Case Review #F: Progressive adolescent-scoliosis
•
2 likes•453 views

A 22 year old female presented with a progressive 53° thoracic curve. She was treated with an Anterior Interbody fusion T9-L1.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (17)
Similar to Case Review #F: Progressive adolescent-scoliosis
Similar to Case Review #F: Progressive adolescent-scoliosis (15)
More from Robert Pashman
More from Robert Pashman (11)
Recently uploaded
Recently uploaded (20)
Case Review #F: Progressive adolescent-scoliosis
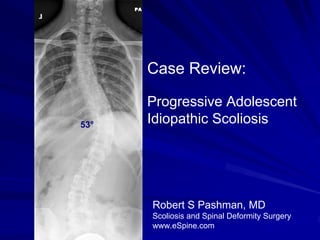
- 1. Case Review: Progressive Adolescent 53° Idiopathic Scoliosis Robert S Pashman, MD Scoliosis and Spinal Deformity Surgery www.eSpine.com
- 2. Patient History 22-year-old female Progressive Adolescent Idiopathic Scoliosis Patient presented with a 53° thoracic curve The patient has anatomic numbering anomaly including 11 rib-bearing vertebrae and 6 lumbar vertebrae. On sagittal x-ray the patient has significant lumbosacral kyphosis indicative of a forme fruste disk and vestigial disk. The apex of the curve variably counted around T11-12, T12- L1, depending on how the count would go - looks like on x-ray to be a thoracolumbar curve with a compensatory proximal left-sided thoracic curve. The patient's right shoulder is slightly depressed, but the upper curve bends out to the left from approximately 30 to 22 degrees, and therefore because of its flexibility and significant unrotated state will be called a compensatory curve. The patient could be classified as Lenke II if confirmed structurality of the proximal curve and/or a thoracolumbar with a proximal structural curve.
- 3. Pre-op X-rays The patient was diagnosed with Adolescent Idiopathic Scoliosis at 14 years old. She was treated with conservative 53° management which incuded: pilates, physical therapy, and chiropractic care.
- 4. Bending X-rays Right and left side-benders show the L1 vertebrae levels to the left of the Harrington midcarpal line and therefore right and left side- bending also shows that the T8-9 disk opens completely and therefore the levels of T9 to L1 will be chosen.
- 5. Indications for Surgery Progressive 50° right thoracolumbar Adolescent Idiopathic Scoliosis. Thoracic lumbar pain, secondary to progressive Adolescent Idiopathic scoliosis. Failed conservative therapy. Severe cosmetic deformity.
- 6. Surgical Strategy Anterior thoracoabdominal and short-segment anterior transvertebral fixation to attack the low thoracolumbar apex curve and to maintain flexibility of the proximal curve as well as the distal curve, which is compromised at this time because of the structural anomaly of the lumbosacral spine. T9 right thoracotomy, thoracoabdominal approach to the thoracolumbar spine. Removal, rib for rib graft harvesting. Radical diskectomy with spinal canal decompression, T9-10, T10-11, T11- 12 and T12-L1. Segmental spinal instrumentation, T9 to L1, with transvertebral pedicle screw-rod construct, double-staple system Legacy stainless steel 5.5. Anterior interbody fusion, T9, T10-11, T11-12, T12-L1 with recombinant human bone morphogenic protein and autogenous bone- harvested bone structural graft device. Intraoperative motor evoked potential interpretation. Intraoperative fluoroscopy and interpretation.
- 7. Post-Op Films Her thoracotomy is well-healed. The patient is not taking any pain medicine. Her balance is excellent. X-rays look good. No evidence of hardware failure. The patient is happy with her outcome.
- 8. Pre-Op/Post-op Comparison Her 53° curvature now has 24° 53° been reduced down to 24° and she is doing well.
- 9. Pre-Op/Post-op Comparison The patient’s spine is balanced. The fusion is still growing, and will be complete at 12 months post-op.