved on a hospital-wide basis, additional PDSA cycles may also be used to continually monitor progress in order to sustain quality improvement efforts. In many instances, there is a lot of excitement, enthusiasm, and attention focused on a newly initiated project that can eventually fade over time. In order to keep momentum and ensure the implemented changes result in the desired effects over both the short and long term, additional cycles are necessary. fin81226_08_c08_223-246.indd 238 10/30/14 7:30 PM Section 8.5 Continuous Quality Improvement (CQI) Questions to Consider 1. Suppose you are about to lead a quality improvement project and plan to use PDSA cycles to improve emergency room wait times. How will you describe the PDSA process to your team members? What should they expect when working on a PDSA project?
- 42. 2. Suppose your project in Question 1 is completed after 12 PDSA cycles. Emergency room wait times are now down to an all-time low of one hour per patient. Everyone in the emergency room has been enthusiastic about the changes made. What will you tell your team now? What should they expect would happen moving forward? What are some ways to sustain the improvements implemented? 8.5 Continuous Quality Improvement (CQI) Continuous quality improvement (CQI) is defined as a comprehensive management philoso- phy that applies scientific methods to increase knowledge, reduce variation, and sustain con- tinuous improvement (Tindill & Stewart, 1993). In other words, CQI philosophy states that quality improvement never rests and should be ongoing. Thus, as soon as problems have been identified and improved, a new cycle should begin. The new cycle incorporates the use of analytical decision-making tools, such as Pareto charts or process control charts (described in Chapter 7), to monitor the improved process. CQI Steps CQI involves several steps that can be adapted to any of the process improve- ment methods discussed in prior chap- ters, including Six Sigma or lean the- ory. As a general summary, the steps in CQI can include the following (Kahan & Goodstadt, 1999): Step 1: Identify the problem.
- 43. Step 2: Define the current situ- ation—identify major problem areas in existing processes or day- to-day operations. Step 3: Analyze the problem— identify the root causes of the problem using charts and dia- grams as needed. Step 4: Develop an action plan— outline ways to correct the root causes of the problem and the next specific actions needed to resolve the problem. Shironosov/Thinkstock Step five of Continuous Quality Improvement (CQI) is to examine the results—confirm that the problem and its root causes have decreased, identify whether the target has been met, and display results in graphic format before and after the change. fin81226_08_c08_223-246.indd 239 10/30/14 7:30 PM Section 8.5 Continuous Quality Improvement (CQI) Step 5: Examine the results—confirm the problem and its root causes have decreased, identify whether the target has been met, and display results in graphic format before and after the change.
- 44. Step 6: Start the cycle again—go back to the first step and use the same process to move closer to the ideal state or address another problem. A key feature of CQI is the detection of variation, which is the fluctuation in an existing pro- cess or the tendency to revert back to the old system (see Chapter 7). If variation is detected, then additional processes may be tested and put into place to sustain improvements over the long term. Dr. Walter Shewart is credited with developing the concept of control in respect to variation while he was working to improve quality in the Bell Telephone factories in the 1920s (Statit Software, 2007). Dr. W. Edwards Deming built on the work of Shewart and later took these concepts to Japan, including PDSA, where he was also extremely influential (Statit Software, 2007). Guiding CQI Efforts Several key questions can be continually asked to guide CQI activities. The first involves an assessment of the current state: “How is this process/service doing?” By using analytic meth- ods, it is possible to gather detailed information on how things are going. Once an assess- ment of the current state is conducted, it is possible to ask several other follow-up questions, including: • Can this be more effective? • Can this be faster? • Can this be done with less cost? • Can this be better?
- 45. Consider the pharmacy example discussed earlier, and assume that initial tests and subse- quent larger trials were conducted, leading to hospital-wide implementation of the new com- puterized medication order entry system. The first step in CQI would be continued monitor- ing once the new system is in place. For example, it would be important to know the average turnaround time for a medication order in the new system. By tracking the average time from when a physician entered an order in the system to the delivery of the medication, the quality improvement team would have a measure of process efficiency that could be used as a bench- mark moving forward. By charting the times in a statistical process control chart, the quality improvement team would have a visual representation of this information and allow for rapid identification of any variations in the process. Does the chart show times have decreased since the new system was put in place? The turnaround time for all medications ordered could be averaged and plotted on a daily basis. Significant trends in turnaround times would be easy to detect. The team could also continually ask if there are additional ways to improve the process once the desired state has been achieved. fin81226_08_c08_223-246.indd 240 10/30/14 7:30 PM 1
- 46. LCL = 18.410 15 20 25 30 35 40 45 Average days, positive mammogram to definitive biopsy, control chart Week Avg Delay 1 34 2 30 3 35 4 32 5 28
- 49. 30 17 31 23 32 22 33 24 34 19 35 20 36 21 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 UCL = 43.890 Benchmark Mean = 31.190 LCL = 12.980 UCL = 29.650 Note the Improvements
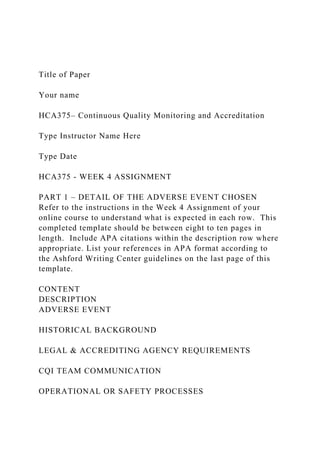
- 50. Mean = 21.313 Section 8.5 Continuous Quality Improvement (CQI) An example of a statistical process control chart, showing the turnaround from the time a suspicious spot was found on a woman’s mammogram test to a follow-up biopsy to determine whether she has breast cancer, is provided in Figure 8.2. Here, the quality improvement effort was aimed at decreasing the average delay in time to biopsy after a mammogram showed a concern for possible breast cancer. The average turnaround time was plotted in weekly incre- ments for patients who received mammograms. Significant decreases in turnaround times are detected after week 20, when the quality improvement initiative had begun. This bench- mark is continually assessed to ensure the gains from the quality improvement initiative are sustained. It is important to note that CQI data analysis and feedback is meant to occur in real time. As illustrated by the examples provided, it would not make much sense to implement a new system and then wait one or two years before understanding whether this has led to improve- ments. In the pharmacy example, it would be important for hospital leadership and front line providers to know as soon as possible whether the new order entry system is improving efficiency. If it is not working as anticipated, then further
- 51. refinements must be made. Waiting extended periods of time or retrospectively collecting data would delay the ability to achieve the desired state within a reasonable time frame. Figure 8.2: Sample statistical process control chart Process control charts allow desired benchmarks (in this case, time from abnormal mammogram to biopsy) to be continually assessed to ensure the gains from the quality improvement initiative are sustained. Source: From “Improving Healthcare with Control Charts” by Raymond G. Carey, PhD. Reprinted by permission 1 LCL = 18.410 15 20 25 30 35 40 45 Average days, positive mammogram to definitive biopsy, control chart
- 55. 36 21 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 UCL = 43.890 Benchmark Mean = 31.190 LCL = 12.980 UCL = 29.650 Note the Improvements Mean = 21.313 fin81226_08_c08_223-246.indd 241 10/30/14 7:30 PM Section 8.6 An Online Presence and Social Media CQI can be adapted to a variety of quality improvement methodologies. In fact, the concepts of continual improvement and use of analytic methods are embedded in PDSA, Six Sigma, and lean methodologies. Thus, CQI is easily added and in many ways already incorporated in the core concepts of existing quality improvement methodologies.
- 56. Questions to Consider 1. You recently led a quality improvement initiative to decrease wait times in the emer- gency room. With the input of emergency room providers, your team tested and ulti- mately implemented a new patient triage system that fast tracks urgent or emergent cases (such as possible heart attacks or strokes) to physicians while common, everyday conditions (such as flu-like symptoms or minor cuts/wounds) are seen by newly hired physician assistants. What type of information should be collected to understand if the new system is working? 2. What are some additional questions your team might want to consider in the first few months after the new triage system is in place? 8.6 An Online Presence and Social Media Online media allows the spread of information about healthcare organizations—both good and bad. You’ve heard the expression “blow your own horn”; when it comes to their quality improvement efforts, some healthcare organizations are doing just that. With people across the globe increasingly using the Internet and social media websites, including blogs and social networking sites such as Facebook, Twitter, and YouTube, for business and personal commu- nications, more and more healthcare organizations are jumping on the bandwagon. After all, if healthcare organizations are using quality improvement for steps such as reducing
- 57. resident falls, avoiding medication errors, or reducing surgical site infections, why hide the good news under a barrel? Healthcare organizations are sharing their successes with patients and potential future customers. Social media is a way for users to participate in communica- tion forums that reach many people. In fact, hundreds of U.S. hospitals are now using social networking tools, with numbers increasing dramatically. Hospitals have their own websites and are finding social media is too difficult to ignore. Healthcare organizations can use social media to reach out to patients with information about their programs and also to educate patients about healthcare issues. Social media also pro- vides a way for consumers to bring a great deal of attention to healthcare issues, both pro and con. They may have good things to say about their care at a healthcare organization. On the flip side, they can also bring attention to poor quality, which can adversely affect an organiza- tion’s reputation. fin81226_08_c08_223-246.indd 242 10/30/14 7:30 PM Summary & Resources One caveat for all healthcare organizations is that they must keep medical information of patients confidential, which is a requirement of the Health Insurance Portability and Account- ability Act (HIPAA) regulations. Healthcare organizations must ensure that patients’ health
- 58. information and pictures are not posted on the Internet without permission. They need to caution staff members about the dangers of blogging about a patient they have cared for if that information allows the patient to be identified. But despite those concerns, healthcare organizations are using social media for marketing, including connecting with patients about the quality improvement taking place within their walls. The Mayo Clinic, which has been a leader in the use of social media, has established a Center for Social Media, which helps other healthcare organizations adopt and explore social media tools. Questions to Consider 1. How might you use social media to spread the word about a quality improvement proj- ect you have just led? 2. What type of information should you share on social media? Is there information you should not publicize? Summary & Resources Chapter Summary This chapter reviewed the pre- and post-project efforts that must be part of all quality improvement activities. In the pre-project phase, it is important to consider the economic, sociologic, and safety impacts a project may have. The risks versus benefits of each project and associated solutions must be weighed carefully. The project
- 59. scope and timeline must align with available resources. Effective communication and teamwork are also necessary to move the project forward smoothly. It is important to keep the lines of communication open among the team members and between the team and the rest of the organization. Preparing the organization for upcoming change is critical to help everyone adapt and move forward in unison. Once a project achieves the desired state, continuous monitoring is needed to ensure these gains can be sustained. Quality improvement never really ends and should be consid- ered a continuous process. Social media is a new way for organizations to share the progress made in improving patient care through their quality improvement efforts. Mini Case Study If it takes a village to raise a child, it takes more than physicians and nurses to make a hos- pital. A hospital must ensure the quality and delivery of a range of services that include feed- ing patients and employees; managing the facility; transporting patients; maintaining clini- cal equipment; safeguarding the facility; and providing a clean, comfortable environment. fin81226_08_c08_223-246.indd 243 10/30/14 7:30 PM Summary & Resources Consider the role that a hospital’s safety officer and facility management play in ensuring
- 60. patient satisfaction. Facility department staff undertake all kinds of jobs, from changing light bulbs to unclogging toilets and cleaning rooms—all tasks needed to maintain a safe and comfortable environment. But just what role does facility management play in improving the quality of patient care? When the hospital where he worked as the safety officer launched an initiative to improve hand hygiene, Joe Thomas didn’t see how his department would be involved. However, the facility department staff played a role. Caregivers need to wash their hands every time before they touch a patient or they increase the risk for hospital-associated infections. However, if the sink in the room is broken, caregivers might skip washing their hands or instead go into the next room to wash their hands, which can increase the risk of cross- contamination if germs from one patient are spread to another. Therefore, Joe and the main- tenance staff committed to fixing sinks throughout the facility within 24 hours of receiving a work order for a repair. The facility management department has tracked performance and found that 97% of sinks are fixed within 24 hours of a report. Discussion Questions 1. What are some ways non-clinical staff can contribute to improving patient care? What are some of the most important contributions various departments make to patient care? What role can those departments play in improving quality?
- 61. 2. What other ways can the facility maintenance department help improve quality? Key Terms adoption Accepting change at an individual level, such as when one employee decides to adopt a new process. communication channels How informa- tion about the innovation is spread. continuous PDSA Several back-to-back PDSA cycles to move from the present situa- tion to the ideal future situation. cost effective Demonstrating that a sub- stantial improvement can be achieved rela- tive to the associated cost or with little cost. cost saving Demonstrating that money can be saved over the long term. diffusion The spread of change across a group of people, or the collective decision among a group of employees to adopt a change. innovation The change; the new idea/ practice/object. social system The group or related units that are involved in communication, adop- tion, and diffusion.
- 62. time The rate of adoption or the speed with which adoption of an innovation occurs. variation Fluctuation in an existing process or the tendency to revert back to the old system. fin81226_08_c08_223-246.indd 244 10/30/14 7:30 PM Summary & Resources Critical Thinking Questions 1. You have been assigned to lead a quality improvement effort on the inpatient oncol- ogy ward. One of the main goals is to improve the efficiency with which the medical team evaluates and manages ongoing medical issues. Ideally, this effort should help decrease patient length of hospital stay, which may also result in cost savings for the hospital. What are some social and ethical considerations that might be relevant to this case? 2. What are the benefits of conducting quality improvement activities in a continuous fashion? What are the downsides, if any? 3. In what ways do the concepts discussed in this chapter, such as PDSA and CQI, over- lap with methodologies, such as lean or Six Sigma, covered in a prior chapter? Are there notable differences?
- 63. Suggested Websites • U.S. Department of Health and Human Services (HHS): https://www.childwelfare.gov/management/reform/soc/communi cate/initiative /soctoolkits/cqi.cfm#phase=pre-planning This website provides a review of Continuous Quality Improvement. • Agency for Healthcare Research and Quality (AHRQ): http://www.ahrq.gov/ This website provides information on evidence to make healthcare safer, higher quality, more accessible, equitable, and affordable. • National Center for Biotechnology Information (NCBI): http://www.ncbi.nlm.nih.gov/books/NBK2651/ This website includes a 51-chapter book on quality improvement in the healthcare setting [Hughes, R. G. (Ed.). (2008, March). Patient safety and quality: An evidence- based handbook for nurses (Prepared with support from the Robert Wood Johnson Foundation; AHRQ Publication No. 08-0043). Rockville, MD: Agency for Healthcare Research and Quality.]. • Robert Wood Johnson Foundation: http://www.rwjf.org/en/research-publications/research- features/evaluating-CQI.html This website describes the Robert Wood Johnson Foundation, which has worked to improve the health and healthcare of all Americans, including information on the Science of Continuous Quality Improvement.
- 64. • Communication Theory: http://communicationtheory.org/shannon-and-weaver-model-of- communication/ This website reviews the Shannon and Weaver Model of Communication. • Business Communication Answers: http://www.answers.com/Q/Shannon_weaver_model_of_commu nication This website includes information on the Shannon and Weaver Model of Communication. fin81226_08_c08_223-246.indd 245 10/30/14 7:30 PM https://www.childwelfare.gov/management/reform/soc/communi cate/initiative/soctoolkits/cqi.cfm#phase=pre-planning https://www.childwelfare.gov/management/reform/soc/communi cate/initiative/soctoolkits/cqi.cfm#phase=pre-planning http://www.ahrq.gov/ http://www.ncbi.nlm.nih.gov/books/NBK2651/ http://www.rwjf.org/en/research-publications/research- features/evaluating-CQI.html http://communicationtheory.org/shannon-and-weaver-model-of- communication/ http://www.answers.com/Q/Shannon_weaver_model_of_commu nication fin81226_08_c08_223-246.indd 246 10/30/14 7:30 PM 177
- 65. What is Special Education? 1 iStockphoto/Thinkstock Pre-Test 1. You can use the terms disability and handicap interchangeably. T/F 2. The history of special education began in Europe. T/F 3. The first American legislation that protected students with disabilities was passed in the 1950s. T/F 4. All students with disabilities should be educated in special education classrooms. T/F 5. Special education law is constantly reinterpreted. T/F Answers can be found at the end of the chapter. 7Two Methods of Quality Improvement: Six Sigma and Lean Theory KEENE/BSIP/SuperStock Learning Objectives After reading this chapter, you should be able to do the following: • Evaluate Six Sigma and its role in quality improvement. • Describe the Six Sigma Belts and metrics used. • Analyze the five steps that define Six Sigma. • Compare and contrast the successes and limitations of Six Sigma.
- 66. • Describe the origin and evolution of lean theory from the manufacturing industry. • Summarize core principles of lean theory implementation. • Explain fundamental concepts and methods used in lean methodology. • Discuss examples of lean projects in healthcare. fin81226_07_c07_177-222.indd 177 10/30/14 7:26 PM Introduction Introduction Compared to other developed countries, such as the United Kingdom, France, or Canada, the United States spends more money on healthcare but has poorer healthcare outcomes (Col- laborators, U.S. Burden of Disease, 2013; Squires, 2011). In 2012, healthcare spending in the United States was $8,895 per capita, the third highest in the world (only Norway and Swit- zerland had a higher per capita rate, at $9,055 and $8,980 respectively; see Table 7.1) (World Bank, 2012). Table 7.1: The top 15 countries for healthcare expenditure per capita Country Expenditure per capita Norway $9,055
- 67. Switzerland $8,980 United States $8,895 Luxembourg $7,452 Monaco $6,708 Denmark $6,304 Australia $6,140 Canada $5,741 Netherlands $5,737 Austria $5,407 Sweden $5,319 Japan $4,752 Belgium $4,711 France $4,690 Germany $4,683 Source: World Bank. (2012). Health expenditure per capita (current US$). Retrieved from http://data.worldbank.org/indicator /SH.XPD.PCAP/countries Despite this higher investment, the United States struggles with lower quality healthcare, fin- ishing far worse than many of its counterparts on various health
- 68. outcomes. These outcomes include higher infant mortality rates, higher rates of hospital admissions for most chronic diseases, and the highest rate of foot amputations for patients with diabetes (see Table 7.2) (Squires, 2011). fin81226_07_c07_177-222.indd 178 10/30/14 7:26 PM http://data.worldbank.org/indicator/SH.XPD.PCAP/countries http://data.worldbank.org/indicator/SH.XPD.PCAP/countries Introduction T a b le 7 .2 : A c o m p a ri so
- 87. a no t a va ila bl e fo r A us tr al ia . a 2 00 6. b 2 00 5. c U .S . d
- 91. qu ir es , D . A . ( 2 0 1 1 ). T h e U .S . h ea lt h s ys te m
- 94. 6 , 1 4 . R ep ri n te d by p er m is si on o f T h e Co m m on
- 95. w ea lt h F u n d. fin81226_07_c07_177-222.indd 179 10/30/14 7:26 PM Section 7.1 Definition and History of Six Sigma A 2013 report published in the Journal of the American Medical Association confirmed that overall mortality rates in the United States still lag behind many countries, including sev- eral with much lower gross domestic product and healthcare spending, such as Chile, South Korea, and Slovenia (Collaborators, U.S. Burden of Disease, 2013). Improving healthcare quality and efficiency, while simultaneously curbing rising medical costs, is a major goal for U.S. healthcare organizations (Toussaint & Berry, 2013). To achieve a higher level of quality, healthcare organizations must use a systematic approach to improve- ment. First, they need to recognize healthcare problems within their organization. Next, they must determine their goals for improvements in quality, as well
- 96. as the changes required to achieve them. Finally, they need to measure the impact and monitor to ensure that enhance- ments in quality are appreciable and sustained. Many of the widely accepted methods to improve quality originated in the manufacturing world and are now increasingly being applied to healthcare. In this chapter, we will examine two popular methods of quality improvement—Six Sigma and lean theory—and how they can be used to improve healthcare operations. Methods of quality improvement have some basics in common. Process improvement meth- odologies provide an established and systematic approach to improving processes. Usually these methodologies include a step-by-step guide to help organizations identify problems, implement interventions, measure the impact of changes, and monitor processes so that improvements in care are sustained. The overarching goal for any quality improvement method is to reduce the number of defects in a product or process as much as possible. Defects are deficiencies in the process being eval- uated—in other words, a result that is outside of the established parameters or benchmarks. Some of the common healthcare organizational processes that might be the target for quality improvement include improving waiting room times, surgery scheduling, and patient satis- faction. A secondary goal is to reduce costs or save the organization money. The added goal of sustaining improvements is also critical to quality improvement
- 97. methods. This is emphasized because organizations need to avoid the natural tendency to revert back to old processes, which can lead to variability in quality over time. Let’s take a look at the details of two process improvement methodologies: Six Sigma and lean theory. 7.1 Definition and History of Six Sigma Six Sigma is one of the most well-known process improvement methodologies, and it has been adopted by many healthcare organizations over the last 20 years. It has been described as a disciplined and quantitative approach to process improvement methodology (Hahn, Hill, Hoerl, & Zinkgraf, 1999; Markarian, 2004). Central features of Six Sigma include (Antony, 2004; Schroeder, Linderman, Liedtke, & Choo, 2008): 1. A clear focus on measurable financial results; 2. Emphasis on data collection and analyses; 3. A defined structure with specified steps and tools; 4. Use of dedicated Six Sigma specialists within the organization; and 5. Emphasis on leadership support and engagement. fin81226_07_c07_177-222.indd 180 10/30/14 7:26 PM Section 7.1 Definition and History of Six Sigma Six Sigma History In 1987, Motorola Company formally introduced Six Sigma as a new way to decrease the number of defects in manufacturing (Schroeder et al.,
- 98. 2008). Soon after, the methodology was adopted by some of the country’s leading companies, including Honey- well (which was acquired by AlliedSig- nal) in 1994 and GE in 1995. In the early 1990s, the healthcare industry began to embrace process improvement methodology and qual- ity management approaches. In 1993, one study showed that 44% of 1,083 U.S. hospitals surveyed applied some form of quality management approach (Choufournier & St. Andre, 1993). Beginning in 2000, reports were published on the successful implementation of Six Sigma at hospitals across the United States, signifying a new chapter in Six Sigma history. One of the most cited examples came from Heidi L. Frankel, MD, and colleagues who used Six Sigma methodology to reduce catheter-related bloodstream infections at Yale New Haven Hospital (Frankel et al., 2005). Other applications of Six Sigma in healthcare include Stanford Medical Center in California and the Red Cross Hospitals in the Netherlands (Koning, Verver, Heuvel, Bisgaard, & Does, 2006). While healthcare organizations are adopting Six Sigma techniques, it is not clear if they are using the process correctly. In 2013, a comprehensive literature review found over 300 articles published on the use of Six Sigma in healthcare management (Dellifraine, Wang, McCaughey, Langabeer, & Erwin, 2013). Among these, 55
- 99. articles were peer reviewed, but only 16 reported correct use of Six Sigma. Based on these findings, the authors concluded that the evidence that Six Sigma is being used correctly in healthcare remains “weak” (Delli- fraine et al., 2013). This review also reported the increasing number of hybrid models, which include combined elements of Six Sigma and lean quality improvement methodologies (lean will be discussed later in this chapter). Together these are referred to as lean Six Sigma; they can be used as complementary tools for quality improvement. A brief timeline of major events in the history of Six Sigma is included in Table 7.3. AP Photo/LM Otero Motorola Company formally introduced the concept of Six Sigma as a new way to decrease the number of defects in manufacturing in 1987. fin81226_07_c07_177-222.indd 181 10/30/14 7:26 PM Section 7.1 Definition and History of Six Sigma Table 7.3: Historical timeline of major events in Six Sigma history Year Milestone 1985 Motorola needs to make major changes to deal with growing competition from Japan and begins to create Six Sigma.
- 100. 1987 Six Sigma concept formally introduced by Motorola. 1988 Motorola wins the Malcolm Baldrige Award for Quality and reports $940 million in savings from Six Sigma. 1994 Honeywell (acquired by AlliedSignal) adopts Six Sigma. 1995 GE adopts Six Sigma. 1997 Honeywell reports successful implementation of Six Sigma, resulting in less than 3.4 defects per million products manufactured. 1999 GE reports net income from Six Sigma exceeding $2 billion. 2003 Reports of successful implementation of Six Sigma in several healthcare organizations, includ- ing Good Samaritan Health System in Kearney, Nebraska; the Charleston Area Medical Center (CAMC) in West Virginia; and Mount Carmel Health System in Columbus, Ohio. 2013 A total of over 300 articles (to date) published on the use of Six Sigma in healthcare. Sources: Antony, J. (2004). Some pros and cons of Six Sigma: An academic perspective. The TQM Magazine, 16(4), 303–306; Schroeder, R. G., Linderman, K., Liedtke, C., & Choo, A. S. (2008). Six Sigma: Definition and underlying theory. Journal of Operations Management, 26(4), 536–554. While rooted in manufacturing, Six Sigma is helping healthcare
- 101. organizations to improve their processes and patient care. Six Sigma Explained The technical definition of Six Sigma is to strive for less than 3.4 defects per million opportu- nities (DPMO), in any process, product, or service (Hahn et al., 1999; Linderman, Schroeder, Zaheer, Choo, & Carlson, 2003). Sigma refers to the Greek letter (represented by the Σ in lower case Greek) that is used in statistics to measure how far something deviates from per- fection. The “six” refers to a statistical calculation worked out by the creators of Six Sigma, which aims for a very high percentage of defect-free products. At Motorola, William Smith, John Mitchell, and Robert Galvin are credited as the masterminds behind the Six Sigma concept (Hahn et al., 1999). They combined two rules to derive the now infamous 3.4 DPMO value. The first is the well-known empirical rule in statistics, which states that nearly all values (or 99.7%, to be exact) lie within three standard deviations of the mean. The second rule was an assumption based on the creators’ experiences in the manufacturing world (Hahn et al., 1999; Kumar, Nowicki, Ramírez-Márquez, & Verma, 2008). Their assump- tion was that even the most controlled manufacturing processes eventually vary, or drift away from perfection (specifically 1.5 standard deviations) over time. In the case of a hospital seeking to improve hand hygiene among staff members to reduce the number of infections and therefore achieve healthier outcomes for patients and reduced
- 102. recovery times, the organization can expect compliance to be high after the initial launch of its initiative. As part of the roll-out, staff members will receive training on hand hygiene fin81226_07_c07_177-222.indd 182 10/30/14 7:26 PM Section 7.2 Six Sigma Quality Improvement Questions to Consider 1. What are two specific examples of ways to improve quality of care in a clinic, hospital, pharmacy, or outpatient laboratory setting? 2. What are some important points to consider when applying quality improvement pro- cesses in healthcare? protocols during meetings on each hospital floor. They will be reminded about the hand hygiene policy at regular staff meetings. Supervisors will monitor to see if staff members are following the protocols. However, after six months, there may be less emphasis on hand hygiene. Supervisors may be focused on other priorities. Some staff members may become less vigilant about following the protocols and slip into old habits. While infection rates may have dropped because of hand hygiene, the hospital may now see a gradual increase in these numbers. Therefore, over the long term, it may become increasingly difficult to maintain the same
- 103. level of quality. This variation in process over the long term is what the originators of Six Sigma tried to capture mathematically. How do you calculate the now-infamous 3.4 DPMO, which is one of the key measurements of a Six Sigma quality system? A process is said to be operating at Six Sigma if the DPMO is 3.4 or less. If a defect means, for instance, a patient acquiring an infection, then for every mil- lion patients, fewer than four would acquire a healthcare- associated infection. Of course, in healthcare, even one patient with an infection is one too many. As they did with manufacturing, the Six Sigma concept can improve healthcare quality, enhance patient satisfaction, and allow an organization to compete with others in a competi- tive market. 7.2 Six Sigma Quality Improvement Just as some of the largest and most successful U.S. companies have adopted Six Sigma, the healthcare industry provides numerous examples of successful Six Sigma implementation. Numerous studies have tried to dissect the inner workings of the most notable Six Sigma organizations to reveal the secrets of their success (Hahn et al., 1999; Schroeder et al., 2008; Senapati, 2004). These studies have shown that many manufacturing companies employ the use of parallel-meso structures to support Six Sigma activities (Schroeder et al., 2008). Paral- lel structures operate outside of and do not directly interfere with daily operations. Thus, to
- 104. ensure success, Six Sigma activities are usually supported in ways that do not alter “normal” operations of an organization. An example of parallel support for Six Sigma activities include dedicated Six Sigma specialists within the organization. These individuals are specifically trained in Six Sigma methodology and work with existing personnel and processes to improve quality. The significant time com- mitment to manage and move quality improvement projects forward lies on the shoulders of fin81226_07_c07_177-222.indd 183 10/30/14 7:26 PM Section 7.2 Six Sigma Quality Improvement these specialists so that daily processes and routines are minimally disrupted. In a healthcare setting, the Six Sigma specialists, who might be physicians, nurses, and others in the organiza- tion, would oversee quality improvement projects, while other personnel remain focused on their daily responsibilities. Healthcare organizations can implement Six Sigma by bringing in experts in this improvement process from outside the organization and teaching them about how healthcare works or by sending their own personnel to learn the Six Sigma methods. For instance, an organization can send physicians, nurses, and other leaders to seminars to train in Six Sigma and bring their knowledge back to the facility. Additionally, meso theory describes the integration of data at
- 105. multiple levels, ranging from micro- to macro-level (Schroeder et al., 2008). Micro level data is very detailed and can include information about individual steps in a process (e.g., the amount of time it takes to register a patient). Macro level data is less detailed and can include information about the process as a whole (e.g., the average length of stay for patients admitted to the hospital). Six Sigma projects require the connection of multiple pieces of information within one orga- nization. This can occur in several ways. Examples include the engagement of participants from various levels within the organization (i.e., from front line workers to leadership) to col- laborate on one project and the integration of various pieces of data from different steps within the process to improve one final product or service (Schroeder et al., 2008). Six Sigma Belts The use of full-time Six Sigma specialists within organizations is a unique attribute of this method- ology. It is not unusual to have dedicated Six Sigma specialists who spend 50% to 100% of their time on Six Sigma-related activities (Hahn et al., 1999; Schroeder et al., 2008). Different companies use var- ious names to describe the individuals working on Six Sigma projects, but the most widely known are the Black Belts, who typically run these improve- ment projects. While others with less training in Six Sigma may be involved in projects and collect data, the structure, reports, and number analysis is typi- cally done by Black Belts. In the Six Sigma methods, white, yellow, and green belt describe individuals
- 106. with less intense training. Black Belts are typically selected to attend at least four weeks of intense Six Sigma training, which provides review as well as hands-on application of quantita- tive methods (including statistical programs) (Hoerl, 2001). Qualitative skills in the areas of team leader- ship and communication are also usually covered, but are emphasized less (Hahn et al., 1999; Hoerl, 2001). The number of Six Sigma belts will vary depending on the available resources, size of the com- pany or organization, and scope of projects. As a general guideline, most companies aim to have AndreyPopov/iStock/Thinkstock “Black Belts,” the most widely used name to describe individuals working on Six Sigma projects, are typically selected to attend at least four weeks of intense Six Sigma training. fin81226_07_c07_177-222.indd 184 10/30/14 7:26 PM Section 7.2 Six Sigma Quality Improvement 1% of their workforce trained at the Black Belt level (North Carolina State University Lean Six Sigma, n.d.). Most Six Sigma projects take an average of four to six months to complete. Black Belts should be able to support three to four large-scale projects annually. Thus, it is estimated that two to three full-time Black Belts are needed to support
- 107. quality improvement activities in a typical acute care hospital with 150 to 300 beds (Caldwell Butler & Associates, n.d.). When Six Sigma is adopted within an organization, individuals are usually first trained by external experts. Trainees typically have the opportunity to progress through belt levels. It is important to note that the Six Sigma certification and training processes are not stan- dardized across organizations. Currently, there is no single society or council that provides Six Sigma certification. A survey of businesses found that companies with fewer than 500 employees were reporting an average of $10,000 or less in total costs of Six Sigma implemen- tation each year (Dusharme, 2004). Additionally, companies that have adopted Six Sigma over many years eventually provide internal training and certification programs that are tailored to the company as needed. Thus, studies have demonstrated that the skills and expertise developed by Black Belts are inconsistent among companies (Antony, 2004). Executive leadership plays a key role in all Six Sigma activities. Leadership must first provide adequate support for these activities in the form of funding. It is impossible to implement Six Sigma methods without spending money to certify employees and paying the salaries to retain experienced Black Belts and higher level Master Black Belts. Leadership may also need to provide additional resources for a particular project. As an example, the use of informa-
- 108. tion technology (IT) support services to assist with data collection, monitoring, and analysis would require leadership approval. Additionally, leadership must align Six Sigma activities with company priorities and values. Leadership must encourage participation and enthusiasm around Six Sigma activities at all levels. Leadership should also promote a culture that empowers employees to seek oppor- tunities to improve quality, rather than being content with the status quo. Senior executives’ continuous support and engagement is necessary to successfully carry out Six Sigma projects (Schroeder et al., 2008). Thus, involvement of executive leadership is critical to the success of Six Sigma in any organization. Six Sigma Metrics Metrics are specialized measures that play a central role in all Six Sigma improvement proj- ects. They are measureable factors that provide useful information about the performance of a process. A variety of metrics can be employed in Six Sigma projects; they will generally fall under one of two categories: 1) customer-oriented metrics and 2) financial metrics. Customer-Oriented Metrics Customer-oriented metrics are measurements of performance from the customer’s perspec- tive. Also referred to as critical-to-quality (CTQ) characteristics, these metrics are defined as key measurable characteristics of a process or product that are essential for customer sat- isfaction (Antony, 2004). Healthcare organizations may
- 109. consider medication errors or emer- gency room throughput as examples of customer-oriented metrics. It is easy to imagine the impact on patient satisfaction, not to mention patient well- being, if medication doses were fin81226_07_c07_177-222.indd 185 10/30/14 7:26 PM Section 7.2 Six Sigma Quality Improvement erroneously mixed up or emergency room wait times were too long. Examples of metrics are included in Table 7.4. Table 7.4: Examples of two CTQ projects Project Example Example CTQ Metric Wait times to obtain new obstetrical visits Patient time spent in obstetrical clinic Benefits Reduced from 38 to 8 days 52% reduction Sources: Kwak, Y. H., & Anbari, F. T. (2006). Benefits, obstacles, and future of Six Sigma approach. Technovation, 26(5–6), 708–715; Bush, S. H., Lao, M. R., Simmons, K. L., Goode, J. H., Cunningham, S. A., & Calhoun, B. C. (2007). Patient access and clinical efficiency improvement in a resident hospital-based women’s medicine center clinic. American Journal of Managed Care, 13(12), 686– 690. Customer-oriented metrics can provide a picture of how well a
- 110. healthcare organization is performing in the eyes of its patients. Financial Metrics Six Sigma projects are usually selected based on their potential to improve specified met- rics and have a financial impact. Financial metrics are measurements of monetary impact. Examples include the amount of money saved when processes are made more efficient or the additional amount of money generated. For instance, a healthcare organization can bring in increased revenues by performing more surgeries with high reimbursement levels or attract- ing more patients. While businesses may select improvement projects that will generate high levels of annual savings or benefits, it may not be realistic for many healthcare organizations to expect such high levels of return. Many large organizations routinely monitor and report their financial results; therefore, the incorporation of a financial analyst on their Six Sigma teams is common (Schroeder et al., 2008). Financial analysts collect data in real time as projects unfold, but also track outcomes beyond just one project cycle (this can vary depending on the project but typically could include tracking results several months to one year pre-project and one year post-project). Examples of reported financial metrics are provided in Table 7.5. Table 7.5: Examples of financial metrics from Six Sigma healthcare organizations
- 111. Healthcare organization Savings Women and Children’s Hospital (Charleston Area Medical Center) Gross obstetrics and gynecology clinic revenue increase of 73% in the first 6 months of 2006 (Bush et al., 2007) Radiology Department in a Hospital (Taiwan) Savings of $36,000 from reduced hospital lengths of stay (Chan, Chiu, Chen, Lin, & Chu, 2005) Mount Sinai Medical Center (New York) Savings of $75,000 by switching from IV to oral antibiotics (DuPree et al., 2009) Froedtert Hospital (Milwaukee, WI) Increase in revenue of $1.2 million by improving commu- nication and documentation of radiology reports (Gor- man, Donnell, Hepp, & Mack, 2007) fin81226_07_c07_177-222.indd 186 10/30/14 7:26 PM Section 7.2 Six Sigma Quality Improvement In healthcare, where organizations are always trying to save money while at the same time improving patient care, managers who can show a potential savings from implementing a new project are more likely to receive approval from top leaders. However, healthcare orga- nizations are not only focused on quality improvements that can save them money. Their rev- enues, or earnings, may be directly tied to quality