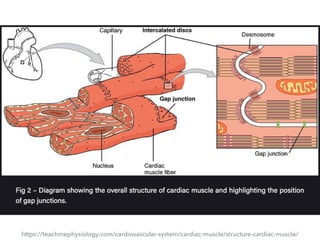
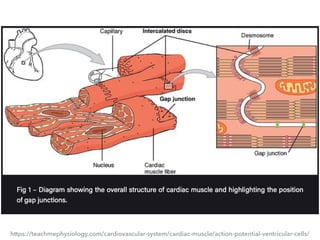
The document discusses the structure and physiology of cardiac muscle contraction. It describes how cardiac myocytes contract via calcium-induced calcium release from the sarcoplasmic reticulum through ryanodine receptors. When L-type calcium channels in the t-tubules open during an action potential, the calcium that enters activates nearby ryanodine receptors, causing a much larger release of calcium from internal stores. This calcium then binds to troponin C and initiates contraction through the sliding filament model. The sarcoplasmic reticulum calcium ATPase pump then removes calcium to allow muscle relaxation. The document also reviews the histological structure of cardiac muscle, including intercalated discs that electrically couple myocytes.