Nefropatía diabética. Nuevos aspectos
•
3 likes•802 views

Memorias Conferencia Científica Anual sobre Síndrome Metabólico 2017 - Programa Científico Nefropatía diabética. Nuevos aspectos Dr. Francisco Gómez Pérez Jefe del Departamento de Endocrinología y Nutrición, Instituto Nacional de Ciencias Médicas y Nutrición “Salvador Zubirán”

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Nefropatía diabética. Nuevos aspectos
Similar to Nefropatía diabética. Nuevos aspectos (20)
More from Conferencia Sindrome Metabolico
More from Conferencia Sindrome Metabolico (20)
Recently uploaded
Recently uploaded (20)
Nefropatía diabética. Nuevos aspectos
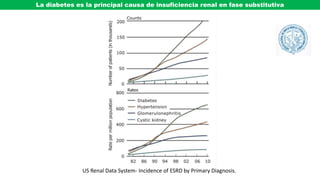
- 1. US Renal Data System- Incidence of ESRD by Primary Diagnosis. La diabetes es la principal causa de insuficiencia renal en fase substitutiva
- 2. Mecanismos implicados en el daño renal y la expansión mesangial en la nefropatía diabética • Activación de PKC y MAPK • Aumento de la formación de productos de Amadori. • Aumento de formación de productos avanzados de glucación. (AGES) • Aumento del flujo de glucosa a través de la vía de los polioles. • Incremento de la vía de aldosa reductasa. • Aumento del paso de glucosa por la vía de las hexosaminas. • Aumento de producción de tromboxane y otros eicosanoides. • Aumento del estrés oxidativo y de carbonilos. • Aumento de la producción renal de factores de crecimiento proescleróticos TGF- β, PDGF, IGF-1, HGF, substancias vasoactivas: Ang-II, ET-1 y quimiocinas (IL-8, MCP-1) Sperling MA. Type 1 Diabetes, Etiology and Treatment 2003. Humana Press SINDROME METABOLICO
- 3. Specific classes of oral hypoglycemic and hypolipidemic agents are associated with renoprotective effects. RAS blockade remains the mainstay of treatment. Novel agents that target different pathophysiologic pathways in diabetic nephropathy are being investigated. Algunas medidas orientadas al control de la nefropatía diabética Dounousi E, et al. Rev Diabet Stud (2015) 12:119-133
- 4. Esquema preventivo y terapéutico en la nefropatía diabetica Intervención Meta Tratamiento renoprotector ACEi o BRA(Evitar combinar ACEi y BRA) Meta < 130/80 en algunos casos resistentes < 140/90 Antihipertensivo Utilizar en casos con Proteína urinaria de 0.5-1 g/d TFG que disminuye > 2 ml/min/año Control glucémico Hba1c 7 % Restricción de proteínas 0.8 g/Kg/día en TFG < 30 ml/min/1.73m2 Protección cardiorenal adicional Restricción de sal < 5g/día o mayor Hipolipemiantes <70-100 mg/dl de LDL-C, < 150 mg/dl Tg Antiplaquetarios Profilaxis de trombosis Ejercicio Al menos 30 min/día 5 días/semana Control de peso Perseguir el peso ideal Tabaquismo Supresión total del hábito Modificado de: Satirapoj B, Adler SG Kidney Res Clin Pract 2014;33:121–131 Aspirina
- 5. HIPERTENSION ARTERIAL SISTOLICA Y DETERIORO DE FUNCION RENAL EN DIABETES
- 6. NUEVAS OPCIONES DE INTERVENCION EN ESTUDIO EN LA NEFROPATIA DIABETICA • Antiinflamatorios - Inhibidores de COX y de xantina oxidasa ?? -Inhibidores de la proteina quimioatrayente de monocitos-1 (MCP-1) - Inhibidores de TNF-α -Señalización de NF-β • Inhibidores de PKC • Inhibidores de HMG-CoA reductasa • Papel de receptores de endotelina en la ND • Señalización Wnt en ND • Antioxidantes e inhibidores de estrés del retículo endoplásmico. • Nuevos enfoques moleculares -Micro RNAs - Mecanismos epigenéticos en la ND
- 7. PAPEL DE COX Y PGE2 EN LA NEFROPATIA DIABETICA Sharma D et al. Diab Res Clin Pract 2017;1 2 8: 9 1 –1 0 8 PLA2: Phospholipase A2; PGE2: Prostaglandin E2; COX-1 and COX-2: Cyclooxygenase-1 and 2; EP receptors: Prostaglandin E2 receptors. EP Receptors: Receptores de Prostanoides La inhibición de COX-2 podría tener efectos benéficos debido a la inhibición de COX-2 en podocitos y atenuación de la hiperfilttración. El papel de COX-2 en el daño renal puede depender de las fuentes de origen de COX, el mecanismo del daño renal y la expresión y el subtipo de los receptores de PGE asi como el momento de la inhibición de COX-2
- 8. COX-2–selective NSAIDs can cause acute renal failure and should be avoided or at least used cautiously for short periods of time (with close monitoring) in patients with chronic renal insufficiency. In addition, randomized, prospective studies should be undertaken to evaluate the renal safety of COX-2 selective agents compared with nonselective COX inhibitors in a large number of high-risk patients. American Journal of Kidney Diseases, Vol 35, No 5 (May), 2000: pp 937-940 COX inhibition, reduces proteinuria in patients with kidney disease. However, by diminishing renal blood flow and intraglomerular pressure it may also precipitate acute kidney injury in predisposed individuals. Whether therapeutically targeting pathway members that lie downstream of the COX enzymes themselves can alter the natural history of kidney disease remains uncertain. Inhibicion de prostaglandinas y nefropatía diabética ONO-AE3-208 (selective inhibitor of EP4) prevents podocyte dedifferentiation induced by transforming growth factor-ß1 (TGF-ß1). The difference in the renal effects of ONO-AE3-208 and captopril, despite both being accompanied by an equivalent reduction in albuminuria, suggested to us that the reno-protective effects of EP4 inhibition are not limited to actions on hemodynamic forces. Likewise, the observation that the reno-protective effect of ONO-AE3-208 was also apparent in non-diabetic SNx rats suggested to us that this effect was also not restricted to high glucose mediated events. Scientific Reports | 7: 3442 | DOI:10.1038/s41598-017-03237-3 June 2017
- 9. • HIPERGLUCEMIA • OBESIDAD FACTORES DE CRECIMIENTO • AUMENTO DE AGNE • LIGANDOS CELULARES • HIPERTENSION • CITOCINAS TLR: Toll-like receptors MCP-1: Proteina quimioatrayente de monocitos-1 IL-6: Interleucina-1 NF-β: Factor nuclear β INFLUENCIA DE DIVERSOS FACTORES SOBRE NF-β NF-β is a protein complex that controls transcription of DNA, cytokine production and cell survival. NF-κB is found in almost all animal cell types and is involved in cellular responses to stimuli such as stress, cytokines, free radicals, heavy metals, ultraviolet irradiation, oxidized LDL, and bacterial or viral antigen
- 10. eNOS ET-1 VEGF PAI-1 NF-B NAD (P) H OXIDASAS TGF- Colágena Fibronectina fibrinolisis ROS Flujo sanguíneo anormal Permeabilidad Vascular Angiogénesis Oclusión Capilar Oclusión vascular Expresión de Genes proinflamatorios Efectos Múltiples HIPERGLUCEMIA DIACILGLICEROL DE FORMAS Y DE PKC
- 11. Have been associated with vascular alterations such as increases in: • Permeability • Contractility • Extracellular matrix synthesis • Cell growth and apoptosis • Angiogenesis, • Leukocyte adhesión • Cytokine activation and inhibition. Linked to • Development of pathologies affecting Large vessels (atherosclerosis, cardiomyopathy) and • Small vessels (retinopathy, nephropathy and neuropathy) PKC:Diversas isoformas: PKC-α, PKC-β 1 / 2 Y PKC-
- 12. EFECTO DE LA RUBOXISTAURIN (INHIBIDOR ESPECIFICO DE PKC EN LA NEFROPATIA DIABETICA Tuttle KR, et al. Am J Kidney Dis. 2015;65(4):632-638
- 13. The single pivotal study provided only marginal evidence of efficacy in the ITT population. This was not confirmed in the population of completers or per protocol. Thus, the study does not provide robust evidence of efficacy and does not comply with the CHMP “Points to consider document” on application with 1. Meta-analysis; 2. One Pivotal study (CPMP/EWP/2330/99). Further confirmatory evidence of efficacy is required. • There was a concern regarding QT prolongation with ruboxistaurin. • There is a concern regarding CPK increase with RBX and in particular possible interactions with statins. • Further, the interaction with tricyclic anti-depressants, neuroleptics and other non anti-arrhythmic QT prolonging drugs, in view of possible additive/synergistic effects on Q-T interval prolongation is a matter of concern.
- 14. Role of inflammatory cascade and its inhibition by 3-Hydroxy-3-methylglutaryl coenzyme A (HMG-COA) reductase PAI-1, ECM and eNOS) in kidney which finally leads to kidney damage. ECM: Extracellular matrix; PAI-1: Plasminogen activator inhibitor-1; eNOS: Endothelial nitric oxide synthase. The small GTP-binding proteins Ras and Rac1 are molecular switches exchanging GDP for GTP and converting external signals in response to a variety of stimuli. Ras and Rac1 play an important role in cell proliferation, cell differentiation, and cell migration. Rac1 is directly involved in the reorganization and changes in the cytoskeleton during cell motility. Nitric oxide (NO) stimulates the Ras – ERK1/2 MAP kinases
- 15. EFECTOS DE ANGIOTENSINA II Y ENDOTELINA EN RIÑON Am J Physiol Regul Integr Comp Physiol 2016; 310: R877–R884
- 16. ENDOTHELIN-1
- 17. Egido J , Rojas-Rivera J, et al. Expert Opinion on Investigational Drugs 2017 doi.org/10.1080/13543784.2017.1325872 EFECTO PROTECTOR DE INHIBIDORES DE ET R EN NEFROPATIA DIABETICA ATRESANTAN BOSENTAN Atresantan produce aumento de peso, retención de lÍquidos y disminución de hemoglobina en pacientes con DM y nefropatía sin embargo sin evidencia significativa de edema o insuficiencia cardiaca. DISMINUCION DE ALBUMINURIA Y PROTECCIÓN RENAL
- 18. Vías epigenéticas afectadas por la hiperglucemia
- 19. MECANISMOS EPIGENETICOS EN NEFROPATIA DIABETICA TGF-β:Transforming growth factorβ; RAAS: Renin angiotensin aldosterone system; PKC: Protein kinase C; AGEs: Advanced glycation end produc
- 22. The RAS including the novel ACE2/Ang(1–7) axis Karnik SS. British Journal of Pharmacology (2017) 174 737–753 737
- 23. Efectos potenciales de ACE2 y angiotensina 1-7 sobre la regulación de la presión arterial Nat. Rev. Cardiol. 11, 413–426 (2014)
- 24. POSIBLES APLICACIONES EN MEDICINA DE LA ANGIOTENSINA 1-7 Passos-Silva DG, verano-Braga T, Santos RAS. Clinical Science 2013;124:443-456
- 25. Padda RS, et al. J Diabetes Metab. 2015; 6 Angiotensina 1-7 en la nefropatía diabética
- 26. CONCEPTO ACTUAL DE LOS RECEPTORES A ANGIOTENSINA 1-7 British Journal of Pharmacology (2017) 174 737–753
- 27. Los riñones de ratones db/db muestran aumento de la acetilación de FOXO1, y disminución de SIRTUINA1 y PPARα que fueron completamente revertidos por tratamiento con angiotensina 1-7
- 28. LA AMPLIFICACION DEL RECEPTOR DE ANGIOTENSINA 1-7 NO PROTEGE A LOS RATONES DEL DESARROLLO DE NEFROPATIA DIABETICA Wyzoki J, et al. Kidney international 2016
- 29. HIPERGLUCEMIA ADP ATP Fosforilación oxidatiiva ROS AGEs Glucoxidación AGNE LDLox RADICALES LIBRES AUMENTO DE 2dos MENSAJEROS PKC MAPK NFB DISFUNCION Y DAÑO CELULAR GSH GSSGANTIOXIDANTES glutatión se convierte en su forma oxidada disulfuro de glutatión (GSSG).
- 30. REPRESENTACION ESQUEMATICA DEL ESTADO DE MARCADORES DE ESTRÉS OXIDATIVO EN PRESENCIA DE DIABETES MDA: malondialdehyde, AOPP: Advanced oxidation protein products, PCO: protein carbonyls, GSH: reduced glutathione, and SOD: superoxide dismutase. Existe un aumento de oxidación y una disminución del sistema antioxidante Journal of Biomarkers 2013http://dx.doi.org/10.1155/2013/378790
- 31. ESTRÉS OXIDATIVO Y RESPUESTAS CELULARES Japan Medical Association Journal 2002; 45: 271
- 32. Deen WM. J. Clin. Invest. 114:1412–1414 Glomerular capillary wall, consisting principally of a fenestrated endothelium, a basement membrane, and epithelial foot processes. The foot processes form filtration slits spanned by slit diaphragms. Also shown is the endothelial cell coat, or glycocalyx. Some approximate dimensions are (8, 10): minimum diameter of fenestra, 30 nm; GBM thickness, 200–400 nm (depending on species); width of filtration slit, 40 nm. The glycocalyx thickness is uncertain
- 33. P = Podocitos. Las flechas indican la localización de la nefrina GBM = Membrana basal glomerular LOCALIZACION GLOMERULAR DE LA NEFRINA (MICROSCOPIA ELECTRÓNICA) EN LAS HENDIDURAS DIAFRAGMATICAS. DE LOS PODOCITOS Ruotsalainen V, Jungberg L, Wartiovaara P, et al Proc Nat Acad Sci USA 1999; 96: 7962
- 34. Toyoda M, Suzuki D, Umezono T, et al, Nephrol Dial Transplant 2004; 19: 380–385 EXPRESIÓN DEL RNAm DE LA NEFRINA HUMANA EN LA NEFROPATIA DIABÉTICA
- 35. Conadesuca.gob.mx Utilización del jarabe de maíz de alta fructosa en la industria en México desde 1970 y mortalidad por diabetes
- 36. Consumo de jarabe de maíz de alta fructosa (HFCS), fructosa libre y consumo total de fructosa, y prevalencia de obesidad
- 37. Promoción del desarrollo de diabetes ? Daño renal
- 39. Señales de insulina, inflamación y señales de estrés En presencia de resistencia a la insulina, mediadores inflamatorios y lípidos activan una cascada de señales que dispara cinasas inflamatorias como JNK e IKK asi como PKC,S6K,mTOR y ERK. La activación de JNK e IKK resulta en la inhibición de la acción de insulina en parte a través de la fosforilación en la serina de los substratos del receptor de insulina (IRS) 1 y 2. La energía del exceso de nutrientes puede inducir estrés del retículo endoplásmico que esta directamente ligado a la activación de vías inflamatorias que a su vez bloquean la acción de la insulina y regulan transcripcionalmente la producción de citocinas inflamatorias. Los ROS que se producen durante el estrés de organelos y disfunción mitocondrial contribuyen a estos efectos. La consecuencias finales son estrés del RE, aumento de la inflamación, inhibición de la acción de insulina y posiblemente de la acción de Leptina que culminan en disfunción metabólica.
- 40. Cell 2010;140: 900–917 Hotamisligil GKS Factores que pueden afectar el funcionamiento del retículo endoplásmico Failure of the ER’s adaptive capacity results in activation of the unfolded protein response (UPR), which intersects with many different inflammatory and stress signaling pathways. These pathways are also critical in chronic metabolic diseases such as obesity, insulin resistance, and type 2 diabetes. The ER and related signaling networks are emerging as a potential site for the intersection of inflammation and metabolic disease. Falla de la capacidad adaptativa del reticuloendoplásmico (ER) resulta en activación de la respuesta de proteínas no plegadas (UPR) que es afectada por diferentes vías y señales de señalamiento de estrés. Estas vías también son críticas en enfermedades metabólicas crónicas tales como obesidad, resistencia a la insulina y DMT2. El RE y las redes de señalamiento están emergiendo como un posible sitio de importancia en enfermedades metabólicas e inflamatorias.
- 41. Endoplasmic reticulum (ER) stress response The UPR has three aims: initially to restore normal function of the cell by halting protein translation, degrading misfolded proteins, and activating the signaling pathways that lead to increasing the production of molecular chaperones involved in protein folding. If these objectives are not achieved within a certain time span or the disruption is prolonged, the UPR aims towards apoptosis. UPR = Unfolded protein response PERK function is essential for cell survival following exposure of cells to ER stress, but the mechanisms whereby PERK signaling promotes cell survival are not thoroughly understood. We have identified the Nrf2 transcription factor as a novel PERK substrate IRE1: ER stress sensor and cell fate executor ATF6 is an endoplasmic reticulum (ER) membrane-anchored transcription factor
- 42. Al unirse oxLDL al receptor escavenger CD36 dispara la activación de la transcripción del factor PPARγ lo que induce a una presentación aumentada del receptor en la superficie del macrófago. NFB también es estimulado por oxLDL induciendo la síntesis de diversas citocinas. Además oxLDL desencadena la activación de cinasas relacionadas con CD36 tales como Lyn,MEKK2, JNK1 y JNK2 Efecto de oxLDL sobre macrófagos via el receptor scavenger CD36, NF-kB (factor nuclear potenciador de las cadenas ligeras kappa de las células B activadas) es un complejo proteico que controla la transcripción del ADN. NF-kB se encuentra en la mayoría de tipos de células animales y está implicado en la respuesta celular frente a estímulos como el estrés, las citoquinas, radiación ultravioleta, LDL oxidadas y antígenos bacterianos o virales
- 43. Consequences of VEGF-A increase in diabetic nephropathy VEGF-induced thickening and distortion of podocyte foot processes in diabetic mice, observed by scanning electron microscopy. A) Control diabetic glomerulus; B) Vegf164 overexpressing glomerulus showing wider foot processes. Scale bars=2 μm. Tufro A, Veron D, Semin Nephrol. 2012 July ; 32(4): 385–393. VEGF-A increases TGFβ, CTGF and established a positive feedback loop, leading to extracellular matrix (ECM) accumulation and GBM thickening (orange); VEGF-A induces nephrin downregulation and foot process effacement (FPE) (green); VEGF-A stimulates eNOS, which in the setting of high ROS leads to peroxinitrite (ONOO−) and further ROS generation, a positive feedback loop (blue), the dashed line represents the normal negative feedback regulation of VEGF-A by NO, not operative in DN. Low NO and high ROS damage endothelial cells and induce HTN.
- 44. Vitamin D binding to VDR inhibits targets responsible for declining renal function. The combined inhibition of heparanase and the RAA axis has proved capable of controlling the onset of proteinuria. In addition, the combined inhibition of heparanase and the TGFβ pathway may prevent the progression of fibrosis mediated by tubular epithelial–mesenchymal transi EFECTO DE VITAMINA D EN LA NEFROPATIA DIABETICA Masola V et al. J Pathol 2016;238: 7-9
- 45. Mechanism by which uric acid contributes to the development of renal and non-renal diseases. RAS, renin–angiotensin system. Johnson RJ , Nakagawa T, Jalal D , Sánchez-Lozada LG et al. Nephrol Dial Transplant 2013; 28: 2221–2228
- 46. Patel1 SR, Malhotra A, White DP, Gottlieb DJ. Et al. Am J Epidemiol. 2006; 164: 947–954. Mean age-adjusted weight of the Nurses’ Health Study cohort from 1986 to 2002 as a function of habitual sleep duration Patel et al. In analyses adjusted for age and body mass index, women sleeping 5 hours or less gained 1.14 kg (95% (CI): 0.49, 1.79) more than did those sleeping 7 hours over 16 years, and women sleeping 6 hours gained 0.71 kg (95% CI: 0.41, 1.00) more. The relative risks of a 15-kg weight gain were 1.32 (95% CI: 1.19,1.47) and 1.12 (95% CI: 1.06, 1.19) for those sleeping 5 and 6 hours, respectively. The relative risks for incident obesity (body mass index: >30 kg/m2) were 1.15 (95% CI: 1.04, 1.26) and 1.06 (95% CI: 1.01, 1.11). These associations remained significant after inclusion of important covariates and were not affected by adjustment for physical activity or dietary consumption
- 47. Hydration and Chronic Kidney Disease Progression: A Critical Review of the Evidence Am J Nephrol 2016;43:281–292 Clark WF, Sontrop JM, Huang SH
- 48. A number of experimental studies in rats and a few observations in humans suggest that vasopressin increases GFR and albuminuria, thus inducing a vicious circle as suggested by Brenner for a high protein diet. Adapted from Brenner. Am J Nephrol 2016;43:281–292
- 49. Prevalencia de patrón A o B de acuerdo con la proporción de hidratos de carbono en la dieta Ronald M Krauss Annu. Rev. Nutr. 2001. 21:283–95 Men with a predominance of small, dense LDL (pattern B) on the high-fat diet (n D 18) exhibited a twofold greater reduction in LDL cholesterol than did pattern A men. This was associated with significantly greater reductions in mass of midsized (LDL2) and small (LDL3) LDL subfractions measured by analytic ultracentrifugation. Only pattern B subjects showed significant reductions in plasma apoB, and in LDL relative to HDL cholesterol levels Patron A No aterogénico sin hiperlipidemia postprandial. Patron B Aterogénico con hiperlipidemia postprandial
- 50. Fructose-induced metabolic syndrome is associated with glomerular hypertension and renal microvascular damage in rats Laura G. Sanchez-Lozada,1 Edilia Tapia,1 Adriana Jiménez,1 Pablo Bautista,1 Magdalena Cristobal,1 Tomas Nepomuceno,1 Virgilia Soto,2 Carmen Avila-Casado,2 Takahiko Nakagawa,3 Richard J. Johnson,3 Jaime Herrera-Acosta,1† and Martha Franco1 In the present study, plasma UA levels correlated with fructose ingestion even in individual animals as demonstrated by the positive correlation between % fructose caloric intake and UA at week 8. Previously, we demonstrated that rats made hyperuricemic by inhibiting uricase with oxonic acid had increased blood pressure, afferent arteriole thickening,glomerular hypertension, and cortical vasoconstriction (29). In the present study, we found positive linear relationships between plasma uric acid and SBP (r 0.54, P 0.01) and arteriolar area (r 0.64, P 0.001) and a negative correlation with ultrafiltration coefficient, a marker of glomerular vasoconstriction(r 0.41, P 0.05). Therefore, higher UA levels induced by 60% fructose diet may be partially responsible for the glomerular hemodynamic alteration Am J Physiol Renal Physiol 292: F423–F429, 2007. Departments of 1Nephrology and 2Pathology, Instituto Nacional de Cardiología Ignacio Chávez, Mexico City, Mexico; and 3Nephrology, Hypertension and Transplantation, University of Florida, Gainesville, Florida
- 51. Hazard ratios greater than 1 demonstrate an increased risk for composite outcome with sulfonylurea compared with metformin. ACEi=angiotensinconverting enzyme inhibitor; ARB=angiotensin receptor blocker. N Engl J Med 2008; 359: 1577–15 METFORMIN SULFONYLUREA Adjusted hazard ratios for the composite outcome of glomerular filtration rate event or end-stage renal disease among age, race, HbA1c, and renin–angiotensin– aldosterone system blockade subgroups Kidney International 2012; 81: 698–706
- 52. Número de eventos, personas/año, tasas e índices de riesgo ajustados por cada resultado final en relación con medicamentos antidiabéticos 469 688 participantes con DM tipo 2 edades 25-84 entre abril 2007 a enero de 2015 Hippisley-Cox J, Coupland C. BMJ 2016;352 Hazard ratios adjusted for: sex; age; calendar year; duration since diagnosis of diabetes (five levels); ethnicity (nine levels); Townsend deprivation score; smoking status (five levels); use of anticoagulants, thiazides, ACE inhibitors, angiotensin 2 blockers; calcium channel blockers; statins; aspirin; existing complications (blindness, hyperglycaemia, hypoglycaemia, amputation, severe kidney failure); hypertension; cardiovascular disease; atrial fibrillation; chronic renal disease; rheumatoid arthritis; valvular heart disease; peripheral vascular disease; body mass index; systolic blood pressure; HbA1c; serum creatinine; cholesterol:high density lipoprotein ratio. Hazard ratios also mutually adjusted for use of each of the other diabetes drug classes. BLINDNESS RENAL FAILURE
- 53. Número de eventos, personas/año, tasas e índices de riesgo ajustados por cada resultado final en relación con medicamentos antidiabéticos 469 688 participantes con DM tipo 2 edades 25-84 entre abril 2007 a enero de 2015 Hippisley-Cox J, Coupland C. BMJ 2016;352 Hazard ratios adjusted for: sex; age; calendar year; duration since diagnosis of diabetes (five levels); ethnicity (nine levels); Townsend deprivation score; smoking status (five levels); use of anticoagulants, thiazides, ACE inhibitors, angiotensin 2 blockers; calcium channel blockers; statins; aspirin; existing complications (blindness, hyperglycaemia, hypoglycaemia, amputation, severe kidney failure); hypertension; cardiovascular disease; atrial fibrillation; chronic renal disease; rheumatoid arthritis; valvular heart disease; peripheral vascular disease; body mass index; systolic blood pressure; HbA1c; serum creatinine; cholesterol:high density lipoprotein ratio. Hazard ratios also mutually adjusted for use of each of the other diabetes drug classes. BLINDNESS RENAL FAILURE
- 54. Annuzzi G, Bozzetto L, Costabile G et al. Polyphenols improve fasting and postprandial dyslipidemia and reduce oxidative stress: a randomized controlled trial1–3 Am J Clin Nutr 2014;99:463–7100
- 55. Sachiko Hattori Sitagliptin reduces albuminuria in patients with type 2 diabetes Endocrine Journal 2011, 58 (1), 69-73
- 56. Comparación de linagliptina y placebo en varios puntos finales relacionados con nefropatía Am J Kidney Dis. 2015;66:441-449 Cooper ME, Perkovic V, McGill, JB, et al
- 59. Lang F. Kidney Blood Press Res 2017;42:483-494 LA INGESTION SUBOPTIMA DE LIQUIDOS PUEDE AUMENTAR LOS NIVELES DE VASOPRESINA Y GLUCOCORTICOIDES AUMENTANDO LA EXPRESION DE SGK1 FAVORECIENDO LAS PATOLOGIAS QUE SE SEÑALAN SGK1: Serine/threonine-protein kinase is also known as serum and glucocorticoid-regulated kinase 1 NFAT5, is a human gene that encodes a transcription factor that regulates the expression of genes involved in the osmotic stress
- 60. HIDRATACION Y ENFERMEDAD RENAL CRONICA
- 62. Am J Nephrol 2016; 43:281-92
- 63. Sirtuins target many proteins that are not histones they havebeen demonstrated to bind and deacetylate p53 in vitro and in vivo [32,33,41]. p53 is transcriptional activator, and its activation results in cell cycle arrest, senescence or the initiation of programmed cell death. Over expression of sirtuins has been shown to inhibit p53-dependent apoptosis in response to DNA damage and oxidative stress [33]. Recently, it has been reported that increased expression of p53 gene under diabetic condition is associated with renal apoptosis [42]. We found increasedexpression of p53 protein in the kidneys of diabetic animals as compared to their respective controls. However, the expression of p53 is reduced significantly in the kidneys of diabetic rats on IF regimen. The expression as well as activationof p53 is thought to be mediated by Sir2 dependent deacetylation. They both share an inverse relationship as is evident from our results wherein the Sir2 expression is decreased and at the same time p53 is upregulated. Intermittent fasting prevents the progression of type I diabetic nephropathy in rats and changes the expression of Sir2 and p53 FEBS Letters 581 (2007) 1071–1078
- 64. TRATAMIENTO POTENCIAL DE LA NEFROPATIA DIABETICA CON ANGIOTENSINA 1-7 Padda RS, et al. J Diabetes Metab. 2015; 6
- 68. POSIBLES EFECTOS DEL METILGLIOXAL EN DIVERSAS PATOLOGIAS DEL PACIENTE CON DIABETES
- 71. ENDOTHELIN-1 INHIBIDORES DE ENDOTELINA EN NEFROPATIA Expert Opinion on Investigational Drugs 2017
- 72. Compared with other types of tea, green tea is unfermented and contains the highest concentration of catechins, in which EGCG accounts for as much as 50% of its total polyphenols and has been reported to possess antioxidative, antiinflammatory, and anticarcinogenic effects[EGCG is estimated to be 25 times more potent than vitamin E and 100 times more potent than vitamin C. Bao H, Peng A. J Translat Int Med 2016;4: 99-103 EFECTOS DEL TE VERDE COMO ANTIOXIDANTE EN LA ALBUMINURIA SEVERAL MECHANISMS
- 73. Growth hormone (GH)–GH receptor (GHR)–IGF-1 axis in type 1 diabetes (1) reduced portal insulin levels results in decreased expression of hepatic GHR, impaired IGF-1 production and elevated IGFBP-1 levels (2). Low bioavailability of IGF-1 leads to compensatory GH hypersecretion via negative feedback loop mechanism (3). Except in liver, GHR expression in other tissues including kidney is not compromised. Elevated GH levels in poorly controlled type 1 diabetes associated with elevated GHR and IGF-1 in the kidney (4). Elevated GH levels are implicated in the renal hyperfiltration, glomerulosclerosis, nephromegaly, and proteinuria (5). Frontiers in Medicine 2017: (July )
- 74. MODELO PROPUESTO DE LA ACCION DE LA HORMONA DE CRECIMIENTO SOBRE LOS PODOCITOS Los efectos de GH incluyen: desdiferenciacion de podocitos, engrosamiento y/o formación de puentes cruzados de la membrana basa,l deterioro de los podocitos y puede producir apoptosis e hipertrofia. Todos estos efectos resultan en disminución del número de podocitos y alteración de la función glomerular. Este efecto puede verse tanto en la acromegalia como en la diabetes tipo 1.
- 76. Conclusiones • Existen múltiples líneas de investigación dirigidas a la fisiopatología, prevención y tratamiento de los pacientes con nefropatía diabética. • Varias de estas líneas han establecido conocimientos sólidos, muchos de ellos en animales de experimentación pero aun con pocos estudios clínicos y aun en etapas tempranas de evaluación. • Las recomendaciones vigentes siguen siendo las que tienen más bases en estudios controlados. • El control de la glucemia, de la hipertensión arterial, de los lípidos, el evitar medicamentos nefrotóxicos y controlar adecuadamente cada elemento del síndrome metabólico siguen siendo los mejores lineamientos en la prevención y tratamiento de los pacientes con diversos grados de compromiso renal. • La monitorización del control y las posibles complicaciones a intervalos adecuados es de vital importancia. • El obtener consejo de los especialistas en nefrología es muy importante para los médicos que tratan pacientes diabéticos sobre todo cuando ya existe evidencia de compromiso renal. • Es muy importante que el paciente reciba una educación adecuada en relación con los factores de riesgo de esta y otras complicaciones de la diabetes, y la necesidad de mantener un control estricto y con los exámenes pertinentes que permitan valorar sud condiciones de salud, para poder detectar tempranamente esta alteración.