Download as PDF, PPTX
![Age-adjusted RR for Spine and Hip-Fracture
in Relation to endogenous Serum E2-Levels
1,00
Hip-Fracture Spine-Fracture
1.0 1.0
0,75 Independent of BMD
Relative Risk
0,50 0.5 0.5
0.4 0.4
0.3 0.3
0,25
0,00
<5 5-6 7-9 >9
Endogenous Serum Estradiol Level [pg/ml]
Cummings et al. (1998); NEJM Vol 339 No 11, 733-740](https://image.slidesharecdn.com/200901291336190-osteoearlymenopause-100503064024-phpapp01/85/Prevention-of-Osteoporosis-in-early-menopause-17-320.jpg)

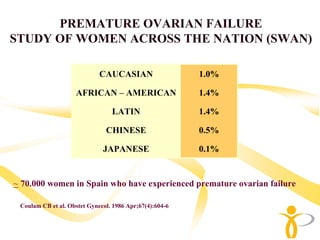
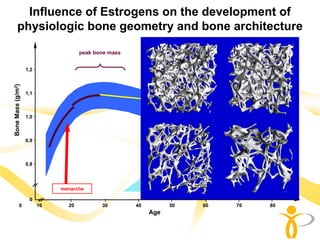
This document discusses prevention of osteoporosis in early menopause. It begins with definitions of early menopause including bilateral oophorectomy and premature ovarian failure. It then discusses the effects of estrogen deficiency on bone loss and how early menopause can negatively impact bone mineral density. The document notes that early menopause is associated with increased risk of fractures compared to natural menopause. Finally, it discusses approaches for preventing osteoporosis in women experiencing early menopause.




























![Osteoporosis%203rd%20yr[1]](https://cdn.slidesharecdn.com/ss_thumbnails/osteoporosis203rd20yr1-111103005118-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































