
Recommended
More Related Content
What's hot
What's hot (20)
Similar to proximal humerus fracture fixation teaching
Similar to proximal humerus fracture fixation teaching (20)
More from All India Institute of Medical Sciences, Bhopal
More from All India Institute of Medical Sciences, Bhopal (20)
Recently uploaded
Recently uploaded (20)
proximal humerus fracture fixation teaching
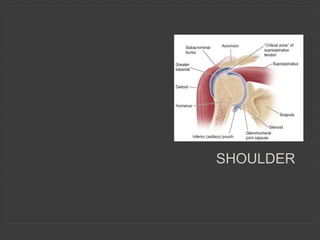
- 1. SHOULDER
- 2. FUNCTIONAL RESULTS AFTER FRACTURE SURGERY: UNPREDICTABLE • Complex anatomy • Interaction of anatomic structures • Numerous muscle attachments • Subacromial Bursa
- 4. BLOOD SUPPLY • Vascularisation of the humeral head is possible ONLY via the ascending branch of the anterior humeral circumflex artery Gerber et al. JBJS 72A:1486,1990
- 5. INITIAL WORKUP • History: Mechanism of injury – High/Low energy • Clinical Assessment: Look: ?? Dislocation, Feel: Axillary nerve, Clavicle # ??, Surgical emphysema (rib #s) • Neurological Exam: Brachial plexus injury • Vascular Injury
- 6. FACTORS GUIDING CHOICE OF T/T PATIENT FACTORS* • Physiological age • Patient’s choice • Hand dominance • Multiple medical co-morbidities • Poor mental status (non compliant) • Associated injuries • Timing of presentation *Krishnan SG et al. Hemiarthoplasty for proximal humeral fracture. Orthop Clin North Am.2008;39:441
- 8. At 3 momths
- 9. At 6 months
- 11. AW 46 O - AT SURGERY
- 13. SURGERY • Reduction held with 3 K wires • Retain/ Reconstruct medial buttress
- 14. MEDIAL BUTTRESS – ALLOGRAFT • Robinson CM. JBJS(Br) 2010;92-B:672 • Gardener MJ. J Orthop Trauma 2008;22:195
- 15. MEDIAL BUTTRESS – SYNTHETIC BONE SUBSTITUTE (CALLOS)
- 16. MEDIAL BUTTRESS – CALLOS 14/12
- 17. MEDIAL COMMUNITION - MEDIALISATION • Lee CW. Prognostic factors for unstable fractures treated with locking-plate fixation. J Shoulder Elbow Surg 2009;18:83
- 18. COMPLICATIONS • Screw penetration • Varus malreduction – implant failure* • AVN – 5 – 17%** • *Agudelo J et al Analysis of efficacy and failure in proximal humerus fractures treated with locking plates. J Orthop Trauma 2007;21(10):676 • **Greiner S et al. Humeral head necrosis rate at midterm FU for PH#. Injury 2009;40:186-91
- 20. 83 FEMALE COPD, DIABETIC, OSTEOPOROSIS
- 21. 4 PART FRACTURE DISLOCATION: VASCULAR COMPROMISE WITH ROTATOR CUFF INJURY
- 22. 89 Female IHD HT
- 24. NON-UNION WITH ROTATOR CUFF COMPROMISE
- 27. 1. Failure of fixation of tuberosities 2. Lack of maintenance of offset - Stem height 3. Version of the humeral stem
- 28. STANDARD TECHNIQUE FOR FIXATION OF TUBEROSITIES • 4 Horizontal Tension Bands – across both tuberosities and around neck of prosthesis • 2 Vertical Tension Bands • Ticron 5
- 29. HEMI – STEM HEIGHT • Provides adequate lever arm for the rotator cuff. • Shortening >1cm prevents optimum function* • How do we calculate?? medial calcar** prosthesis : glenoid relationship distance from pec major tendon to top of humeral head is constant (51 – 54mm)*** *Boileau P et al. Shoulder arthroplasty for fractures: problems and solutions. Shoulder arthroplasty.Heidelberg:Springer-Verlag;1999:297 **Mighell MA et al. Outcomes of hemiarthroplasty for fractures of the proximal humerus. J Shoulder Elbow Surg. 2006;72:387 ***Murachovsky J et al. Pectoralis major tendon reference: a new method. J Shoulder Elbow Surg 2006;15:675
- 30. HEMI - RETROVERSION • Range 20° - 40°* • Reliance on the bicipital groove** • Use of the fracture jig *Kontakis et al.The bicipital groove as a landmark for orientation of the humeral prosthesis. J Shoulder Elbow Surg 2001;10:136 **Baig et al. Bicipital groove orientation: considerations for the retroversion of a prosthesis. J Shoulder Elbow Surg 2006;15:195
- 31. DISPLACED FRACTURES???? Is functional outcome of displaced fractures similar in both conservative & surgical t/t ??
- 32. DISPLACED FRACTURES???? Is functional outcome of displaced fractures similar in both conservative & surgical t/t ?? Handoll et al Cochrane Review 2007 McLaurin TM. PHF Are we operating on too many? Bull Hosp J Dis 2004;62:24 Zyto K et al Non-operative t/t of comminuted fractures of the PH in elderly patients. Injury 1998;29(5):349 Rasmussen S et al. Displaced PHF:results of conservative t/t.Injury 1992;23(1):441 Rangan A et al. JAMA. ProFHer Trial 2010
- 33. PROXIMAL HUMERAL FRACTURES • Buckle # • SH Classification. • Displacement % Varus/Valgus
- 34. WHAT IS ACCEPTABLE REDUCTION? • The proximal physis contributes 80% of the length of the humerus. • Enormous remodelling potential • The older child with greater deformity may be treated with closed reduction -controversial • Approximate indications are: – 5-12 years - accept 60 degree angulation and 50% displacement – >12 years - accept 30 degrees angulation and 30% displacement
- 35. INDICATIONS FOR MUA/ PINNING • >50% displacement of the humeral head relative to the shaft • Angulation AP or lateral x-ray of >60 degrees in a child <12 years >30 degrees in a child >12 years • Pathological fracture of the proximal humerus • Associated injuries, i.e. brachial plexus injury, vascular injury • In association with other unilateral upper limb fractures and multiple trauma
- 37. ROTATOR CUFF - COMPONENTS • Supraspinatus • Infraspinatus • Teres Minor • Subscapularis
- 38. ROTATOR CUFF - COMPONENTS • Supraspinatus • Infraspinatus • Teres Minor • Subscapularis Which is the 5th component?
- 39. ROTATOR CUFF: PRIME FUNCTIONS • Prime INITIATOR of Abduction • ROTATION of the Humerus (90% of external rotation strength) • STABILISER of the joint (Muscular balance) • COMPRESSOR of the Humeral head into the glenoid fossa DELTOID ---- FORCE of Abduction (55%)
- 40. BIOMECHANICS: ARM ELEVATION STABILITY: Rotator Cuff & Long head of Biceps Shoulder Girdle Complex muscles FORCE & ENDURANCE: Deltoid Rotator Cuff BALANCE BETWEEN DELTOID FORCE & ARM WEIGHT
- 41. DELTOID MOMENT > ARM WEIGHT MOMENT = ELEVATION
- 42. PROF GRAMMONT’S CONCEPT • CR – medialised & stabilised • 10mm more lateralisation of humerus L2>L1 • Deltoid length/force increased (164%) F2>F1
- 43. PROF GRAMMONT’S CONCEPT • CR – medialised & stabilised • 10mm more lateralisation of humerus L2>L1 • Deltoid length/force increased (164%) F2>F1
- 44. ROTATOR CUFF TEAR - MINOR • Elevation normal – ENDURANCE shorter • Elevation by external rotation of the shoulder – biceps becomes the head depressor for the deltoid to act
- 45. ROTATOR CUFF TEAR – WHO? • Age 45 yrs • 40% “never done strenuous physical work” • Cuff defects frequently bilateral • Many heavy manual labourers never develop cuff defects • 50% no recollection of shoulder trauma Neer CS II Impingement Lesions,Clin Orth173:70-77;1983
- 46. INJURY - ACUTE TEARS • Uncommon • High Impact injury Fall from a height Mountain biking RTAs (Motor bikers) Often associated with shoulder dislocation & other injuries: Brachial plexus • Overhead athletics
- 47. OVERHEAD ATHLETICS / SPORTS • Pathology* Tensile overload Outlet impingement Internal impingement • Asymptomatic throwers have rotator cuff abnormalities *Rotator cuff tears in overhead athletes. Economopoulos KJ1, Brockmeier SF. Clin Sports Med. 2012 Oct;31(4):675-92.
- 48. HIGH IMPACT INJURY COMPLETE TEARS • Investigation – MRI • Surgical repair • Open • Arthroscopic
- 49. OVERHEAD ATHLETICS • Acute Partial Tears • Acute on chronic tears
- 50. ACUTE PARTIAL TEARS • <50% partial thickness tears* • Conservative management • Surgical Debridement* Decompression surgery** • Good results *Débridement of small partial-thickness rotator cuff tears in elite overhead throwers. Reynolds SB et al Clin Orthop Relat Res. 2008 Mar;466(3):614-21 **Partial thickness rotator cuff tears: Results of arthroscopic treatment. Snyder SJ et al Arthroscopy: The Journal of Arthroscopic & Related Surgery Vol 7, Issue 1, March 91, 1-7 **Rotator cuff tears in overhead athletes. Economopoulos KJ1, Brockmeier SF. Clin Sports Med. 2012 Oct;31(4):675-92.
- 51. ACUTE COMPLETE TEARS • Investigation: Ultrasound / MRI • Treatment: Surgical • Time: within 3 weeks* *Acute Tears of the Rotator Cuff: The Timing of Surgical Repair. Bassett RW, Cofield RH Clinical Orthopaedics & Related Research: May 1983 Vol 175