
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Liver surgery
Similar to Liver surgery (20)
More from Abed elrheem abomokh
More from Abed elrheem abomokh (6)
Recently uploaded
Recently uploaded (20)
Liver surgery
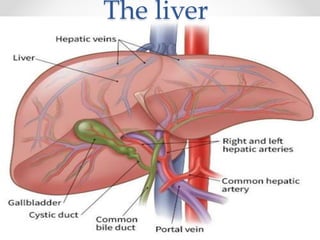
- 1. The liver
- 2. History of liver surgery Ancient Greek , hepar, derives from the verb hepaomai, which means “mend” or “repair.” The ancient Greek myth of Prometheus reminds us that the liver is the only organ that regenerates. principles are correct that after hepatic resection, the remnant liver will hypertrophy over weeks to months to regain most of its original liver mass. what is the maximum amount of liver that can be resected while retaining adequate liver function ?
- 3. • Liver before and after auto repair
- 11. Liver Innervation * Parasympathetic : - Anterior liver Lt Vagal Branch - Posterior Liver Rt Vagal Branch * Sympathetic : - Greater Thoracic splanchnic & celiac branches.
- 13. Lymph Drainage • Lymph is produced within the liver perisinusoidal space of Disse hilar cystic duct lymph node (Calot’s triangle node), common bile duct, hepatic artery, and retropancreatic and celiac lymph nodes.
- 15. Calot’s node - “hilar node”
- 16. Calot’s triangle
- 17. Liver Physiology • These include processes such as storage, metabolism, production, and secretion. • One crucial role is the processing of absorbed nutrients through the metabolism of glucose, lipids, and proteins. • The liver maintains glucose concentrations in a normal range over both short and long periods and in the fasting state. by performing several important roles in carbohydrate metabolism. (Glycogenolysis ,gluconeogenesis ,glycogen synthesis or glycolysis and lipogenesis.) • The liver also plays a central role in lipid metabolism through the formation of bile and the production of cholesterol and fatty acids. • Protein metabolism occurs in the liver through amino acid deamination, resulting in the production of ammonia as well as the production of a variety of amino acids. • the liver also is responsible for the synthesis of most circulating plasma proteins. (albumin, factors of the coagulation and fibrinolytic systems, and compounds of 2 the complement cascade. • the detoxification of many substances through drug metabolism occurs in the
- 19. Bile Synthesis
- 20. Drug Metabolism
- 21. Liver Function Test *Hepatic Cell Injury: • Aspartate transaminase (AST) • Alanine transaminase (ALT) • Alkaline phosphatase (AP) • γ-glutamyltranspeptidase (GGT) • Bilirubin * Liver Function: • Serum albumin levels • Prothrombin time (PT).
- 22. Abnormal synthetic function • Liver synthetic function is best assessed by: -Albumin level -INR ( PT ) • liver produces approximately 10 g of albumin per day. However, albumin levels are dependent on a number of factors such as nutritional status, renal dysfunction, protein-losing enteropathies, and hormonal disturbances.
- 23. Cholestasis • Cholestasis is a condition in which bile flow from the liver to the duodenum is impaired, due to intrahepatic causes (hepatocellular dysfunction) or extrahepatic causes (biliary tree obstruction). • detected by measuring the serum levels of bilirubin, AP, and GGT. • elevated indirect bilirubin level suggests intrahepatic cholestasis. • elevated direct bilirubin level suggests extrahepatic obstruction.
- 24. Jaundice • Yellowish discoloration of skin , sclera and mucus membrane with the pigment bilirubin. 1) Prehepatic : ( Excessive Hemolysis – insufficient gluco) A- genetic ( spherocytosis , leptocytosis , G6PD deficency) B- Acquired ( coomp’s test) 2) Intrahepatic (involve the intracellular mechanisms for conjugation and excretion of bile from the hepatocyte). 3) Extrahepatic ( extrinsic or intrinsic biliary obstruction )
- 25. Detectable when Bilirubin > ?? mg/dl.
- 26. Acute Liver Failure • Rate of extent of hepatocytes damage exceed the regenerative ability of the liver. • Around 2000 patient annually in U.S . • Development of Hepatic Encephalopathy within 26 weeks of severe liver injury with no previous history of liver diseases or portal HTN. • Before the introduction of orthotopic liver transplantation (OLT), the chance for survival was <20%. Currently, most series report 5-year survival rates of >70% for affected patients.2
- 27. • ETIOLOGY : - East Viral hepatitis A,B,E. - West Drug & Toxins . ALF need to be monitored in the intensive care unit (ICU) setting, and specific attention needs to be given to fluid management, ulcer prophylaxis, hemodynamic monitoring, electrolyte management, and treatment of infection. - Hypophosphatemia, a sign of hepatic regeneration, may indicate a higher likelihood of spontaneous recovery and needs to be corrected via intravenous (IV) administration of phosphate.
- 28. How to treat Acetaminophen overdose ?
- 29. • Few Hours of presentation ? Charcoal reduces the amount of acetaminophen in the GI tract. • N-acetylcysteine (NAC) 1.orally (140 mg/kg initial dose, followed by 70 mg/kg every 4 hours × 17 doses) 2. intravenous route (loading dose of 150 mg/kg, followed by a maintenance dose of 50 mg/kg every 4 hours × 12 doses).
- 30. Liver cirrhosis
- 31. Cirrhosis & portal HTN • Sustained wound healing in response to chronic liver injury presence of fibrous septa subdividing the parenchyma into hepatocellular nodules. • 40% of cirrhotic patients are asymptomatic. • ESLD – end stage liver disease is an indication for liver transplant with 5 year mortality of 50% of patient. • Liver cirrhosis is the most common nonneoplastic cause of death among patients with hepatobiliary and GI diseases. • Morphology : micronodular , macronodular ,mixed.
- 34. • Causes of portal HTN are: Prehepatic portal vein thrombosis. Hepatic cirrhosis , HCC , fibrosis. Posthepatic Budd-chiari syndrome. • Cirrhosis induced Portal HTN accounts for 90% of all Portal HTN cases. • Rule of 23 of portal HTN: 23 of cirrhotic patient develop Portal HTN 23 of portal HTN patient develop Esophageal varices. 23 of esophageal varices are ruptured.
- 35. * Clinical presentation of liver cirrhosis : • fatigue, anorexia, weight loss, jaundice, abdominal pain, peripheral edema, ascites, GI bleeding, and hepatic encephalopathy. *On physical examination Spider angiomata and palmar erythema (alterations in sex hormone metabolism), Finger clubbing , leukonychia duputyren’s contracture. * Clinical presentation of cirrhosis with portal HTN : • Esophageal varices , splenomegaly , caput medusa , hemorrhoids.
- 38. • Ruptured Esophageal varcies is the most dangerous complication of Portal HTN. • Ruptured esophageal acounts for 50% of upper GI bleeding in patients known to have esophageal varcies. Diagnostic test EGD “ upper GI endoscopy” . * Treatment of ruptured Esophageal Varices : • Large bore IV’s x 2 • Iv fluids , Foleys catheter , cross blood send labs. • Intubation to protect from aspiration.
- 39. Caput Medusa – Portal HTN
- 41. Example of palmar erythema- cirrhosis
- 42. Spider angioma
- 44. Infections of the liver • liver contains the largest portion of the reticuloendothelial system in the human body and is therefore able to handle the continuous low-level exposure to enteric bacteria that it receives through the portal venous system , nonviral infections are unusual.
- 45. Pyogenic Abscess • Most common abscess seen in the U.S . • 40% Monomicrobial. • 40% Polymicrobial. • 20% Negative Culture. • Commenst are Gram negative : E.coli (70%) , klibseila proteus. • Most common liver abscess in the U.S . • In patients with endocarditis and infected indwelling catheters, Staphylococcus and Streptococcus species are more commonly found. • Treatment include correction of the underlying cause and IV antibiotic therapy (8 weeks ).
- 46. Multiple hepatic Abscess. “ honeycomb appearance”
- 47. Amebic Abscess • Entamoeba histolytica is a parasite that is endemic worldwide, infecting approximately 10% of the world’s population.( areas with poor sanitaion). • Most commonly involve Rt superior anterior liver lobe. • Most common type of liver abscess worldwide. • Amebiasis should be considered in patients who have traveled to an endemic area and present with right upper quadrant pain, fever, hepatomegaly, and hepatic abscess. • Leukocytosis is common, whereas elevated transaminase levels and jaundice are unusual
- 49. “Amebic - Anchovy paste abscess”
- 50. • Ultrasound and CT scanning of the abdomen are both very sensitive but nonspecific for the detection of amebic abscesses. • Metronidazole 750 mg three times a day for 7 to 10 days is the treatment of choice and is successful in 95% of cases. • Aspiration of the abscess if : - large abscesses - not respond to medical therapy - superinfected. - abscesses of the left lobe of the liver at risk for rupture into the pericardium.
- 51. Hydatid Cyst • Hydatid disease is due to infection by the tapeworm Echinococcus granulosus in its larval or cyst stage. • 70 % of hydatid cysts found in the liver , others found in lung , brain or bone. • Hydatid cysts commonly involve the right lobe of the liver, usually the anterior-inferior or posterior-inferior segments . Eosinophilia is seen in approximately 30% of infected patients. Ultrasonography and CT scanning of the abdomen are both quite sensitive for detecting hydatid cysts.
- 53. Ring like calcifications - Hydatid cyst
- 54. • Unless the cysts are small or the patient is not a suitable candidate for surgical resection, the treatment of hydatid disease is surgically based because of the high risk of secondary infection and rupture. • Medical treatment with albendazole relies on drug diffusion through the cyst membrane(albendazole preferred over mebendazole ) • surgical resection involving laparoscopic or open complete cyst removal with instillation of a scolicidal agent is preferred and usually is curative. • If complete cystectomy is not possible, then formal anatomic liver resection can be undertaken.
- 55. Benign Liver Lesions • Hepatic Cyst • Adenoma • Hemangioma • Focal nodular hyperplasia • Bile duct Hamartoma
- 56. cyst • 1. primary (congenital ) • 2. secondary to trauma • 3. infection ( pyogenic/ parasitic) • 4. neoplastic disease. • In most cases, congenital cysts are differentiated from secondary cysts (infectious or neoplastic origin) in that they have : well-defined thin wall , no solid component and are filled with homogeneous, clear fluid.
- 57. Simple hepatic cyst Vs Infectious hydatid cyst
- 58. Hemangioma • Hemangiomas are the most common solid benign masses that occur in the liver. • They consist of large endothelial-lined vascular spaces • represent congenital vascular lesions that contain fibrous tissue and small blood vessels that eventually grow. • surgical resection can be considered if the patient is symptomatic. • Caution should be exercised in ordering a liver biopsy if the suspected diagnosis is hemangioma because of the risk of bleeding from the biopsy site..
- 59. Liver Hemangioma on CT
- 60. Adenoma • Hepatic adenomas are benign solid neoplasms of the liver. They are most commonly seen in premenopausal women older than 30 years of age and are typically solitary. • Use of Estrogen Contraceptives are clear risk factors. • Histologically : Adenoma lacks bile duct glands , kupffer cells , have no lobules and contain hepatocytes that are congested. • Hepatic adenomas also have a risk of malignant transformation to a well-differentiated HCC. Therefore, it usually is recommended that a hepatic adenoma (once diagnosed) be surgically resected.
- 61. Hepatic adenoma
- 62. Focal Nodular Hyperplasia • FNH is a solid, benign lesion of the liver believed to be a hyperplastic response to an anomalous artery. Similar to adenomas, they are more common in women of childbearing age. • Biphasic CT well circumiscribed lesion with central scar. • MRI The lesion appear black on both T1 & T2 • FNH lesions usually do not rupture spontaneously and have no significant risk of malignant transformation. Therefore, the management of FNH is usually reassurance and prospective observation irrespective of size. • Oral contraceptive or estrogen use should be stopped when either FNH or adenoma is diagnosed. ( stop it )
- 63. Malignant liver tumor • A – primary ( HCC , Cholangiocarcinoma) • B – Metastasis ( colorectal CA ) • Most common liver tumor is Metastasis colorectal cancer. • Around 150000 new cases of colorectal CA are diagnosed every year with 60% of them will have hepatic metastasis. • TO be continued .
Editor's Notes
- It is interesting to note that the ancient Greeks seem to have been aware of this fact, because the Greek word for the liver, hepar, derives from the verb hepaomai, which means “mend” or “repair.” Hence hepar roughly translates as “repairable.”1 The importance of the liver dates back to even biblicalti what is the maximum amount of liver that can be resected while retaining adequate liver function ? - 80%
- Coronary ligament Holds the liver to the inferior surface of diaphragm. Right Triangular ligament - Holds the liver to the Left triangular ligament Holds the liver to the Falcifrom Ligament Holds the liver to the anterior abdominal wall , Separating Lt Medial & Lt Lateral segments. Round Ligament It is the remnant of obliterated umbilical vein.
- Cantle’s line imiginary line divides the liver into Rt and Lt lobes.
- Hepatocaval ligament. ( connetcting the liver caudate lobe to the inferior vena cava.
- Commonest hepatic blood supply
- Hepatic blood supply variations.
- Rt Hepativ vein drains segments VI , VII . Middle Hepatic vein drains Segment IVa, IVb ,VI , VIII Left Hepatic vein drains Segment II , III * CAUDATE lobe ( Segment I ) drains directly to the IVC.
- A common source of referred pain to the right shoulder and scapula as well as the right side or back is the right phrenic nerve (c2-c5), which is stimulated by tumors that stretch Glisson’s capsule or by diaphragmatic irritation.
- Lymph is produced within the liver and drains via the perisinusoidal space of Disse and periportal clefts of Mall to larger lymphatics that drain to the hilar cystic duct lymph node (Calot’s triangle node), as well as the common bile duct, hepatic artery, and retropancreatic and celiac lymph nodes.
- Calot’s Triangle and Calots Node. important for resection of hilar cholangiocarcinoma, which has a high incidence of lymph node metastases.
- These include processes such as storage, metabolism, production, and secretion. One crucial role is the processing of absorbed nutrients through the metabolism of glucose, lipids, and proteins. The liver maintains glucose concentrations in a normal range over both short and long periods by performing several important roles in carbohydrate metabolism. In the fasting state, the liver ensures a sufficient supply of glucose to the central nervous system. (Glycogenolysis ,gluconeogenesis ,glycogen synthesis or glycolysis and lipogenesis.) The liver also plays a central role in lipid metabolism through the formation of bile and the production of cholesterol and fatty acids. Protein metabolism occurs in the liver through amino acid deamination, resulting in the production of ammonia as well as the production of a variety of amino acids. the liver also is responsible for the synthesis of most circulating plasma proteins. (albumin, factors of the coagulation and fibrinolytic systems, and compounds of 2 the complement cascade. the detoxification of many substances through drug metabolism occurs in the
- Bilirubin is the breakdown product of normal heme catabolism. Bilirubin is bound to albumin in the circulation and sent to the liver. In the liver, it is conjugated to glucuronic acid to form bilirubin diglucuronide in a reaction catalyzed by the enzyme glucuronyl transferase, making it water soluble. This glucuronide is then excreted into the bile canaliculi.
- The main components of bile are water, electrolytes, and a variety of organic molecules including bile pigments, bile salts, phospholipids (e.g., lecithin), and cholesterol. The two fundamental roles of bile are to aid in the digestion and absorption of lipids and lipid-soluble vitamins and to eliminate waste products (bilirubin and cholesterol) through secretion into bile and elimination in feces. The human liver can produce about 1 L of bile daily. The bile acids are derivatives of cholesterol synthesized in hepatocytes , the bile acids cholic acid and chenodeoxycholic acid. These bile acids are conjugated to either glycine or taurine before secretion into the biliary system. Bacteria in the intestine can remove glycine and taurine from bile salts. Bile salts secreted into the intestine are efficiently reabsorbed and reused. Approximately 90% to 95% of the bile salts are absorbed from the small intestine at the terminal ileum. transported back to the liver in the portal vein and re-excreted in the bile. Those lost in the stool are replaced by synthesis in the liver.
- In most cases, a drug is rela- tively lipophilic to ensure good absorption. Liver help in making it more hydrophilic to be more easily eliminated. Phase I reactions include oxidation, reduction, and hydrolysis of molecules. These result in metabolites that are more hydrophilic than the original chemicals. The cytochrome P450 system is a family of hemoproteins important for oxidative reactions involving drugs and toxic substances. Phase II reactions, also known as conjugation reactions, are synthetic reactions that involve addition of subgroups to the drug molecule. These subgroups include glucuronate, acetate, glutathione, glycine, sulfate, and methyl groups. Some drugs may convert onto active metabolites in the liver. During an overdose, the normal metabolic pathways are overwhelmed, and some of the drug is converted to a reactive and toxic intermediate by the cytochrome P450 system. Glutathione normally reacts with this intermediate, leading to the production and subsequent excretion of a harmless product. However, as glutathione stores are diminished, the reactive intermediate cannot be detoxified and it combines with lipid membranes of hepatocytes, which results in cellular necrosis. Thus, treatment of acetaminophen overdoses consists of replenishing glutathione stores by supplementing with sulfhydryl compounds such as acetylcysteine.
- This term is a misnomer, however, because most of these tests measure not liver function but rather cell damage. More accurate measurement of the liver’s synthetic function is provided by serum albumin levels and prothrombin time (PT).
- INR > 1.5 ALBUMIN < 3
- Intrahepatic : Gilbert syndrome , crigler-najjar , dupin johnson syndrome , viral hepatitis Extrahepatic : cholangitis , cholidocholethiasis , pancreatitis , pancreatic tumor , pancretic pseudocyst.
- Detectable when Bilirubin > 2.5 – 3 mg/dl.
- OLT= native liver is removed and replaced with donor organ in the same anatomic position of the original organ. MOST common cause of death is = High Intrcranial pressure follwed by sepsis and systemic organ faliure.
- N-acetylcysteine (NAC), the clinically effective antidote for acetaminophen over- dose, should be administered as early as possible to any patient with suspected acetaminophen-associated ALF.
- N-acetylcysteine (NAC), the clinically effective antidote for acetaminophen over- dose, should be administered as early as possible to any patient with suspected acetaminophen-associated ALF.
- ESLD – nutretional insufficency , coagulopathy , hepaticencphalopathy
- Example of Macronodular Cirrhosis.
- Example of Micronodular cirrhosis.
- Spleenomegaly is the most common clinical finding in cirrhosis and portal HTN.
- Esophageal varices are found in 40% of cirrhotic patients. Ruptured esophageal varcies is the oue biggest fear of Portal HTN. It is the connection of coronary vein ( esophageal branch of the left gastriv vein to the azygus vein) .
- EGD = esophagogastrodoudenoscopy
- Portal HTN the anastomosis of umbilical vein ( within falciform ligament) and epigastric vein.
- The Anastomosis of superior hemorrhoidal vein( superoir mesentric vein) with the middile & inferior hemorrhoidal vein.
- Alterations of sex hormones
- Alterations of sex hormones
- Unkown mechanism
- IV antibiotic therapy should be continued for at least 8 weeks and can be expected to be effective in 80% to 90% of patients
- cystic form passes through the stomach and small bowel unharmed and then transforms into a trophozoite in the colon. Here it invades the colonic mucosa forming typical flask-shaped ulcers, enters the portal venous system, and is carried to the liver. Occasionally, the trophozoite will pass through the hepatic sinusoid and into the systemic circulation, which results in lung and brain abscesses. Amebae multiply and block small intrahepatic portal radicles with consequent focal infarction of hepatocytes. They contain a proteolytic enzyme that also destroys liver parenchyma.
- abscess to resolve depends on the initial size at presentation and varies from 30 to 300 days.46 Both ultrasound and CT of the liver can be used as follow-up after the initiation of medical therapy
- Albendazole act on b-tubulin inhibiting microtubules. Scolicidal agent is hypertonic salt used to kill the protoscolices to prevent its spread to the patient tissues.
- Central scar = fibrous septa Flow fluids are seen black on both T1 & T2