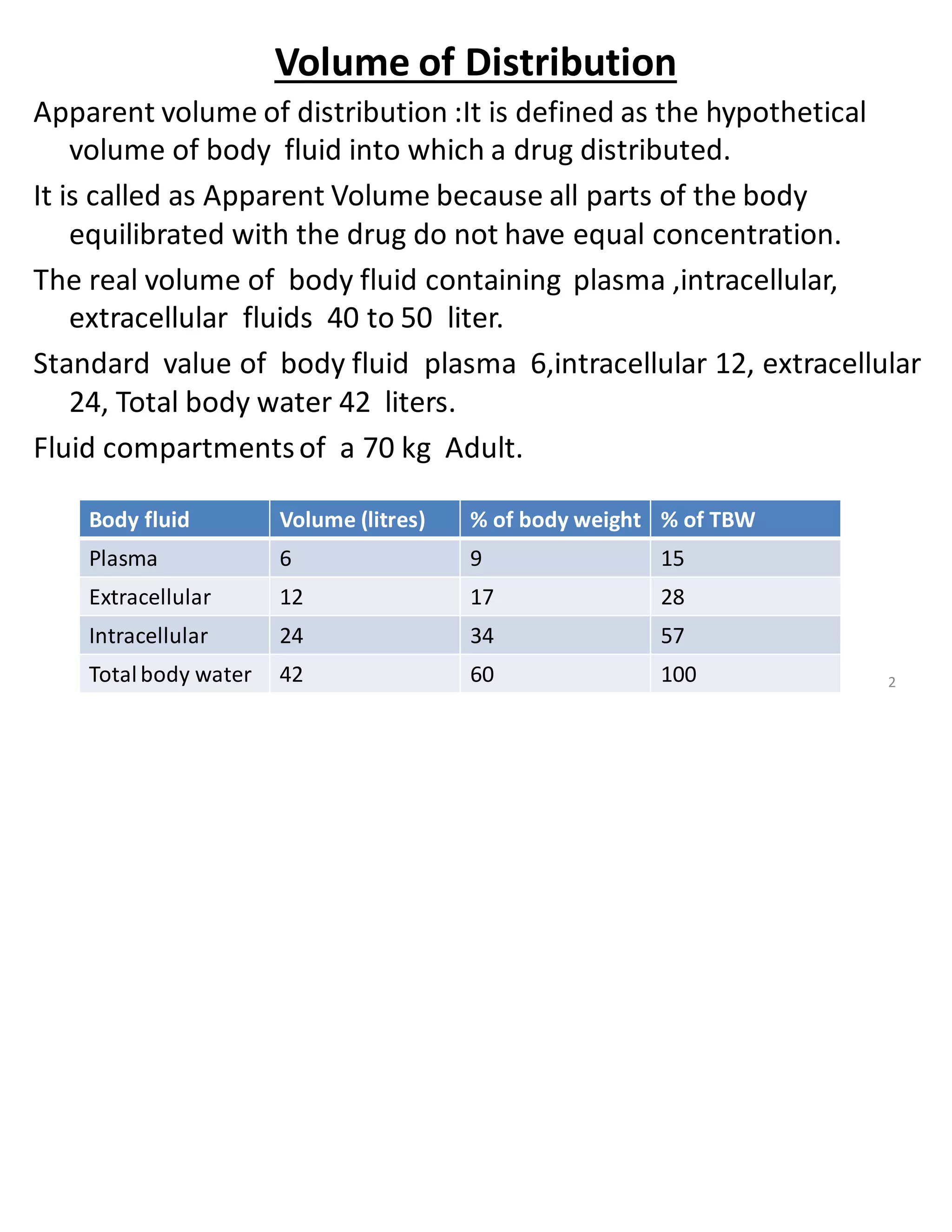
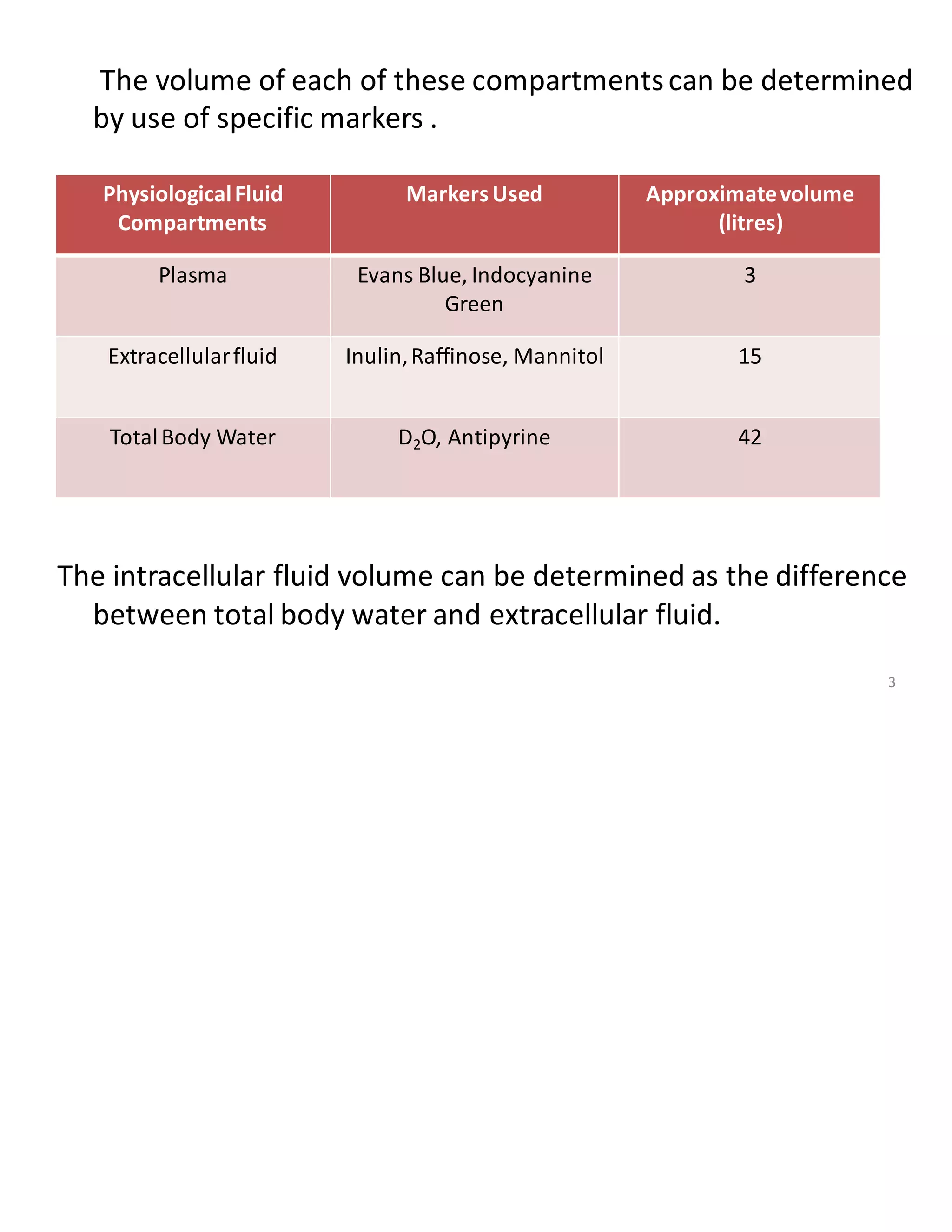



This document discusses drug distribution and protein binding. It provides details on: 1. The apparent volume of distribution, which is the hypothetical volume that a drug appears to be distributed in the body. Drugs that bind strongly to plasma proteins have a smaller apparent Vd, while those that bind strongly to tissues have a larger Vd. 2. The different fluid compartments in the body and markers used to determine their volumes. It also discusses factors that affect drug-protein binding such as drug properties, protein concentrations, and binding affinities. 3. The major plasma proteins that drugs bind to like human serum albumin, alpha-1-acid glycoprotein, and lipoproteins. It describes the





















































![Chapter 9 introduction to pharmacokinetic model [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter9finalforvideointroductiontopharmacokineticmodelcompatibilitymode-200527080141-thumbnail.jpg?width=640&height=640&fit=bounds)


























