2.
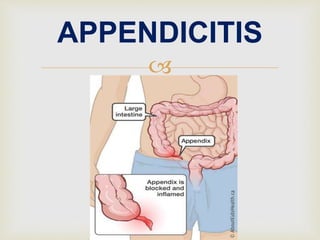
Appendicitis is an inflammation of the appendix, a
finger-shaped pouch that projects from colon on the
lower right side of abdomen. Appendicitis causes
pain in lower right abdomen. However, in most
people, pain begins around the navel and then
moves.
DEFINITION
3.
INCIDENCE
It can occur at any age but is rare in clients younger than
2 years and reaches a peak incidence in clients between
20 and 30 years.
It is not common in older adults; however when it does
occur in such clients, rupture of the appendix is more
common.
Appendicitis affects 7% to 12% of the population.
4.
5.
6.
There is no clear cause of appendicitis.
Obstruction of the appendiceal lumen causes appendicitis.
Mucus backs up in appendiceal lumen, causing bacteria
that normally live inside the appendix to multiply.
As a result, the appendix swells and becomes infected.
CAUSES AND RISK
FACTORS
7.
Sources of obstruction include food waste, hard piece of
stool, parasites, or growths that clog the appendiceal
lumen, enlarged lymph tissue in the wall of the appendix,
caused by infection in the gastrointestinal tract or
elsewhere in the body, inflammatory bowel disease and
trauma to the abdomen.
8.
PATHOPHYSIOLOGY
Due to etiological factors
Obstruction of the appendix lumen by faecioth
Decreased flow or drainage of mucosal secretion
Increased intra luminal pressure in the appendix
10.
Necrosis and perforation of appendix; bacteria invade in
appendix
Disruption of cell membrane and at last inflammation of
appendix
11.
The classic manifestation of appendicitis begins with acute
abdominal pain that comes in waves.
At first, the pain may be perceived merely as discomfort
that makes the client feel that passing flatus or having a
bowel movement will bring relief. Taking laxative during
this period may lead to rupture of the appendix and
peritonitis.
CLINICAL
MANIFESTATION
12.
The pain typically start in the epigastrium or
periumbilical region. It then shifts to the right lower
quadrant as the inflammatory process spreads to
involve the serosal layers of the bowel.
The pain becomes steady rather than intermittent, and
the client guards or protects the area by lying still and
drawing the legs up to relieve tension on the
abdominal muscles.
13.
Local tenderness is elicited at McBurney’s point when
pressure is applied.
Vomiting that begins after the pain starts.
Loss of appetite
Low-grade fever
Coated tongue
Bad breath
15.
Blumberg's sign, also referred to
as rebound tenderness, is a clinical
sign that is elicited during physical
examination of a patient's abdomen
by a doctor or other health care
provider. It is indicative of
peritonitis. It refers to pain upon
removal of pressure rather than
application of pressure to the
abdomen.
18. The obturator sign or Cope's obturator test is an indicator of
irritation to the obturator internus muscle. The technique for
detecting the obturator sign, called the obturator test, is carried
out on each leg in succession. The patient lies on her/his back with
the hip and knee both flexed at ninety degrees.
19.
Aaron's sign is a referred pain felt in the epigastrium
upon continuous firm pressure over McBurney's point. It
is indicative of appendicitis. Aaron's sign is named for
Charles Dettie Aaron, an American gastroenterologist.
20.
Diagnosis is based on results of a complete physical
examination and on laboratory and x-ray findings.
ASSESSMENT &
DIAGNOSTIC FINDINGS
21.
The complete blood cell count demonstrates an
elevated white blood cell count.
22.
Abdominal x-ray films, ultrasound studies, and CT scans may reveal
a right lower quadrant density or localized distention of the bowel.
23.
To correct or prevent fluid and electrolyte imbalance and
dehydration, antibiotics like Inj. Augmentin or Inj.
ampiclox and intravenous fluids are administered until
surgery is performed.
Analgesics like Inj. voveron can be administered after the
diagnosis is made.
MEDICAL MANAGEMENT
24.
Surgical intervention involves removal of the appendix
(appendectomy) within 24 to 48 hours of onset of the
manifestations. The surgery can be performed through a small
open incision or a laparoscope (a lighted scope used to visualize
and remove the appendix). When the operation is performed in
time, the mortality rate is less than 0.5%. delay usually causes
rupture of the organ and resultant peritonitis.
SURGICAL
MANAGEMENT
25.
1) Peritonitis:
Observe for abdominal tenderness,
fever, vomiting, abdominal rigidity,
and tachycardia.
Employ constant nasogastric suction
Correct dehydration as prescribed
Administer antibiotic agents as
prescribed.
POTENTIAL
COMPLICATION
26. 2) Pelvic abscess:
Evaluate for anorexia, chills, fever and
diaphoresis.
Observe for diarrhea, which may
indicate pelvic abscess
Prepare patient for rectal examination.
Prepare patient for surgical drainage
procedures.
27.
3) Subphrenic abscess (abscess under diaphragm):
Assess patient for chills, fever.
Prepare for x-ray examination.
Prepare for surgical drainage of abscess.
28.
4) Ileus (paralytic and mechanical)
Assess for bowel sounds.
Employ nasogastric intubation and suction.
Replace fluids and electrolytes by intravenous route as
prescribed.
Prepare for surgery, if diagnosis of mechanical ileus is
established.
29.
Goals include relieving pain, preventing fluid volume deficit,
reducing anxiety, eliminating infection from the potential or actual
disruption of the GI tract, maintaining skin integrity, and attaining
optimal nutrition.
NURSING MANAGEMENT
30.
Acute pain
Imbalanced nutrition less than body requirements
Impaired skin integrity
Ineffective tissue perfusion
Risk for deficient fluid volume
Risk for infection
Risk for injury
Nursing diagnosis