
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ORAL SURGERY( FRACTURE)
Similar to ORAL SURGERY( FRACTURE) (20)
Recently uploaded
Recently uploaded (20)
ORAL SURGERY( FRACTURE)
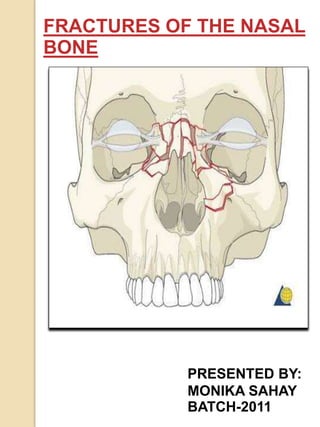
- 1. FRACTURES OF THE NASAL BONE PRESENTED BY: MONIKA SAHAY BATCH-2011
- 2. CONTENTS INTRODUCTION SITES OF INJURIES SYMPTOMS CAUSES DIAGNOSIS MANAGEMENT REFRENCES
- 3. INTRODUCTION Disruption or break in the continuity of bone structure is referred as fracture. A nasal fracture is commonly referred as a broken nose. Fractures of nasal bones are the most common trauma to the face because of the projection of nose on the face. Nasal fracture is usually the result of direct injury with other facial fractures. Fractures of the nasal bones and septal cartilage result in not only cosmetic deformity, but also functional disturbances.
- 4. SITES OF INJURIES ANTERIOR INJURIES LATERAL INJURIES
- 5. ANTERIOR INJURIES 1.Anterior injuries involves fractures of bridge of the nose, frontal process, lacrimal bones, and the septum. 2.Comminuted fragments may be driven laterally into the orbit or upward into ethmoid region. 3.Direct, violent, and/ or anterior force may result in smash fracture of anterior bone.
- 6. LATERAL INJURIES 1.Lateral injuries involve only one nasal bone with medial displacement. 2.In severe case, a violent blow from side results in fracture of both nasal bones and fracture of nasal septum with lateral shifting of entire bony framework. 3.This type of fracture is called “open book” fr
- 7. OPEN BOOK FRACTURE 4.There is collapse of the nasal septum with splaying out of the nasal bone like pages of an open book. 5.There may be telescoping or overlapping of fragments seen.
- 8. CAUSES Nasal fractures are caused by: - Physical trauma to the face. -Common sources of nasal fractures include: Sports injuries Fighting Falls Car accidents Falls from syncope Or impaired balance in the elderly.
- 10. WHAT DOES A NASAL FRACTURE LOOK LIKE? LATERAL INJURY
- 11. SIGNS AND SYMPTOMS OF A NASAL FRACTURE Nose pain Swelling of the nose Nosebleed Bruising around the nose and the eyes The nose is bent A grating feeling when nose is touched Blocked passages Nasal airway obstruction Nasal deformity
- 12. DIAGNOSIS On clinical evaluation nasal deformities like depressed bridge of the nose, flattening or deviation of the nasal bone is seen. In fresh fractures, edema, hematoma, lacerations, subconjuctival hemorrhage is seen. Subcutaneous emphysema may be present, because of patient’s repeated attempts to blow the nose. Circumorbital ecchymosis CSF rhinorrhoea may be
- 13. CLINICAL FEATURES DEPRESSED BRIDGE OF NOSE DEVIATED NOSE SUBCONJUCTIVAL HEMORRHAGE CIRCUMORBITAL ECCHYMOSIS
- 14. RADIOGRAPHIC EVALUATION Lateral views of the nasal bones,15° or 30° occipitomental projections can be taken. A lateral view taken with small dental film against the side of the nose also provides excellent detailed study. CT scan is helpful for higher level fractures of the nose.
- 16. MANAGEMENT Minor nasal fractures maybe allowed to heal on their own provided there is no significant cosmetic deformity. Closed reduction is the treatment of choice for most nasal bone and/ or septal fractures. Closed reduction can be done under LA with or without sedation or general anesthesia.
- 17. Closed Reduction: - It refers to manipulation of the bone fragments without surgical exposure of the fragments. -This allows the bone to grow back together. -It is carried under local anesthesia or general anesthesia. For manipulating the fragments Walsham’s and Asch’s forceps are used.
- 18. -Interfered by presence of oedema. -Best time is before the appearance of oedema, or after it has subsided (usually5-7days). -Difficult after 2 weeks because it heals by that time.
- 19. CLOSED REDUCTION AND SEPTAL REDCUTION INWARD ROTATION OF LEFT NASAL BONE. HORIZONTAL SEPTAL WALL FRACTURE BILATERAL COMMINUTED DISPLACED AND DEPRESSED NASAL FRACTURES ASCH FORCEPS WERE USED TO MANIPULATE SEPTUM INTO A STRAIGHTER POSITION, BUT NOT ENTIRELY SYMMETRIC.
- 20. At the end, internal stablization is done with nasal packing using half inch ribbon gauze saturated with antibiotic ointment. The pack is removed after 3 to 4 days. The external dressing consist of padding the area with cotton wool or gauze pieces and stablizing it with adhesive tape in “butterfly” manner, secured to the forehead and crossing over the nasal bridge on either side. Airway can be maintained
- 21. METHODS OF IMMOBLIZATION Splinting may be required for immobilization. 1.INTRANASAL SPLINTING: Ribbon gauze Stainless steel splint Use of ribbon gauze is the most standard method of providing intranasal support. A 1” ribbon gauze of 12-15cm length is taken and inserted in nose, in layers. -Inadequate anteroposterior support. -Difficulty in breathing from nose -Potential source of infection DISADVANTAGE:
- 22. EXTRANASAL SPLINTING Plaster of Paris Lead splints -The most commonly employed extranasal splint is the Plaster of Paris. -This consist of eight layers of Plaster of Paris splint bandage which is cut so as to produce a strip of plaster across the bridge on either side of the nose along with frontal extension. -The plaster should be moulded in shape of the nose, and it should not extent on to the soft part of the nose. -This is left in place for 1week.
- 23. -In case of mobile fracture which cannot be stablized with plaster of paris, lead plates can be used on either side of the nose. -These lead plates consist of two holes and are fitted on each side of the nose with help of tantalum or stainless steel sutures which are passed into the holes and beneath the nasal bone. -The splint is left in place for a period of 3 weeks.
- 24. SPLINTING DONE WITH PLASTER OF PARIS (A) LEAD PLATES, AND (B) SPLINTING (B) DONE WITH LEAD SPLINTS
- 25. OPEN REDUCTION INDICATION FOR OPEN REDUCTION: -Extensive fractures -Deviation of the nasal pyramid greater than one half width of the nasal bridge. -Open septal fracture -Persistent deformity after closed reduction.
- 26. COMPLICATIONS EARLY Epistaxis is common with nasal fracture and may recur with reduction. Hematoma is always a concern and must be excluded for each patient. CSF rihnorrhoea is uncommon but may occur when fractures extend to include the cribriform plate. LATE • Nasal obstruction • Secondary nasal deformity • Saddle nose deformity • Synechia • Septal perforation
- 27. -TEXTBOOK OF ORAL AND MAXILLOFACIAL SURGERY- Dr. Neelima Anil Malik -TEXT BOOK OF ORAL AND MAXILLOFACIAL SURGERY -SM BALAJI BIBLIOGRAPHY
- 28. THANK YOU