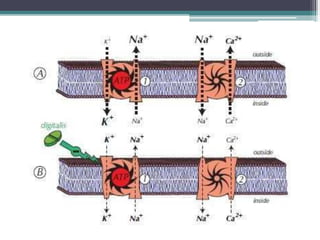
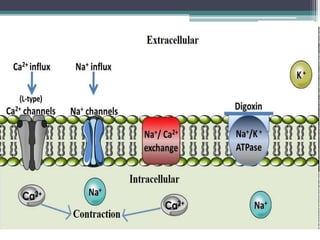
This document discusses cardiotonic drugs, which increase the contractility of the cardiac muscle without increasing oxygen demand. It focuses on two main types - cardiac glycosides like digoxin, and phosphodiesterase inhibitors. Digoxin increases calcium levels in cardiac cells, strengthening contractions. It has a positive inotropic effect and is used to treat heart failure and arrhythmias. The document outlines the mechanisms, effects, dosing, interactions, toxicity and nursing considerations for digoxin and phosphodiesterase inhibitors.




































![제 23회 보아즈(BOAZ) 빅데이터 컨퍼런스 - [MBOAX] : ABSA를 활용한 소비자 반응 분석 기반 운영 효율화 대시보드 설계](https://cdn.slidesharecdn.com/ss_thumbnails/3-1boaz23rdconferencemboax-260203102709-9d519923-thumbnail.jpg?width=640&height=640&fit=bounds)















