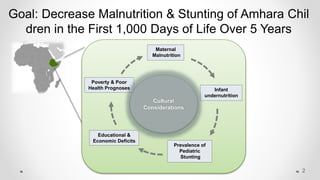
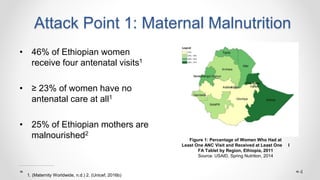
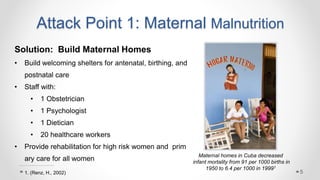
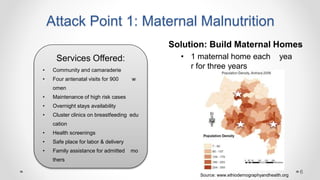
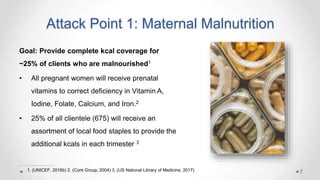
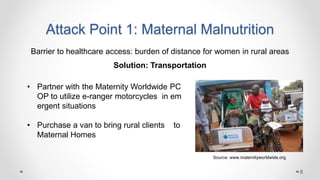
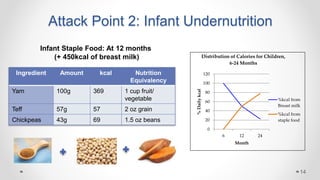
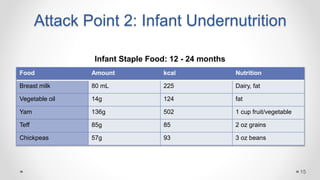
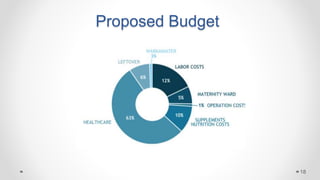
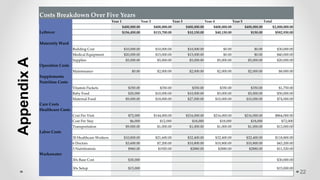
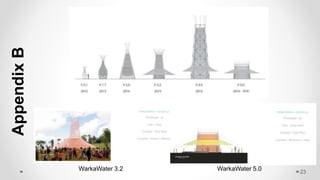
This document proposes a community-based solution to reduce stunting and malnutrition in Amhara children in Ethiopia over 5 years. It identifies key issues like maternal malnutrition, infant undernutrition, and lack of clean water. The solution has three main attack points: 1) building maternal homes to address maternal malnutrition, 2) developing an infant staple food to combat undernutrition from 6-24 months, and 3) installing WarkaWater devices for a sustainable source of clean water. The budget outlines costs of $2 million over 5 years to implement maternal homes, supplements, transportation, healthcare workers, and Warkawater devices. The expectation is this comprehensive approach will decrease disease and malnutrition while increasing health awareness.