Case 1
Case 1
25 year old female
25 year old female
3 month history of B-symptoms, progressive
3 month history of B-symptoms, progressive
anemia (normocytic), new adenopathy – not
anemia (normocytic), new adenopathy – not
painful but progressive over weeks, weight loss
painful but progressive over weeks, weight loss
Physical exam – diffuse adenopathy 2-3 cm in
Physical exam – diffuse adenopathy 2-3 cm in
size, oral ulceration - ?HSV, no organomegaly
size, oral ulceration - ?HSV, no organomegaly
Laboratory Investigations – Hemoglobin 60,
Laboratory Investigations – Hemoglobin 60,
MCV of 80, low WBC, normal platelet count,
MCV of 80, low WBC, normal platelet count,
normal biochemistry – high LDH
normal biochemistry – high LDH
3.
Case 2
Case 2
83 yo Female
83 yo Female
Otherwise healthy
Otherwise healthy
5 years ago presented with painful right submandicular
5 years ago presented with painful right submandicular
node – 3X3 cm – given ABx and followed for a few
node – 3X3 cm – given ABx and followed for a few
months – slight decrease
months – slight decrease
FNA done – reactive
FNA done – reactive
Node persisted over months – excisional biopsy –
Node persisted over months – excisional biopsy –
reactive adenopathy
reactive adenopathy
6 months ago – recurrent right submandicular node –
6 months ago – recurrent right submandicular node –
matted, slowly increased in size – now 3X3cm
matted, slowly increased in size – now 3X3cm
4.
Objectives
Objectives
Approach toAdenopathy
Approach to Adenopathy
Who to investigate
Who to investigate
When to investigate
When to investigate
How to define risk for underlying malignancy
How to define risk for underlying malignancy
6.
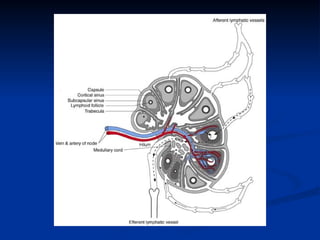
Lymph Nodes
Lymph Nodes
Anatomy
Anatomy
Collection of lymphoid cells attached to both vascular and
Collection of lymphoid cells attached to both vascular and
lymphatic systems
lymphatic systems
Over 600 lymph nodes in the body
Over 600 lymph nodes in the body
Function
Function
To provide optimal sites for the concentration of free or cell-
To provide optimal sites for the concentration of free or cell-
associated antigens and recirculating lymphocytes –
associated antigens and recirculating lymphocytes –
“sensitization of the immune response”
“sensitization of the immune response”
To allow contact between B-cells, T-cells and macrophages
To allow contact between B-cells, T-cells and macrophages
Lymphadenopathy - node greater than 1cm in size
Lymphadenopathy - node greater than 1cm in size
7.
Why do lymphnodes enlarge?
Why do lymph nodes enlarge?
Increase in the number of benign lymphocytes
Increase in the number of benign lymphocytes
and macrophages in response to antigens
and macrophages in response to antigens
Infiltration of inflammatory cells in infection
Infiltration of inflammatory cells in infection
(lymphadenitis)
(lymphadenitis)
In situ proliferation of malignant lymphocytes or
In situ proliferation of malignant lymphocytes or
macrophages
macrophages
Infiltration by metastatic malignant cells
Infiltration by metastatic malignant cells
Infiltration of lymph nodes by metabolite laden
Infiltration of lymph nodes by metabolite laden
macrophages (lipid storage diseases)
macrophages (lipid storage diseases)
8.
Epidemiology
Epidemiology
0.6% annualincidence of unexplained
0.6% annual incidence of unexplained
adenopathy in the general population
adenopathy in the general population
10% were referred to a subspecialist and 3.2 %
10% were referred to a subspecialist and 3.2 %
required a biopsy and 1.1% had a malignancy
required a biopsy and 1.1% had a malignancy
9.
When to worry?
Whento worry?
Age
Age
Characteristics of the node
Characteristics of the node
Location of the node
Location of the node
Clinical setting associated with
Clinical setting associated with
lymphadenopathy
lymphadenopathy
10.
Age
Age
Children/young adults– more likely to respond
Children/young adults – more likely to respond
to minor stimuli with lymphoid hyperplasia
to minor stimuli with lymphoid hyperplasia
Lymph nodes in patients less than the age of 30 are
Lymph nodes in patients less than the age of 30 are
clinically benign in 80% of cases whereas in patients
clinically benign in 80% of cases whereas in patients
over the age of 50 only 40% are benign
over the age of 50 only 40% are benign
Biopsies done in patients less than 25 yrs have a
Biopsies done in patients less than 25 yrs have a
incidence of malignancy of <20% vs the over-50 age
incidence of malignancy of <20% vs the over-50 age
group has an incidence of malignancy of 55-80%
group has an incidence of malignancy of 55-80%
11.
Characteristics of thenode
Characteristics of the node
Nodes lasting less than 2 weeks or greater than
Nodes lasting less than 2 weeks or greater than
one year with no progression of size have a low
one year with no progression of size have a low
likelihood of being neoplastic – excludes low
likelihood of being neoplastic – excludes low
grade lymphoma
grade lymphoma
Cervical nodes – up to 56% of young adults
Cervical nodes – up to 56% of young adults
have adenopathy on clinical exam
have adenopathy on clinical exam
Inguinal adenopathy is common – up to 1-2 cm
Inguinal adenopathy is common – up to 1-2 cm
in size and often benign reactive nodes
in size and often benign reactive nodes
12.
Characteristics of thenode
Characteristics of the node
Consistency – Hard/Firm vs Soft/Shotty; Fluctuant
Consistency – Hard/Firm vs Soft/Shotty; Fluctuant
Mobile vs Fixed/Matted
Mobile vs Fixed/Matted
Tender vs Painless
Tender vs Painless
Clearly demarcated
Clearly demarcated
Size
Size
When to worry – 1.5-2cm in size
When to worry – 1.5-2cm in size
Epitroclear nodes over 0.5cm; Inguinal over 1.5cm
Epitroclear nodes over 0.5cm; Inguinal over 1.5cm
Duration and Rate of Growth
Duration and Rate of Growth
13.
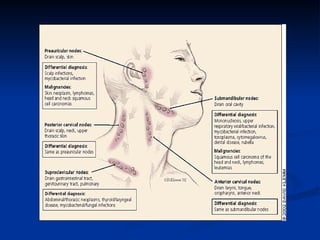
Location of thenode
Location of the node
Supraclavicular lymphadenopathy
Supraclavicular lymphadenopathy
Highest risk of malignancy – estimated as 90% in
Highest risk of malignancy – estimated as 90% in
patients older than 40 years vs 25% in those younger
patients older than 40 years vs 25% in those younger
than 40 yrs
than 40 yrs
Right sided node – cancer in mediastinum, lungs,
Right sided node – cancer in mediastinum, lungs,
esophagus
esophagus
Left sided node (Virchow’s) – testes, ovaries,
Left sided node (Virchow’s) – testes, ovaries,
kidneys, pancreas, stomach, gallbladder or prostate
kidneys, pancreas, stomach, gallbladder or prostate
Paraumbilical node (Sister Joseph’s)
Paraumbilical node (Sister Joseph’s)
Abdominal or pelvic neoplasm
Abdominal or pelvic neoplasm
14.
Location of thenode
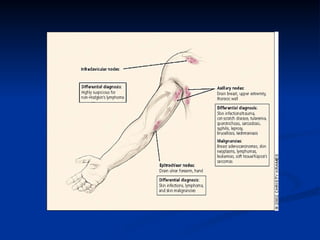
Location of the node
Epitroclear nodes
Epitroclear nodes
Unlikely to be reactive
Unlikely to be reactive
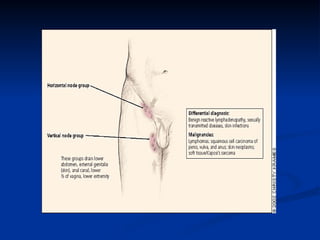
Isolated inguinal adenopathy
Isolated inguinal adenopathy
Less likely to be associated with malignancy
Less likely to be associated with malignancy
15.
Clinical Setting
Clinical Setting
B symptoms – fever, night sweats, weight loss
B symptoms – fever, night sweats, weight loss
Fatigue
Fatigue
Pruritis
Pruritis
Evidence of other medical conditions –
Evidence of other medical conditions –
connective tissue disease
connective tissue disease
Young patient – mononucleosis type of
Young patient – mononucleosis type of
syndrome
syndrome
16.
History
History
Identifiable causefor the lymphadenopathy?
Identifiable cause for the lymphadenopathy?
Localizing symptoms or signs to suggest
Localizing symptoms or signs to suggest
infection/neoplasm/trauma at a particular site
infection/neoplasm/trauma at a particular site
URTI, pharyngitis, periodontal disease, conjunctivitis, insect bites,
URTI, pharyngitis, periodontal disease, conjunctivitis, insect bites,
recent immunization etc
recent immunization etc
Constitutional symptoms
Constitutional symptoms
Epidemiological clues
Epidemiological clues
Occupational exposures, recent travel, high-risk behaviour
Occupational exposures, recent travel, high-risk behaviour
Medications – serum-sickness syndrome
Medications – serum-sickness syndrome
17.
Physical Exam
Physical Exam
Full nodal examination – nodal characteristics
Full nodal examination – nodal characteristics
Organomegaly
Organomegaly
Localized – examine area drained by the nodes
Localized – examine area drained by the nodes
for evidence of infection, skin lesions or
for evidence of infection, skin lesions or
tumours
tumours
18.
Approach to Lymphadenopathy
Approachto Lymphadenopathy
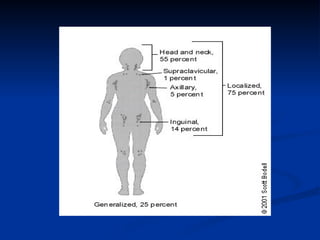
Localized – one area involved
Localized – one area involved
Generalized – two or more non-contiguous
Generalized – two or more non-contiguous
areas
areas
Management
Management
Identify underlyingcause and treat as
Identify underlying cause and treat as
appropriate – confirmatory tests
appropriate – confirmatory tests
Generalized adenopathy – usually has
Generalized adenopathy – usually has
identifiable cause
identifiable cause
Localized adenopathy
Localized adenopathy
3-4 week observation period for resolution if not
3-4 week observation period for resolution if not
high clinical suspicion for malignancy
high clinical suspicion for malignancy
Biopsy if risk for malignancy - excisional
Biopsy if risk for malignancy - excisional
26.
Fine Needle Aspirate
FineNeedle Aspirate
Convenient, less invasive, quicker turn-around
Convenient, less invasive, quicker turn-around
time
time
Most patients with a benign diagnosis on FNA
Most patients with a benign diagnosis on FNA
biopsy do not undergo a surgical biopsy
biopsy do not undergo a surgical biopsy
27.
Conclusions
Conclusions
Lymphadenopathy –initial presenting symptom
Lymphadenopathy – initial presenting symptom
Reactive vs Malignant
Reactive vs Malignant
Probability
Probability
History
History
Physical Exam
Physical Exam
Biopsy if not resolved in 3-4 weeks for low risk
Biopsy if not resolved in 3-4 weeks for low risk
patients
patients
Biopsy all high risk patients – excisional biopsy
Biopsy all high risk patients – excisional biopsy
































![pt with inguinoscrotal swellings[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ptwithinguinoscrotalswellings1-250602050940-2dde0455-thumbnail.jpg?width=640&height=640&fit=bounds)
























