Seronegative spondyloarthropathies
•Download as PPT, PDF•
6 likes•611 views

Education /spine imaging

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Seronegative spondyloarthropathies
Similar to Seronegative spondyloarthropathies (20)
Recently uploaded
Recently uploaded (20)
Seronegative spondyloarthropathies
- 1. SERONEGATIVE&SEROPOSITIVE SPONDYLOARTHROPATHIES BY DR; SAMEH A RAOUF PROFESSOR OF RADIO DIAGNOSIS AIN SHAMS UNIVERSITY
- 2. OBJECTIVES: 1. Describe the essentials of diagnosis for the disorders in this category. 2. Review the signs, symptoms and physical examination and imaging findings commonly associated with these disorders.
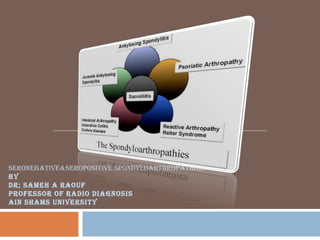
- 3. Seronegative = ANA negative, RF negative Spondyloarthropathy = vertebral arthritis Ankylosing Spondylitis (AS) Reiter’s Syndrome & Reactive Arthritis Psoriatic Arthritis (Ps A) Arthritis associated with IBD (Irritable Bowel Disease or Enteropathic Arthritis), Crohn’s arthropathy. Undifferentiated Spondyloarthropathies (uSpA) Juvenile Spondylitis.
- 4. Seronegative spondylarthropathy consists of a spectrum of chronic inflammatory disorders that lack the presence of rheumatoid factor and are clearly distinct from rheumatoid arthritis. Where as rheumatoid arthritis involves predominantly the synovial joints, significant abnormalities in the cartilaginous joints, entheses, as well as synovial articulations are seen in spondylarthropathic processes.
- 5. The seronegative spondyloarthropathies are a group of arthritic diseases that affect multiple organ systems and are thought to have a significant genetic component to their origin.
- 6. Axial skeleton involvement Prominent sacroiliitis Variable peripheral joint involvement Inflammatory eye disease Uveitis Enthesopathy HLA-B27
- 7. HLA-B27 is the most important predictor of AS. 90+% of Caucasians with AS are B27+ Studies suggest B27 antigen accounts for 20-50% of the risk for AS There are 23 known subtypes of HLA B27 and not all are associated with disease Suggests a structure-function relationship. The absence of HLA-B27 expression in an individual patient does not exclude the diagnosis of AS.
- 8. Ankylosing Spondylitis 90% Reactive arthritis 40-80% Juvenile Sp A 70% IBD 35-75% Psoriatic arthritis With axial disease 50% Peripheral disease 15% Undifferentiated Sp A 70% Acute anterior uveitis 50% Aortic insufficiency, heart block 80%
- 9. Young adults Peak onset ages 20-40 overall prevalence is estimated to be as high as 0.2–2%. Males>Females (4:1). More common in Caucasians
- 10. Skeletal Axial arthritis (eg, sacroiliitis and spondylitis). Arthritis of ‘girdle joints’ (hips and shoulders). Peripheral arthritis uncommon. Others: enthesitis, osteoporosis, vertebral, fractures, spondylodiscitis, pseudoarthrosis. Extraskeletal Acute anterior uveitis. Cardiovascular involvement. Pulmonary involvement. Cauda equina syndrome. Enteric mucosal lesions. Amyloidosis, miscellaneous.
- 11. Back pain >3months. Morning stifnness. Tenderness over the SI joints& spinal tenderness 2ry spondyolitis Multiple different maneuvers (all unreliable) Reduced range of motion of the back. Reduced chest expansion owing to costosternal and costovertebral affections. Peripheral joints affection e.g. shoulders and hips. The lower limbs are more frequently involved than the upper limbs. In 20–25% of AS patients, peripheral articular symptoms may precede axial manifestations. Painful tendinopathy occurs in about 10%
- 12. Evaluation of other joints Particular attention to the large joints Lab evaluation HLA-B27 Imaging for AS SI joints, others as clinically indicated
- 13. Clinical Criteria Low back pain, > 3 months, improved by exercise, not relieved by rest Limitation of lumbar spine motion, sagittal and frontal planes Limitation of chest expansion relative to normal values for age and sex • Radiologic Criteria – Sacroiliitis grade ≥ 2 bilaterally or grade 3 – 4 unilaterally • Grading – Definite AS if radiologic criterion present plus at least one clinical criteria – Probable AS if: • Three clinical criterion • Radiologic criterion present, but no signs or symptoms satisfy clinical criteria
- 20. Sacroiliac Joints and Pelvis Sacroiliitis is the hallmark of Ankylosing spondylitis. Sacroiliitis is the earliest radiographic sign in 99% of cases of AS Although Sacroiliitis alone is a non-specific finding and is not sufficient for the diagnosis of AS. Changes in the sacroiliac joints are considered ubiquitous among patients with AS . Both the synovial and ligamentous (superior and posterior) portions of the joint are involved. Classically, the involvement is symmetric and bilateral particularly very early in the course of the disease. unilateral disease may occur.
- 22. Conventional Radiographic Findings in Ankylosing Spondylitis Small erosions lined up one behind the other at corresponding sites of the ilium and the sacrum resemble a string of beads or rosary. The erosions usually develop earlier on the iliac than on the sacral side of the joint possibly because the cartilage covering the sacrum is approximately twice as thick as that covering the ilium . Reactive bone proliferation is seen radiographically as sclerosis of the adjacent cancellous bone with a variable pattern (diffuse, band shaped,spotty, triangular).
- 25. Abnormalities of the spine can be seen at: The disco vertebral junctions. Apophyseal joints, costovertebral joints. Posterior ligamentous attachments, and atlantoaxial joints. Classically, changes are initially noted at the thoracolumbar and lumbosacral junctions. Spinal extension to the midlumbar, as well as the upper thoracic and cervical vertebrae, occurs with disease progression but may be arrested at any stage .
- 26. There is a spectrum of: Inflammatory and destructive lesions of the spine in AS. This predominantly involves the cartilaginous disco vertebral junction. One of the earliest plain-film findings of spinal involvement, typically seen at vertebrae T10 through L2, is the so-called Romanus lesion, also known as spondylitis anterior
- 30. Marginal osteosclerosis. Along the spectrum of discovertebral diseases are the more destructive lesions, such as Andersson lesions. Three types are distinguished: Type I shows central focal endplate destruction with intraosseous disc herniation and associated reactive endplate changes, the nature of which depends on the age of the lesion. In the relatively acute stage, marrow edema is identified, with enhancement after intravenous gadolinium contrast administration Type-II lesions are located more at the periphery of the discovertebral junction. Type-III lesions involving both the central and the peripheral portions may be difficult to differentiate from infectious spondylodiscitis.
- 31. Diagnostic features: The absence of an anterior paraspinal soft tissue mass . The predominant low signal intensity of the intervertebral disc on T2-weighted images (with only possible minor areas of high signal intensity adjacent to vertebral erosions) indicate a noninfectious Andersson lesion.
- 36. Vertebral bodies initially erode at corner, reactive sclerosis occurs below this leading to squared appearance Eventually anulus fibrosus and longitudinal ligaments become ossified (syndesmophytes) Discs can become calcified, along with all ligaments including those between spinous processes bamboo spine Dagger sign, fused spinous process ligaments http://uwmsk.org:8080/EvasMSKTF/
- 40. Magnetic resonance imaging : Enable early diagnosis of spinal manifestations of AS by an increased sensitivity for identification of early-stage Sacroiliitis or vertebral osteitis. Is also superior to other imaging techniques for differential diagnosis of Andersson lesions vs. infectious spondylodiscitis and in the evaluation of most acute and chronic spinal complications of AS. MRI has been used to assess the effect drugs in the management of acute inflammatory lesions
- 41. Classical Reiter’s syndrome Arthritis, uveitis, urethritis “Incomplete Reiter’s” Undifferentiated spondyloarthropathy
- 42. Peripheral arthritis Abrupt onset, asymmetric oligoarthritis Lower extremities Enthesopathy Sausage digits, heel pain (Achilles), plantar pain Inflammatory spinal pain Evidence of preceding infection GU or GI most common
- 43. Inflammatory eye disease Conjunctivitis, iritis Cardiovascular Aortic root dilatation, conduction disturbances Genital and skin lesions Gut mucosal changes Association with HIV
- 44. Reactive Arthritis (Reiter's arthritis)
- 45. Reactive Arthritis (Reiter's arthritis)
- 46. Inflammatory polyarthritis associated with psoriasis May occur prior to the onset of skin disease Usually seronegative M=F Prevalence rate 0.1%
- 47. Inflammatory DIP disease Asymmetic oligoarthritis with large and small joints Symmetric polyarthritis Arthritis mutilans Spondyloarthropathy Spondylitis and sacroiliitis
- 48. Nail pitting Skin disease Pitting edema Inflammatory eye disease
- 52. Bilateral, asymmetrical Dramatic joint space loss +/- ankylosis (arthritis mutilans) Bone proliferation, “mouse ears” “pencil-in-cup” deformities Normal mineralization Sausage digits Hands > feet > SI > spine Usually favors DIP and PIP in hand SI involvement usually bilateral, asymmetrical Large bridging bone formation in spine, similar to reactive arthritis http://uwmsk.org:8080/EvasMSKTF/ Sausage digits http://uwmsk.org:8080/EvasMSKTF/ http://www.hopkins-arthritis.org/arthritis- info/psoriatic-arthritis/diagnosis.html Psoriatic Arthritis
- 54. abnormal normal
- 55. The appearance of arthritis in patients with inflammatory intestinal disease (ulcerative colitis, Crohn’s disease, and Whipple’s disease) has been described since 1950 These abnormalities have been designated enteropathic arthritis . Both the peripheral joints and the axial skeleton (spondylarthropathy) may be involved enteropathic arthritis. The axial skeleton is involved in about 10% of patients. Radiological manifestations of enteropathic spondylarthropathy (sacroiliitis and spondylitis) are indistinguishable from AS. Axial involvement is poorly correlated with activity of bowel disease, whereas a close temporal association exists between exacerbations of intestinal disease and peripheral joint inflammation
- 58. SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) Is considered as a spondylarthropathy associated with different types of cutaneous pustules. The term pustulotic arthro-osteitis (PAO) is more appropriate.
- 61. • Pathology of Rheumatoid Arthritis: RA is the prototype of conditions accompanied by a hyperplastic, inflammed synovial membrane. In RA and related diseases, the synovial lining becomes hyperemic and thickened, with extensive overgrowth and formation of villi. Inflamed synovial lining in RA eventually grows over the articular surfaces, eroding and destroying cartilage and underlying bone. The invasive portion of the hyperplastic synovial tissue has been termed pannus.
- 62. MR manifestations of RA and related diseases are nonspecific , similar changes can be seen in other inflammatory joint conditions. Therefore the goal of those using MRI in these conditions is not to achieve a specific diagnosis, which may be accomplished using clinical and laboratory parameters, but to assess the extent of the early soft tissue and bone manifestations.
- 65. Pathogenesis of Rheumatoid Arthritis Choy, E. H.S. et al. N Engl J Med 2001;344:907-916
- 66. MRI features Of RA: Erosion of the cartilage and bone. Tendon or ligamental invasion. Synovial pannus :MRI has been used to demonstrate pannus ,and synovial cysts.
Editor's Notes
- Clinical Features of AS Sacroiliitis is the hallmark feature of AS1 and the earliest, most consistent findings are traceable to effects of sacroiliitis and enthesitis. Inflammation of the discovertebral, apophyseal, costovertebral, and costotransverse joints of the spine, and paravertebral ligamentous structures are frequently associated with AS. After many years, chronic inflammation can cause bony ankylosis.2 Chronic low back pain and stiffness, which typically worsens following a period of prolonged inactivity (eg, morning stiffness), are common presentations.1 Over time, lumbar spine mobility becomes restricted in all planes and posture becomes abnormal because of flattening of the lumbar spine and accentuated dorsal spine kyphosis. Radiographic findings in advanced disease include erosions, sclerosis of adjacent bones, pseudo-widening of the sacroiliac joint space, and fibrosis, calcification, interosseous bridging, and ossification of the sacroiliac joints. Extraskeletal manifestations are also frequently part of the clinical picture.2 Khan MA. Spondyloarthropathies. In: Hunder GG, ed. Atlas of Rheumatology. 3rd ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2002. Khan MA. Clinical features of ankylosing spondylitis. In: Hochberg MC, Silman AJ, Smolen JS, Weinblatt ME, Weisman MH, eds. Rheumatology. vol 2, 3rd ed, New York, NY: Mosby; 2003:1161-1181.
- Modified New York Criteria for the Diagnosis of AS Three sets of clinical and radiographic criteria have been introduced over the past 40 years. The Modified New York Criteria,1,2 developed in 1984, are now widely used to diagnose AS. Radiographic evidence of sacroiliitis is heavily relied on to diagnose AS because it is the best nonclinical indicator of disease. Diagnosis may be missed early on, though, because routine pelvic radiographs may not clearly demonstrate sacroiliitis in the initial stages of AS.3 Van der Linden S. Ankylosing spondylitis. In: Textbook of Rheumatology 5th ed. Kelly WN, Harris ED, Ruddy S, Sledge CB, eds. Philadelphia, PA: WB Saunders; 1996:969-982. Van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984;27:361-368. 3. Khan MA. Spondyloarthropathies. In: Hunder GG, ed. Atlas of Rheumatology. 3rd ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2002.
- cricoarytenoid
- PMN’s in SF – inflammatory fluid WBC>2000 Pannus takes on special invasive properties
- Figure 2. Pathogenesis of Rheumatoid Arthritis. In the normal knee joint, the synovium consists of a synovial membrane (usually one or two cells thick) and underlying loose connective tissue. Synovial-lining cells are designated type A (macrophage-like synoviocytes) or type B (fibroblast-like synoviocytes). In early rheumatoid arthritis, the synovial membrane becomes thickened because of hyperplasia and hypertrophy of the synovial-lining cells. An extensive network of new blood vessels is formed in the synovium. T cells (predominantly CD4 ) and B cells (some of which become plasma cells) infiltrate the synovial membrane. These cells are also found in the synovial fluid, along with large numbers of neutrophils. In the early stages of rheumatoid arthritis, the synovial membrane begins to invade the cartilage. In established rheumatoid arthritis, the synovial membrane becomes transformed into inflammatory tissue, the pannus. This tissue invades and destroys adjacent cartilage and bone. The pannus consists of both type A and type B synoviocytes and plasma cells.