Downloaded 20 times

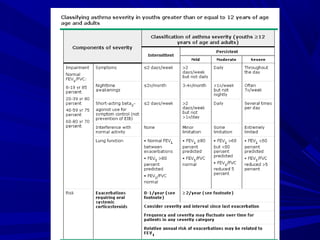
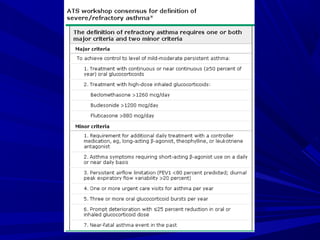
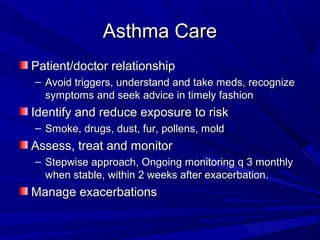
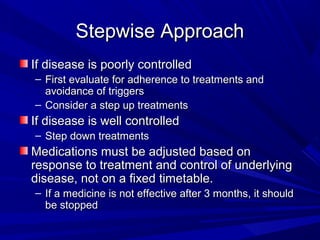
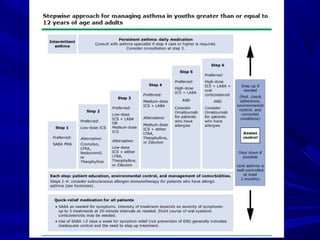
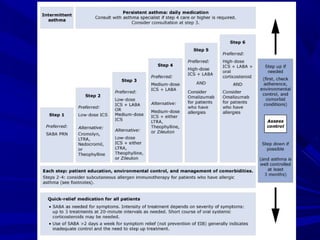
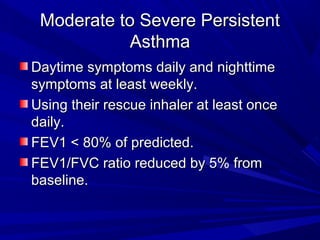



This document summarizes guidelines for diagnosing and managing asthma from the American Thoracic Society, National Asthma Education and Prevention Program, and Global Initiative for Asthma. It outlines defining features of asthma including airway inflammation and obstruction. Diagnosis involves assessing symptoms, lung function testing, and ruling out other causes. Goals of treatment are avoiding symptoms, limiting reliever medication use, and normal lung function through a stepwise treatment approach tailored to asthma severity and level of control.



























![Alibabyte presentazione seminario - parte i - [matteo]](https://cdn.slidesharecdn.com/ss_thumbnails/alibabyte-presentazioneseminario-partei-matteo-130630130105-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















