INTRODUCTION
• Advancement intechnology allow for testing
on an impressively wide variety of specimen
collected from the human body.
• Proper specimen collection and handling is
an integral part of obtaining a valid and
timely laboratory test result.
• Error is the discrepancy between the result
obtained in the testing process and its ‘True
Value’
3.
-communicating them tothe
clinicians in a number of
ways (in particular, by producing a
report and making
any necessary oral
communications regarding ‘‘alert’’
or panic results).
-In this step, the most common
mistakes
4.
Outline
• Introduction
• Specimencollection
– Types of Specimen
– Identification of Patient
– Obtaining Specimen
• Sources of Error
– Pre analytical
– Analytical
– Post analytical
• Summary
• Conclusion
5.
SPECIMEN:
• the substancecollected from a patient for
analysis in the laboratory which maybe
subjected to pre analytic treatment to obtain
a part of it that would eventually be
analysed.
SAMPLE
• This is that part of a specimen that is
eventually subjected to analysis in the
laboratory.
6.
Types of Specimen:
•Whole blood,
• Serum,
• Plasma,
• Urine,
• Feces,
• Saliva,
• Body fluids- Cerebrospinal ,Synovial,Amniotic,
pleural, pericardial and ascitic ,
• Solid tissues- hair,nails
• Specific cell types
• Sweat
7.
Patient Identification
• Allpatients from whom clinical specimens are obtained
must be positively identified prior to specimen collection.
• Positive identification is the responsibility of the person
collecting the specimen.
• A request form duly filled by the requesting doctor providing:
– Hospital number, Surname and first names, Age, Sex,
Nationality, Race/tribe, Ward/clinic
• Hospital inpatients should be wearing an identification
band with the above information,
– Clinical, Summary/Diagnosis.
– the nature of specimen, the type of test and
– the requesting doctor’s and consultant’s names,
signature and phone number.
8.
• At leasttwo patient identifiers are used:
• Inpatients:
– wear an identification bracelet that includes their
last and first name, date of birth and a unique
hospital number.
– Proper identification should include a three-way
match using information on the ID bracelet and
the test requisition, and the patient's stating of
his or her name.
– For unconscious or unidentified patients, it is
important a unique number or identification
system be used.
9.
• Outpatients:
– thereis no ID bracelet, but the patient should
have been given identification labels when
he/she registered.
– This label can be used along with asking the
patient his/her name. If there is no label, then
another means of identification should be used.
• DO NOT collect any specimen unless at least two
positive identifications can be made.
• In case of a paediatric patient, the parent or
guardian should be present and provide active
identification of the child.
10.
Patient Preparation
• Thetiming of the specimen collection should
be determined:
– Fasting
– Random
– Timed-interval
– 24 hour collection
• Identification of appropriate specimen
containers
• Pre-labelling of containers
• Assumption of proper position.
• Personnel should be properly dressed-PPE
11.
BLOOD
• One ofthe body tissues.
• Can be obtained from:
– veins,
– arteries and
– Capillaries
• Method of Collection
– Venipuncture: obtaining blood sample from the
veins. Preferred method as venous blood is usually
the sample of choice.
– Skin puncture: mainly for children and point-of-
care testing. Capillary blood is obtained mainly.
– Arterial puncture: mainly for blood gases
analysis. Requires skills.
12.
Venipuncture
• Defined asall of the steps involved in
obtaining an appropriate identified
blood specimen from a patient.
Preliminary steps
• POSITION
– Sitting or supine but must be in this
position for atleast 20 minutes.
– The patient’s arm should be
extended in a straight line from
shoulder to wrist.
13.
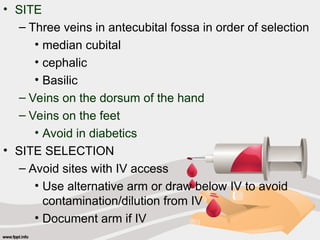
• SITE
– Threeveins in antecubital fossa in order of selection
• median cubital
• cephalic
• Basilic
– Veins on the dorsum of the hand
– Veins on the feet
• Avoid in diabetics
• SITE SELECTION
– Avoid sites with IV access
• Use alternative arm or draw below IV to avoid
contamination/dilution from IV
• Document arm if IV
14.
– Mastectomy—avoid sitedue to lymphostasis
• Infection risk/alteration in body fluids and
blood analytes
– Edematous areas —avoid due to accumulation
of body fluids
• Possible contamination/dilution of specimen
– Avoid arms with haematoma and extensive
scarring
• Phlebotomist must estimate the blood volume
required.
• Must also choose the appropriate needle guage.
15.
Site Preparation
• Priorto venipuncture, the site should be cleansed
with alcohol.
• Cleansing starts at the center of the vein, and
should continue outward in concentric circles.
• The alcohol should be allowed to air dry.
– If not, Hemolysis can occur which may result in
the spurious elevation of such analytes as
potassium, lactate dehydrogenase (LD), iron
and magnesium
• For ethanol, benzalkonium chloride solution should
be used.
• Povidone Iodine should be avoided as it interfers
with most analytes.
16.
Tourniquet Application andTime:
• The tourniquet should be applied approximately 3-
4 inches above the venipuncture site.
• The tourniquet should not be on the arm longer
than one minute.
– A good rule of thumb to determine the one-
minute tourniquet time is to remove the
tourniquet when blood starts to flow into the first
tube of blood being drawn.
– Prolonged tourniquet time can lead to an
increase in various chemistry analytes, including
serum protein, potassium and lactic acid due to
hemoconcentration of blood at the puncture site.
17.
• The compositionof the blood drawn first is most
representative of the composition of circulating
blood.
• Pumping of the fist before venipuncture increases
plasma potassium, phosphate and lactate
concentrations.
• The lowering of blood pH due to lactate causes
ionized calcium to increase.
18.
• Correct collectionsystem
– Evacuated tube system (Vacutainer) for large veins in
antecubital fossa
– Syringe for small, fragile veins or veins outside
antecubital fossa
• Venous access
– Needle entry should be at 15 to 30 degrees depending
on depth of vein
– Needle entry should be in same direction as vein,
centered over vein
– Anchor vein to prevent movement during needle entry
and to reduce pain to patient
19.
Evacuated Tubes
• Needleis screwed into the holder
• Tap the tube gently to dislodge any additive from the
stopper
• Insert the tube onto the holder
• Clean the skin and apply tourniquet
• Guide the needle into the vein, press the tube forwrd
to puncture the stopper and release vacuum
• Fill the tube until the vacuum is exhausted
• Withdraw the tube from the holder
• Replace another tube if necessary
Syringes
• The needleis placed over the nozzle of the syringe
and the cover of the needle is removed.
• After piercing the skin and the vein, the blood is
withdrawn by gently pulling back on the plunger.
• Blood should quickly transferred by gentle ejection
into specimen bottles prepared for its receipts or
promptly analyzed in case of blood gases.
• The bottles or tubes capped and gently mixed
• Haemolysis is less if small bore needle is used
since turbulence is less.
22.
Order of Draw
•Following the correct order of draw during venipuncture is
critical to ensure accurate test results.
• There are established recommendations for the proper
order of draw for evacuated blood collection tubes
– Non additive tubes
– Coagulation or citrate containing tube
– Serum separator tube containing gel
– Heparin containing tube
– EDTA containing tube
– Oxalate-flouride containing tube
• Order of draw affects the quality of the sample and can lead
to erroneous test results due to contamination with the
additive from the previous blood collection tube
23.
Completion of Collection
•Withdraw the needle
• Place a dry gauze over the puncture site with the
arm raised to reduce bleeding.
• With the evacuated tubes, the needle is covered
and the needle and the tube holder are
immediately discarded into a sharp container.
• All tubes or specimen bottles are labeled. The rate
of time of collection should be included.
• Gloves are discarded, hands washed with soap
and water before proceeding to the next patient.
24.
Venipuncture in children
•The technique in adults and children are similar.
However, children are likely to make unexpected
movements, assistance in holding them still is often
desirable.
• Either a syringe or evacuated blood tube system
may be used.
• A 21-23 gauge needle or 20-23 gauge butterfly
needle with attached tubing may be used.
25.
Skin Puncture
• Anopen collection technique in which the skin is
punctured by a lancet and a small volume of blood
collected into a microdevice- capillary tube
• Indications:
– Sample volume is limited e.g. children
– Repeated venipuncture have resulted in severe pain.
– Extensive burns or bandaging where veins are
unavailable.
– Sample to be applied directly to a testing device in a
point-of-care testing situation or to filter paper.
26.
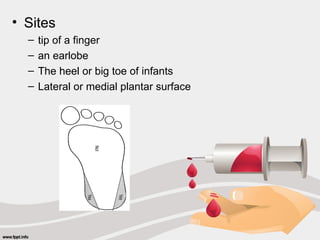
• Sites
– tipof a finger
– an earlobe
– The heel or big toe of infants
– Lateral or medial plantar surface
27.
PROCEDURE
• Pre warmif necessary with a slightly warm cloth
• Clean the skin over the area to be used, allow to
dry
• Quickly puncture with a sharp stab with lancet
• Depth should be <2.5mm to avoid contact with
bone
• Hold the area downward to collect blood by gravity
• First drop should be wiped off
• Transfer to appropriate capillary tube/card
• Do not massage the finger- causes outflow of
tissue fluid and debris
28.
Arterial Puncture
• Onlyperformed by a physician or specially trained
technicians or nurses with required skill.
• Arterial samples are used for blood gas analysis.
The preferred sites are:
• Radial artery at the wrist
• Brachial artery in the elbow
• Femoral artery in the groin.
– The arm is the preferred sites for the elderly due to
leakage of blood from the femoral artery.
29.
Blood Gas Analysis
•Glass syringes
– Evacuated tubes should not be used due to residual air
• Needle and syringe flushed with heparin solution to ensure
adequate anticoagulation
• Eliminate trapped in the needle and in the dead space of
the nozzle
• Apply pressure after sample is drawn
• Seal the nozzle, place syringe in a plastic bag and place in
melting ice
– Inhibits metabolic activity of the white cells
– Prevents change in pH
– Prevents expansion of gases
• Transport immediately to the lab
• Analysis shoould be performed immediately
30.
Factors Affecting BloodCollection
• Anticoagulant and preservatives
• Type of sample- fasting
• Sites of collection
• Collection from intravenous and arterial lines.
• Heamolysis
• Posture-conc of plasma protein low in supine.
• medication
Anticoagulants and Preservatives
• Heparin
– available as Na, K, NH4, Li and widely used.
– activates antithrombin III which then forms complexes with
activated coagulation factors
– 20 units to 1 ml of blood
31.
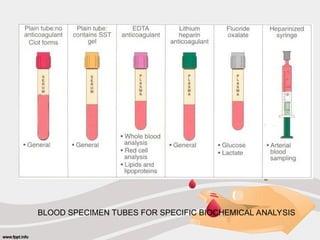
EDTA
• Chelating agent-binds Ca+ hence prevents clotting
• Preserves cellular components of blood
• Unsuitable for ALP, Ca and Iron assay
FLOURIDE OXALATE
• For blood glucose analysis
• Inhibits glycolysis- flouride inhibits enolase
• Oxalate forms insoluble complexes with Ca ions
Others e.g. Acid-citrate dextrose (ACD) used to
isolate genomic DNA, sodium citrate, sodium
iodoacetate etc.
32.
Site of collection
•Blood obtained from different sites differs in composition
• Skin puncture blood is more like arterial blood than venous
blood.
• Capillary and arterial blood in are similar pH, PCO2, PO2
and oxygen saturation while PCO2 of venous blood is up to
6 to 7mmHg more.
• Venous blood glucose is much as (0.39mmol/L) less than
the capillary blood glucose due to tissue metabolism.
• Skin puncture blood is contaminated with interstitial and
intracellular fluids resulting in increased glucose and
potassium and decrease bilirubin, calcium, sodium and total
protein compared to venous blood.
33.
Collection from IVLines
• Direct from IV line shows increased analytes in the infusion.
• Shut off fluid with the stop cock
• Withdraw and discard about 10 ml of blood before taking
specimen for analysis
• Draw from the vein below the IV line
Haemolysis
• This causes dilutional effect on those constituents present at
lower concentration in the erythrocytes than in plasma.
• But causes those constituents at higher concentration in
erythrocytes e.g. LD, Potassium, magnesium and phosphate to
Saturate Plasma causing an increase in concentration as well in
plasma
•
34.
Criteria for rejectionof specimens
Criteria for rejection of specimens
oMissing or inadequate identification
Missing or inadequate identification
oInsufficient volume
Insufficient volume
oSpecimen collected in wrong collection tube
Specimen collected in wrong collection tube
oContamination
Contamination
oInappropriate transport and storage
Inappropriate transport and storage
oUnknown time delay
Unknown time delay
35.
URINE
• Urine isan excretory product of the body and
presence of certain substances in the urine
reflects the metabolic state of the body.
• It can be easily collected and examined,
• The type of urine specimen to be collected is
determined by the test to be performed
36.
Types of urinespecimen and mode of collection.
• Untimed or random specimen
– A single collection of urine any time, day or night in a clean,
dtergent free container.
– suitable for only a few clinical test e.g. fractional excretion of
sodium to distinguish between prerenal from intrinsic renal failure
etc.
• Fasting or early morning urine
– Empty bladder before retiring at night, discard.
– Collect the morning specimen on rising.
– used to determine urine pH, osmolality, specific gravity, proteins
and Hcg
• Double-void urine
– Urine excreted during a timed period after a complete emptying of
the bladder
– used to assess glucose excretion during a glucose tolerance test.
It must be timed in relation to the ingestion of glucose.
37.
• Timed urinespecimen
– collected a specific period of time e.g. 1, 4 or 24 hours.
Example is a quantitation of proteinuria in urine.
– 24 HOUR URINE SPECIMEN
• Empty the bladder and discard
• Collect for the next 24 hours including specimen at the
24th
hour
• Specimen passed during defeacation must be added
• Preserve with 5 ml of 10% thymol in Propanol
• Keep specimen in refrigerator during collection
• clean-catch specimen (MSU) for bacterial culture
– Clean the urethral orifice
– Pass the first stream of urine to clean the passage
– Collect the next stream in a clean in sterile container
– Continue voiding
38.
• Catheter specimen
•Suprapubic specimen
– especially for infant
– Clean the skin over the full bladder
– Apply local anaesthetic
– Pass a 22 gauge needle through the skin
– Penetrate the bladder and withdraw urine into the
syringe
• Urine collected from children
– To collect an untimed specimen from a child, the penis
and scrotal or perined area is first cleaned and dried to
remove natural or applied oils.
– A plastic bag e.g. U-bag is then applied around the infant
genitalia and left in place until a urine has been voided.
39.
Urine preservatives
• Reducebacterial action
• Reduce chemical decomposition
• Solubulise constituents that might otherwise
precipitate
• Decrease atmospheric oxidation of unstable
compounds
TYPES
• The most satisfactory form of preservation is
refrigeration at 40
C combined with chemical
preservation.
• Formalin, HCl, Boric Acid, Thymol,
40.
Faeces
• Small aliquotscan be analysed for occult blood
• Patient is encouraged to put a small part of
excreted faeces into d specimen bottle or apply
directly to the reagent impregnated slide for
analysis.
• No preservative added
• Chemical test carried out on faecal specimen are
for blood, abnormal quantities of fat or increased
protein content
41.
Cerebrospinal fluid
• Itis obtained by a lumbar puncture by a physician in the
lumbar region.
• The first few drops of the fluid are discarded and the rest of
the fluid is collected in sterile containers.
• During the lumbar puncture, the first specimen should be
used for chemical analysis while the 2nd is used for
microbiological analysis.
• Sample for CSF glucose may be collected in a plain
container if analysis is to be carried out rapidly or in a
flouride oxalate bottle
• Blood sample should be drawn 30-60 mins before collection
for comparison
• Specimen for protein and other analytes are taken in a plain
bottle
42.
Synovial Fluid
• Fluidfound in the joint cavity, bursae and tendon
sheaths
• It is a dialysate of plasma mixed with Hyaluronic acid
Arthrocentesis- sterile aspiration of synovial fluid
• Performed by a physician or surgeon
– The skin over the site is decontaminated
– Local anaesthetic is used
– The fluid is aspirated with a sterile syringe
– Do not add acetic acid any other fluid , may precipitate the
synovial protein
– EDTA may be used for TWBC and differential,
– Sterile plain tubes for glucose and protein measurement
43.
Pleural / Pericardialand Ascitic fulid
This fluids lubricates the opposing parietal and
visceral membrane surfaces
Diagnostic Paracentesis: the aspiration of any of
these fluid for laboratory analysis
• Decontaminate the skin
• Aspirate fuild with sterile needle
• Assay for protein, RBCs, enzymes, TGs in Chylous
ascites
44.
Amniotic fluid
Amniocentesis procedurefor collecting amniotic fluid
• Performed by an obstetrician
Indications
• Prenatal diagnosis of congenital disorders.
• To assess fetal maturity
• Rhesus isoimmunization
• intrauterine infection.
• Fetal lung maturity (lecithin/splingovalion, Albumin/surfactant).
Procedure
• The skin is first cleaned and anaesthetized
• 10ml of fluid is aspirated into a syringe under USS guidance
• Sterile containers are used to transport the fluid to the laboratory.
• If the lecithium-sphingomylin (L/S) ration or an albumen to surfactant
ratio is to be determined, the specimen is immediately placed on ice in
its container.
• If bilirubin is to be assayed, the specimen should be transferred to a
brown tube or bottle or wrapped in aluminum foil to avoid
photodegradation.
45.
Saliva
• Used tomeasure blood group substances to
determine secretor status and genotype and most
recently to detect presence of anti-HIV antibodies.
• This is produce by asking a patient to chew an inert
material such as a piece of rubber after rinsing his
or her mouth. The first mouthful of saliva is
discarded and the next is collected into a glass
bottle.
• A dental cotton can be chewed by a patient, saliva
is extracted from the soaked cotton by
centrifugation while placed in a plastic tube
46.
Solid Tissue
• Malignanttissue from the breast is a tissue that is
analyzed for estrogen and progesterome receptors.
• Breast tissue is trimmed of fat and non tumour
material and frozen within 20 minutes in liquid
nitrogen or in a mixture of dry ice or alcohol.
• The tissue is then examined to confirm that it is
malignant and finally processed to determine
estrogen and progesterone receptors.
• Toxicological and trace element determinations
can also be carried out on the tissue.
47.
Hair and Nails
•Used for trace metal analysis
• Collection procedure is poorly standardized and
measurements are better obtained on blood or
urine.
It is limited to forensic analysis.
Sweat
• Used to determine the chloride level in cystic
fibrosis
• Also used in drug abuse detection.
• Production is by stimulation with pilocarpine intake.
48.
Specific Cells
Buccal cellsare used to provide an excellent source of
genomic DNA.
– The patient is provided with a mouthwash and instructed
to rinse and then mouthwash to a collection tube.
– A swab is used to collect the buccal cells.
• After collection, the swab is stored in a plastic container or
immersed in phosphate – buffered saline.
chorionic villous sampling to know the genetic disorders
present in a fetus in utero.
• It involves insertion of a needle into the placenta and
removing some of the chorionic villi.
– Can be done between 10 to 12 weeks. Whereas with an
amniotic fluid sample, testing cannot be performed until
week 15 or 20 of gestation.
49.
HANDLING OF SPECIMENSFOR ANALYSIS
Maintenance of Specimen Identification
• Proper identification of specimen must be maintained at
each step of the testing process and every specimen
container adequately labeled.
Preservation of specimen in transit
• Specimen must be properly preserved both during its
transport to the laboratory.
• Specimens are kept at 40
C from the time of blood collection
until specimen are analyzed;
• Others require remaining at or near room temperature.
• Specimens that have analyte that are thermally labile
should be separated and refrigerated.
• Specimens for bilirubin must be protected from both daylight
and fluorescent light.
50.
SEPARATION AND STORAGESPECIMENS
• Plasma and serum should be separated within 2 hours.
• This will be stable at room temperature for eight hours, and
up to 48 hours at 2- 40
C
• After 48 hours, the serum specimen should be frozen at –
200
C in an aliquot tube.
• analytes that are stable for 24 hours, refrigerate at 40
C
• For hormone analysis, the plasma or serum should be
frozen immediately after centrifuging.
• Specimen tubes should be centrifuged with stoppers in
place to:
– Avoid aerosolization of infectious particles
– Maintain anaerobic conditions which is important in
measurement of carbon dioxide and ionized calcium
– Reduce evaporation e.g. ethanol.
51.
Transport To Lab:
•Prioritize sample for transport
• Send sample to lab
– Pneumatic tube: prone to haemolysis
– Robot
– Hand carry : In hospitals, messengers are used to
transport samples
– Courier
Receive In Lab:
• Accession
• Apply/ verify sample label
• Barcode for testing
• Identify STAT(special turn around time) tests
• Rack sample
52.
Prepare For Testing:
•Centrifuge
• Aliquot
• Pre-treat
• Re-rack
Transport To Sections
• Send sample to appropriate lab section
– Main lab
– Reference lab
– Re-rack
TYPES OF ERROR
•PRE-ANALYTICAL
• ANALYTICAL
• POST –ANALYTICAL
PRE-ANALYTICAL ERRORS
• This phase starts with test request,
• Patient and specimen identification,
• Blood drawing,
ANALYTICAL
In recent decades,
standardization,automation
and
technological advances
have significantly improved
the analytical reliability of
laboratory results and
decreased the error rates
57.
POST
• The post-analyticalprocedures performed
within the laboratory include
• verifying laboratory results
• Feeding them into the laboratory
information system
58.
• Errors canbe minimized by careful adherence to
robust, agreed protocols at every stage of the testing
process: this means a lot more than ensuring that the
analysis is performed correctly.
• Errors can occur at various stages in the process:
– pre-analytical- specimen collection, transport and
processing,
– analytical,- specimen analysis,
– post-analytical- testing results transmission,
interpretation, follow-up, retesting.
• Errors during the collection process are not inevitable
and can be prevented with a diligent application of
quality control, continuing education and effective
collection systems
59.
Collection Errors
• PatientIdentification
– Name
– Unlabelled specimen containers
– Containers labelled with the wrong patient’s name
Patient’s Controllable variables
• Physiological
– Posture
– Exercise/physical training
– Circadian variation
– Menstrual cycle
• Diet
• Lifestyle
– Smoking
– Alcohol
• Drugs
60.
Non controllable variables
•Biological
– Age
– Sex
– Race
• Environmental
– Geographical location
– Altitude
– Ambient temperature
– Seasonal influences
• Underlying medical conditions
– obesity, blindness, pregnancy, fever, shock and trauma
and infusions and transfusions.
61.
• Phlebotomy techniqueError
– Site Selection
– Cleansing of venipuncture site
– Tourniquet Application
– Correct collection system
• Order of Draw
• Improper collection tube drawn for test ordered
• Collection tube not completely filled
62.
• Blood SpecimenTransport Errors
– Transport of blood specimens in the proper
manner after collection ensures the quality of the
sample
– Timing
• Some specimens must be transported immediately
after collection, for example Arterial Blood Gases.
• Specimens for serum or plasma chemistry testing
should be centrifuged and separated within two hours
63.
• Temperature
– Specimensmust be transported at the
appropriate temperature for the required test
• On ice—ABGs, Ammonia
• Warmed --98.6 degrees (37 C), cryoglobulins
• Avoid temperature extremes if transported from via
vehicle from other collection site
• Transport Container
– Some samples need to be protected from light, for
example, bilirubin
– Transport in leak-proof plastic bags in lockable rigid
containers
64.
Sample Preparation Errors
•Sample preparation involves processing of the
sample prior to and in preparation for analysis.
• Processing involves centrifugation,
• and making an aliquot of the specimen in a
test tube or sample cup
• Keep in mind that clotted or whole blood cells can
affect chemicals in the sample over a period of
time, such that additional chemicals arise or some
chemicals are consumed
65.
Error Prevention
• Itis very difficult to establish effective methods
for monitoring and controlling preanalytical
variables because many of the variables are
outside the laboratory areas.
• Requires the coordinated effort of many
individuals and hospital departments
– The highest frequency of errors occurs with the
use of handwritten labels and request forms.
The use of bar code technology has significantly
reduced ID problems.
66.
– Training ofpersonnel for proper collection
and handling of samples, including adherence
to specific steps and maintaining turnaround
time involving sample reception and processing.
– Use of well-written procedures and policies
(SOP) can help to minimize preanalytical errors
(specimen collection manual)
67.
Conclusion
The Golden Ruleof Specimen Collection:
The Patient’s Test Result is Only as Good
as the Sample We Get.
Every effort should be made by all concerned
to ensure that the result is what it is
supposed to be. (ROLE OF THE
PHYSICIAN)