Downloaded 1,280 times


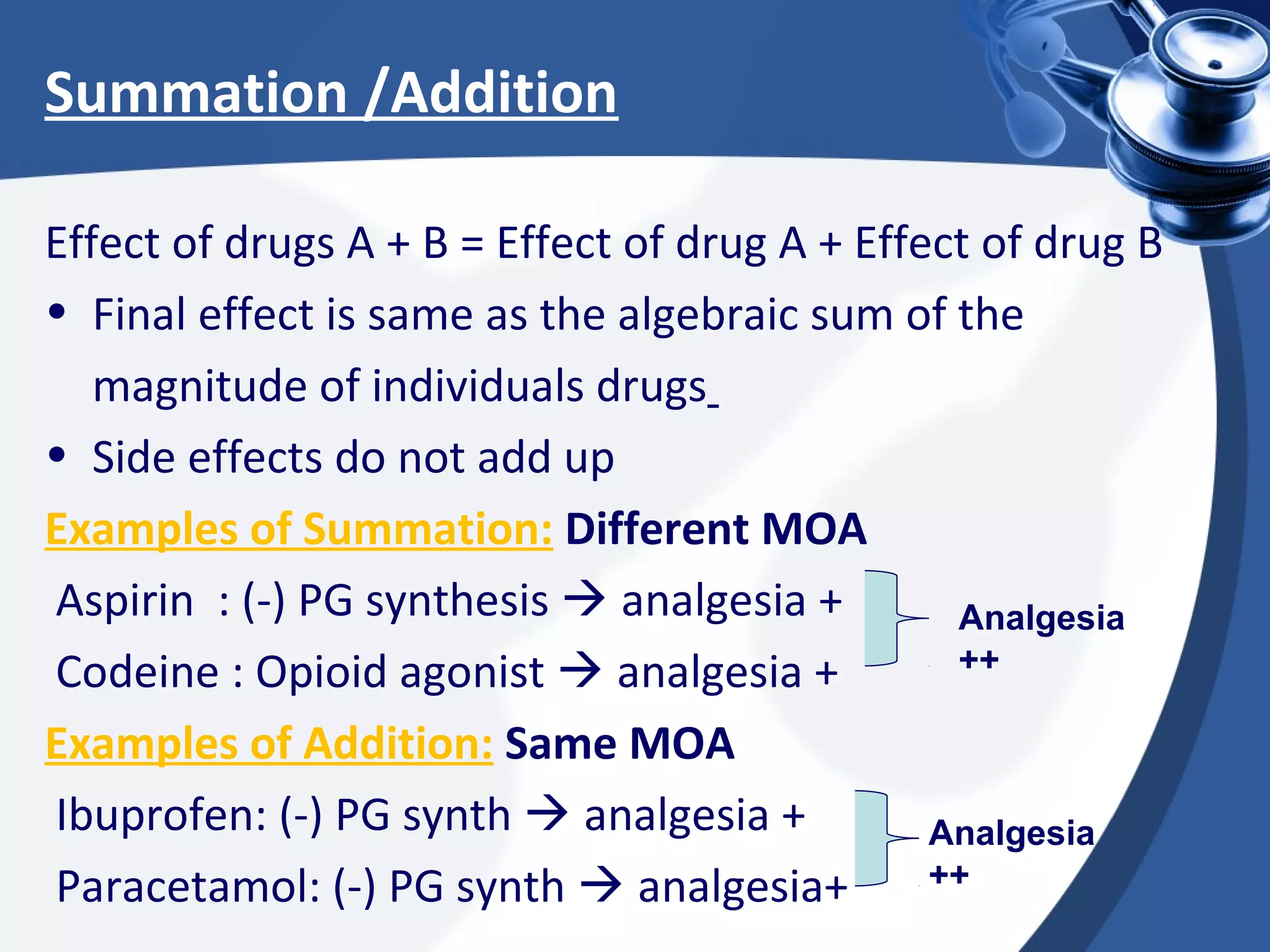
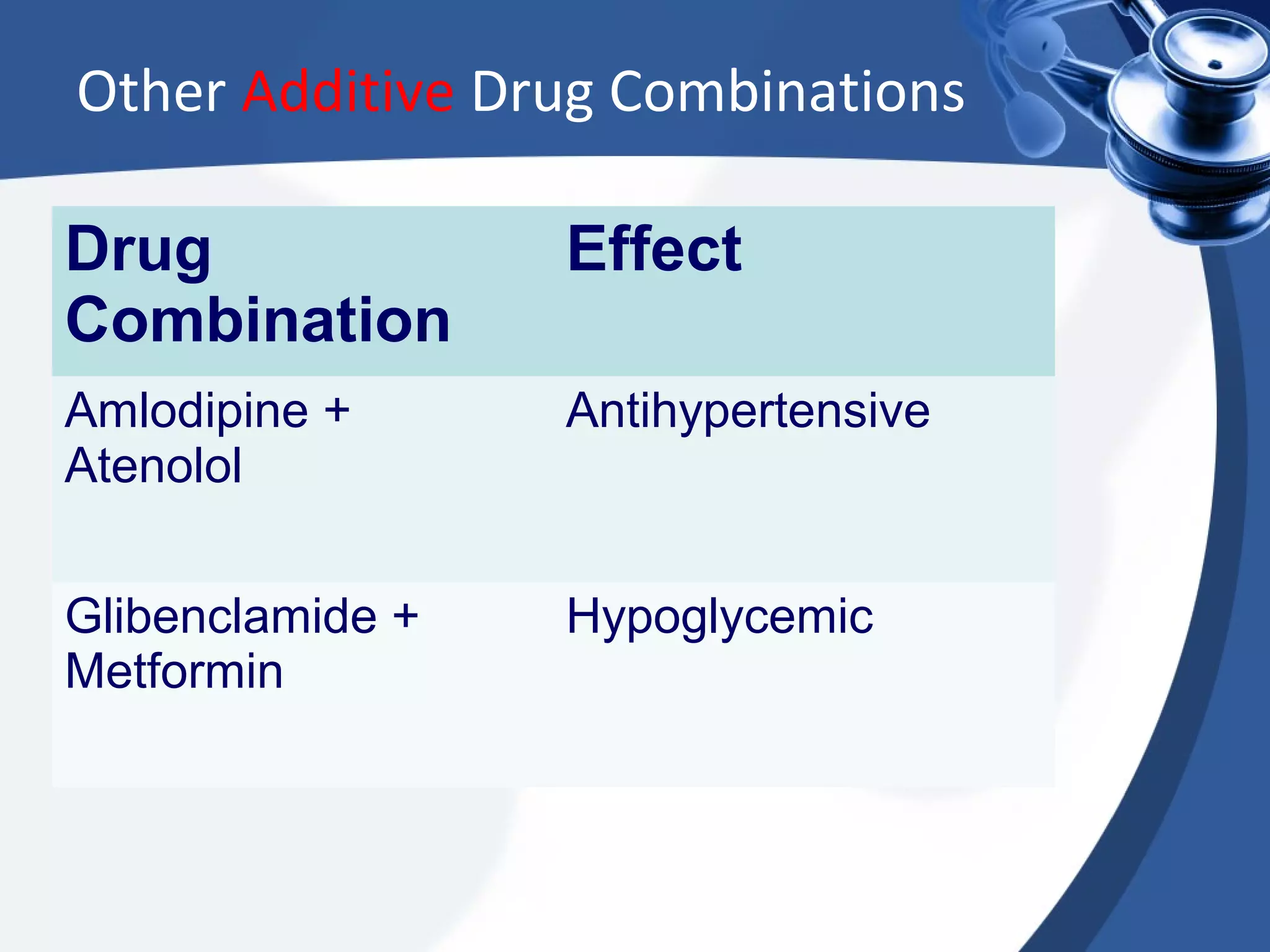
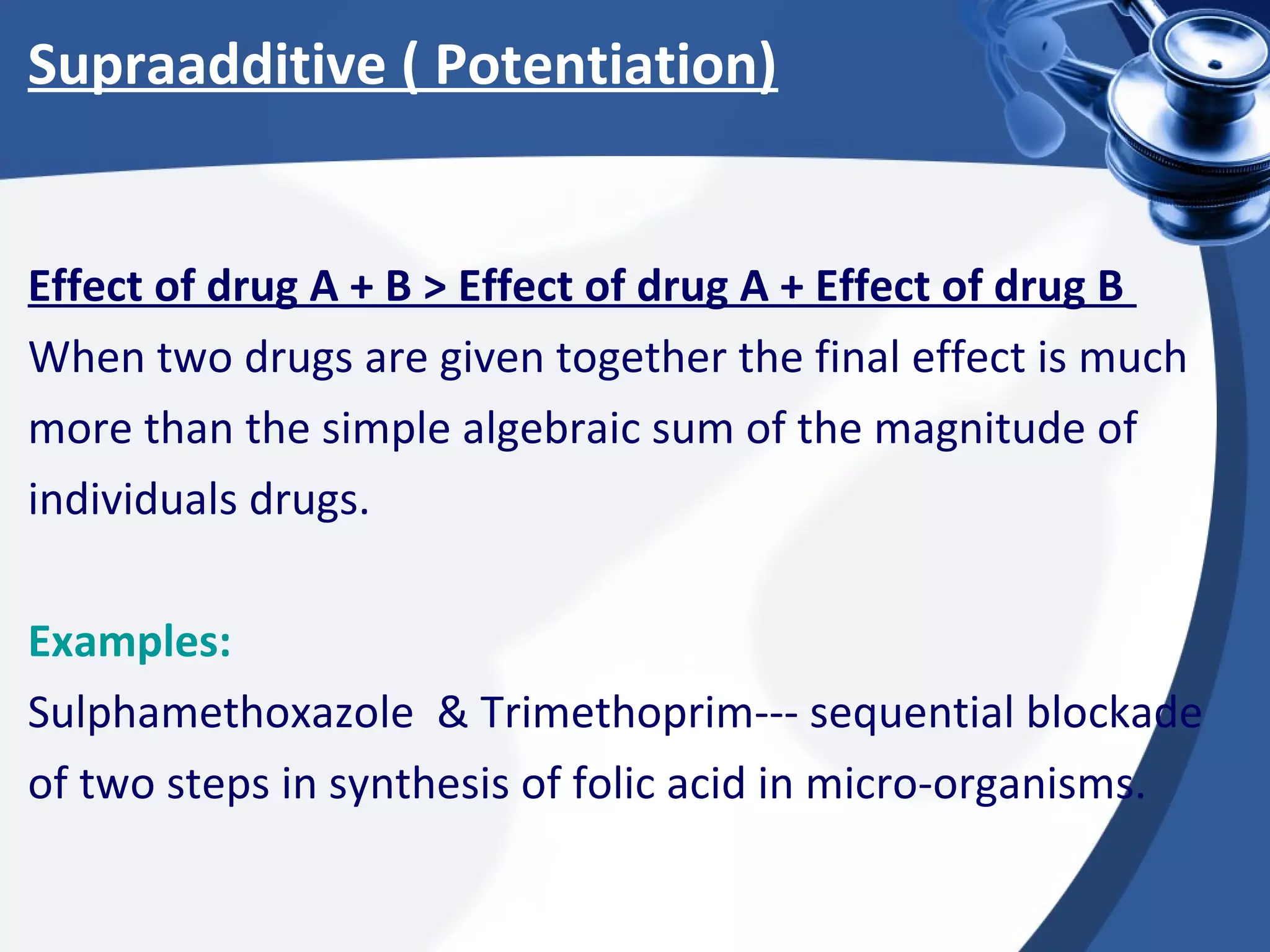


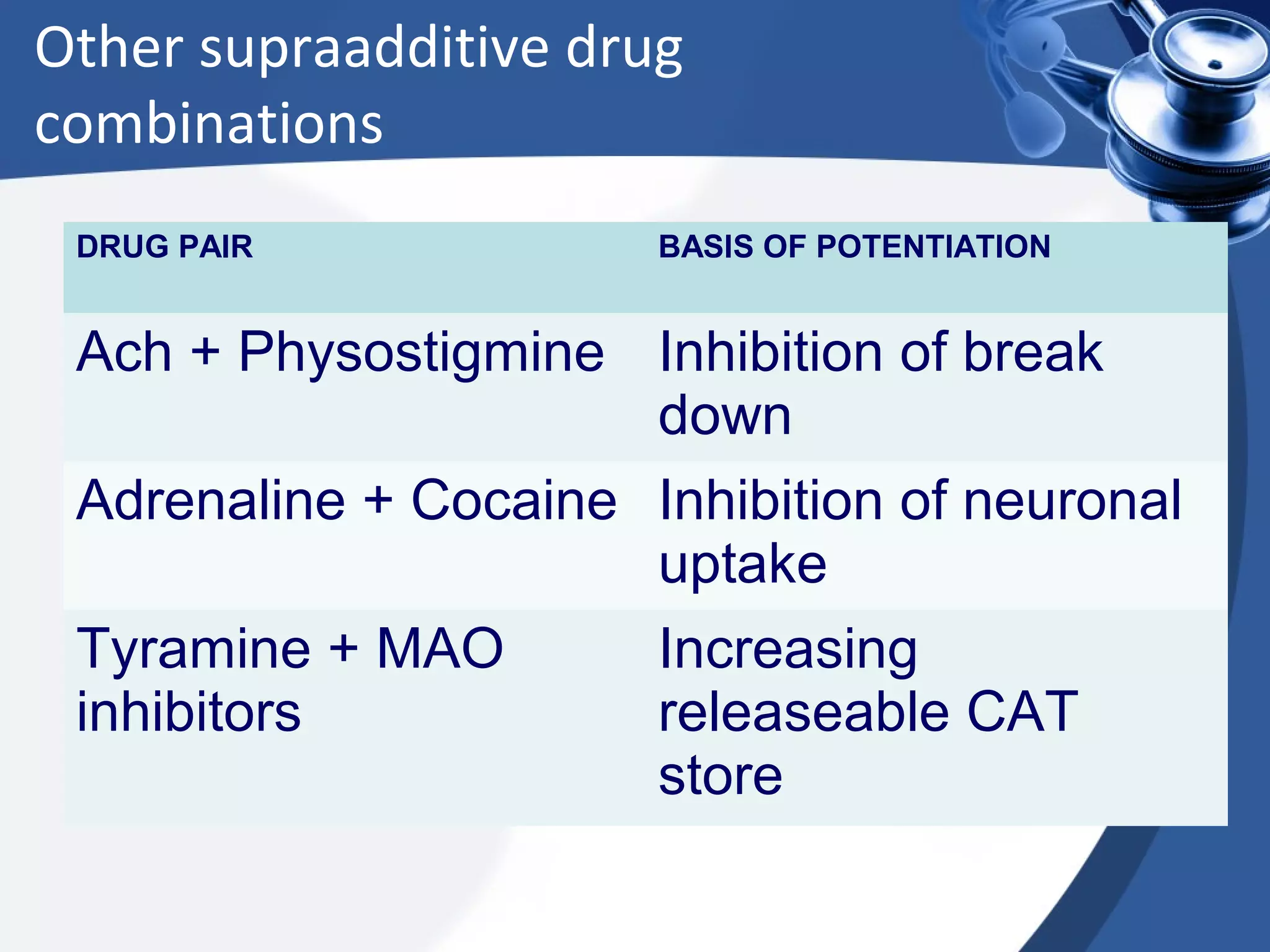



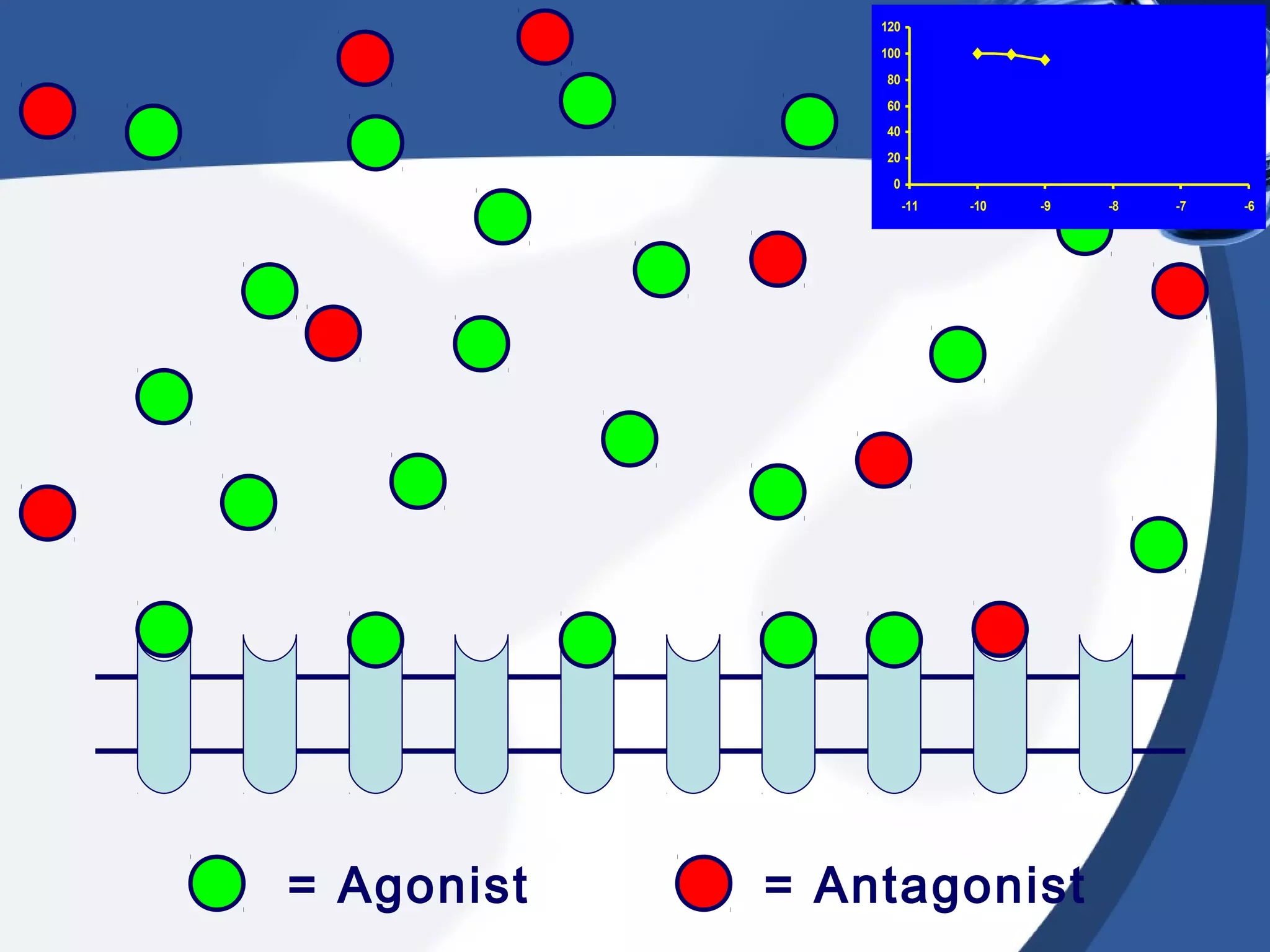

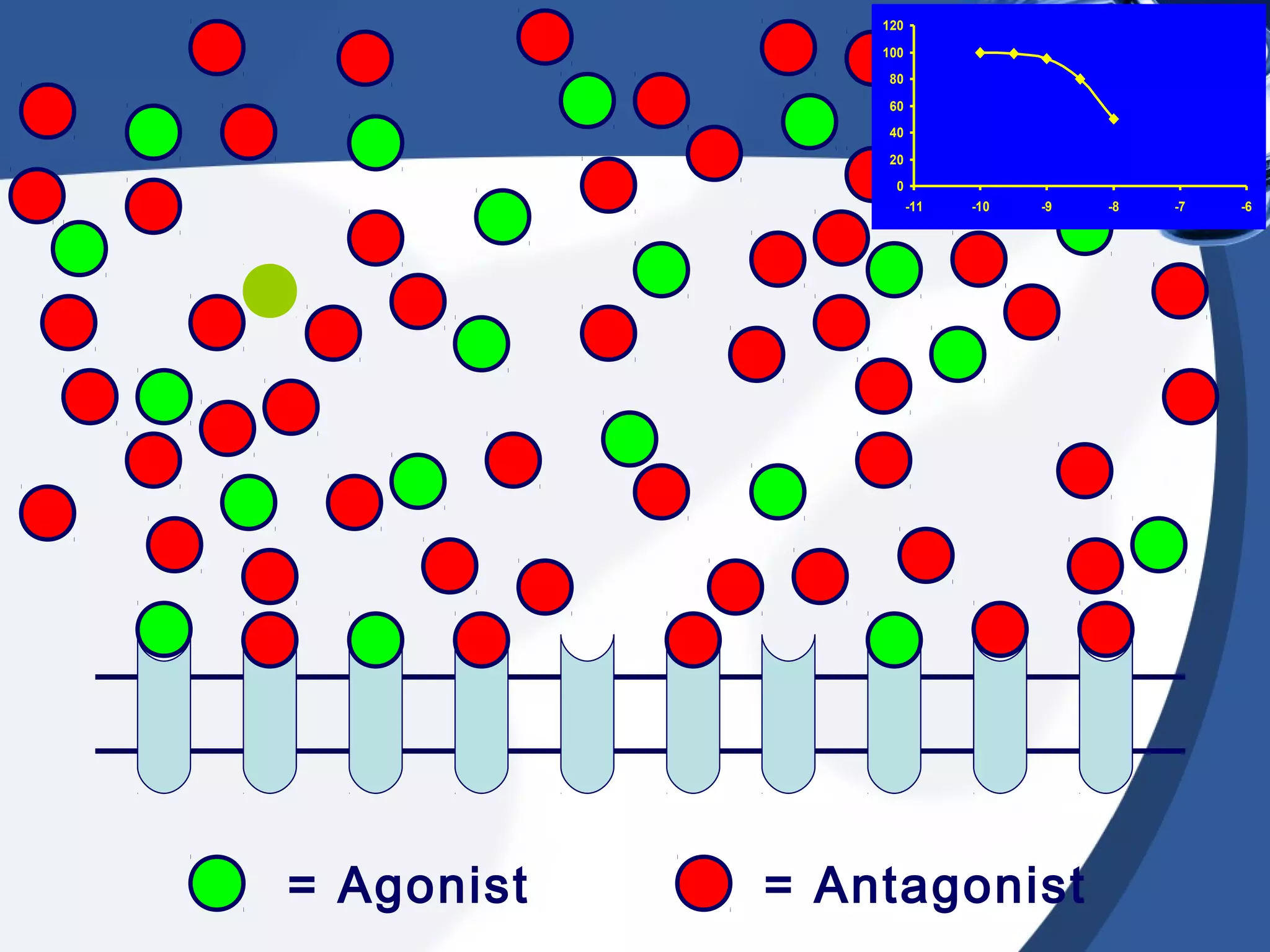

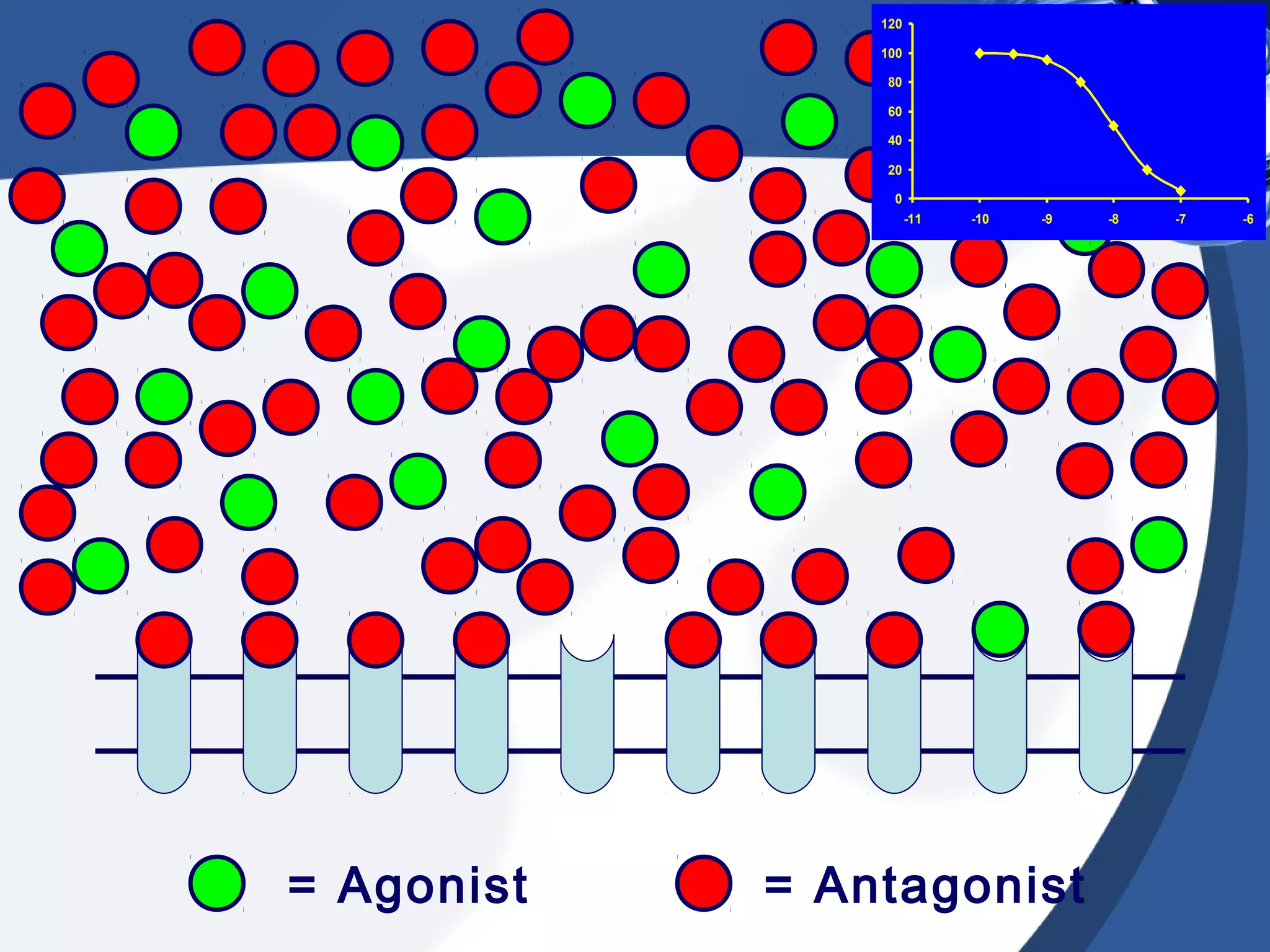
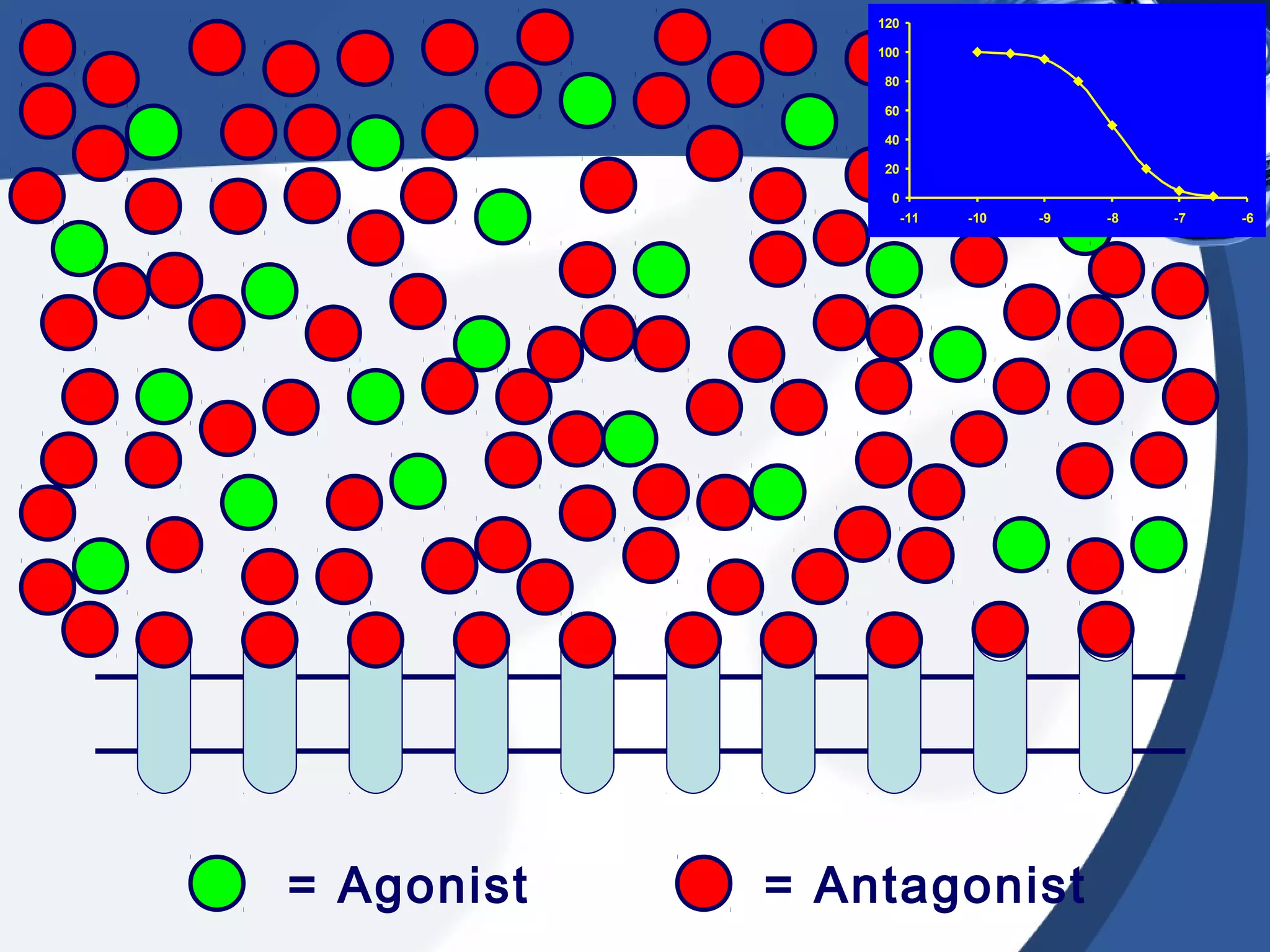
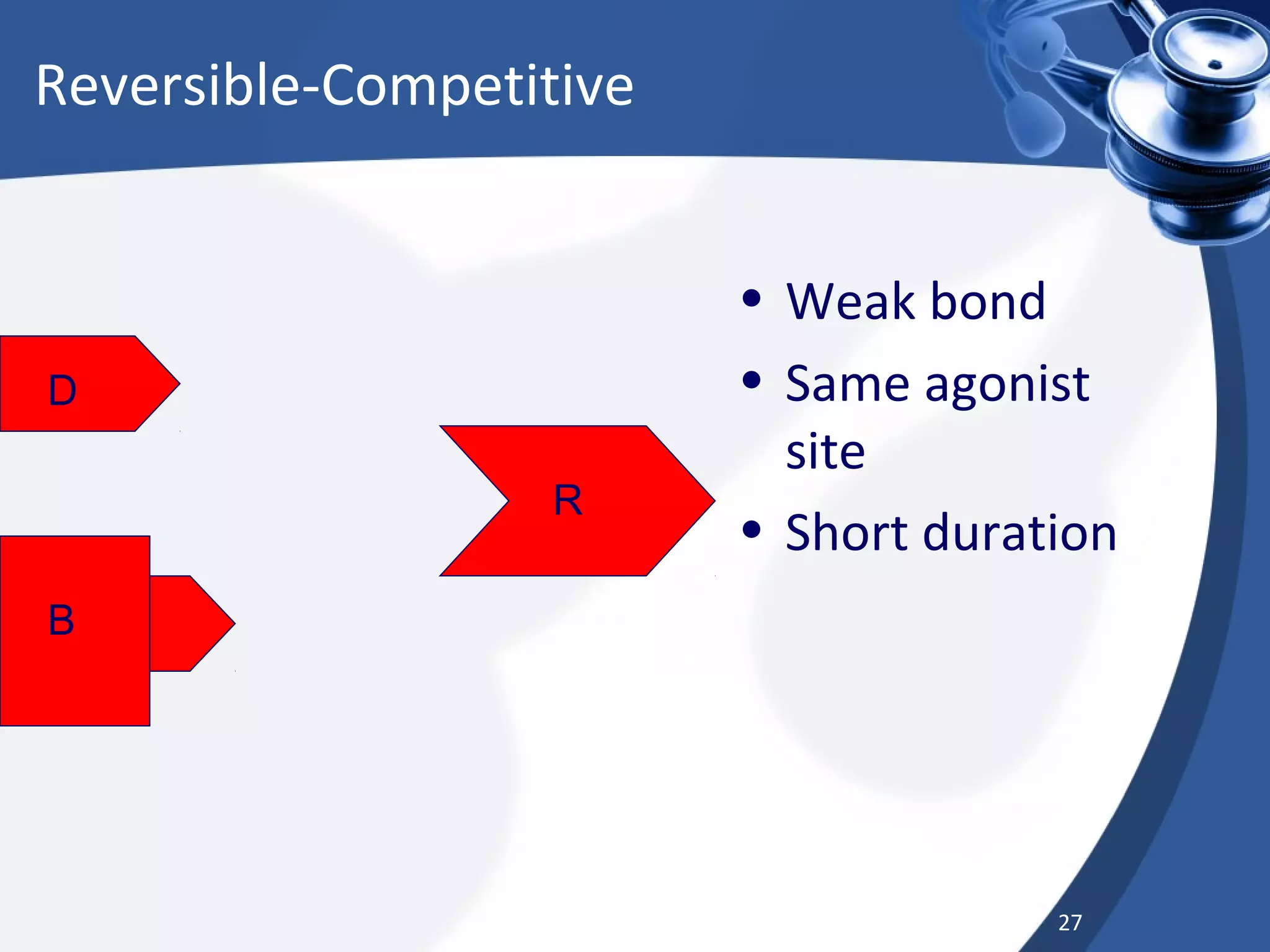
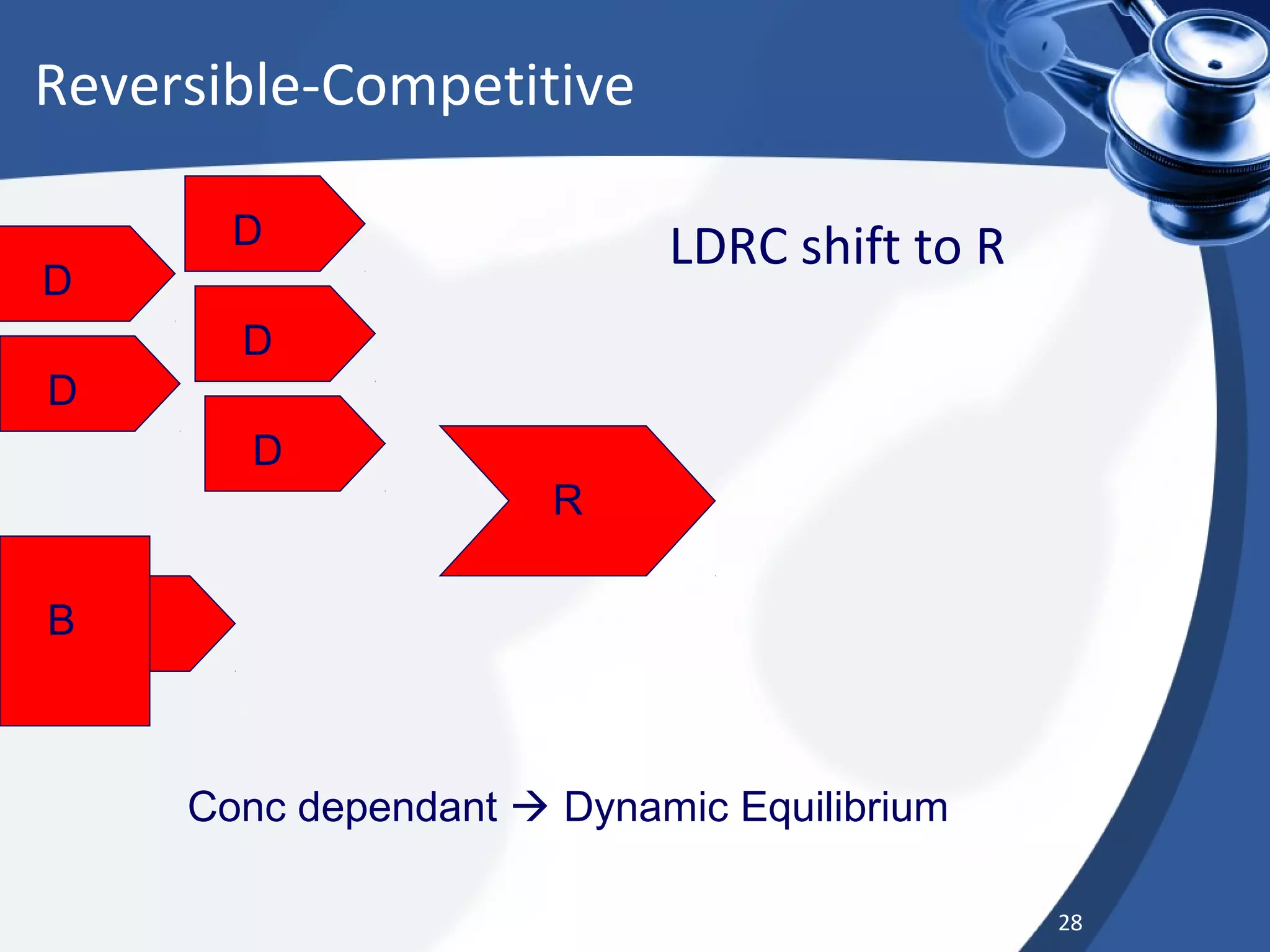
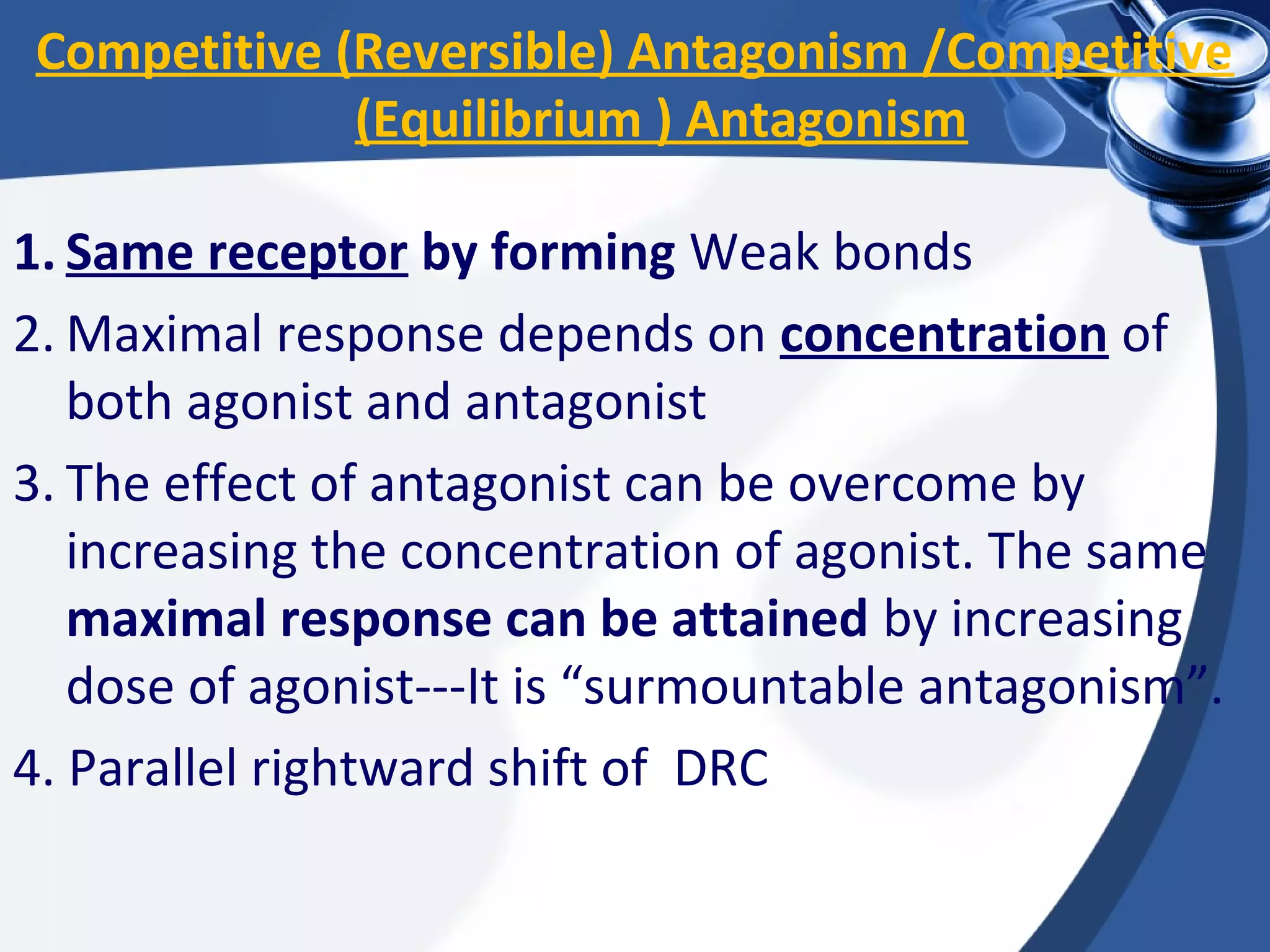

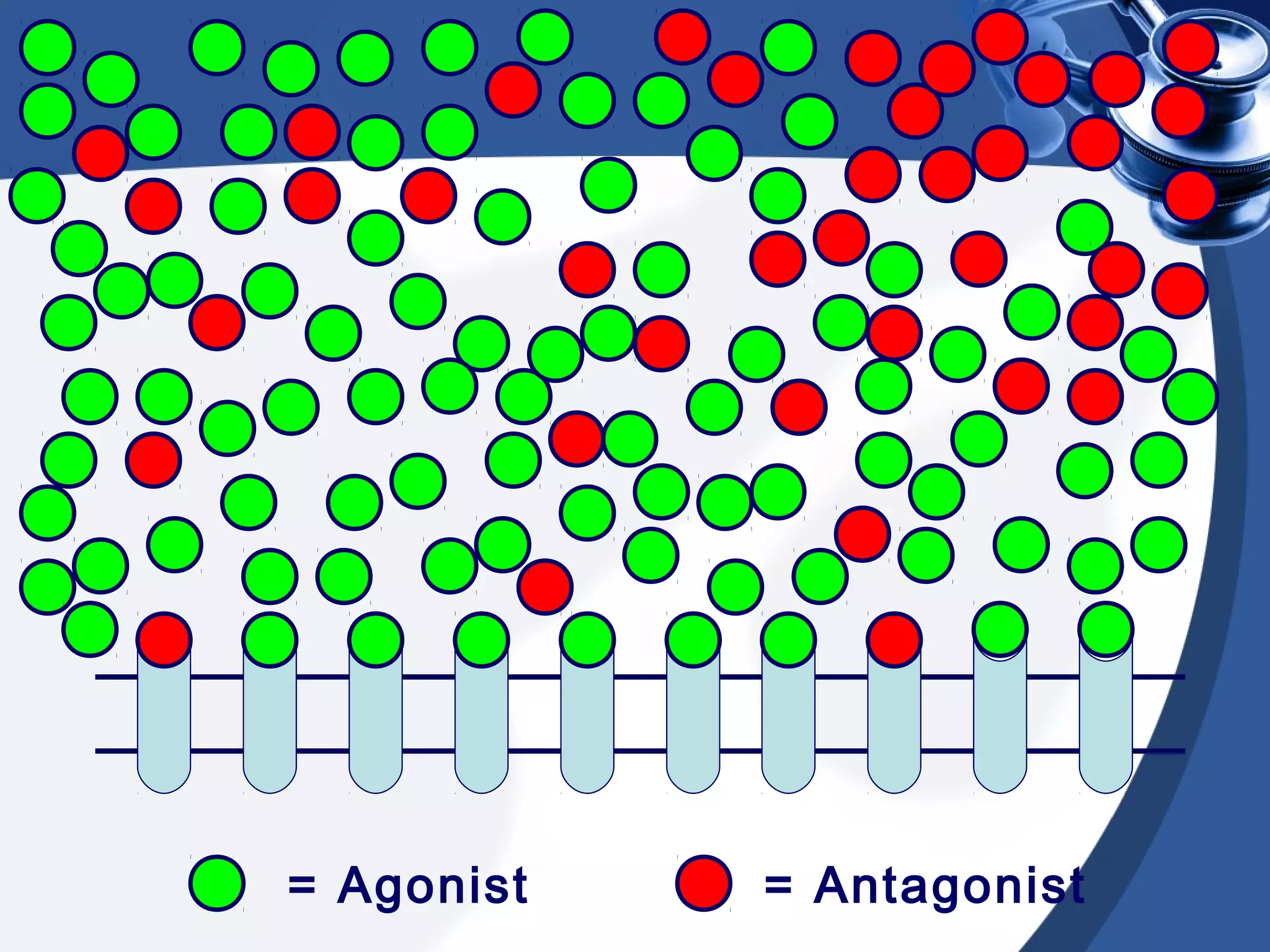



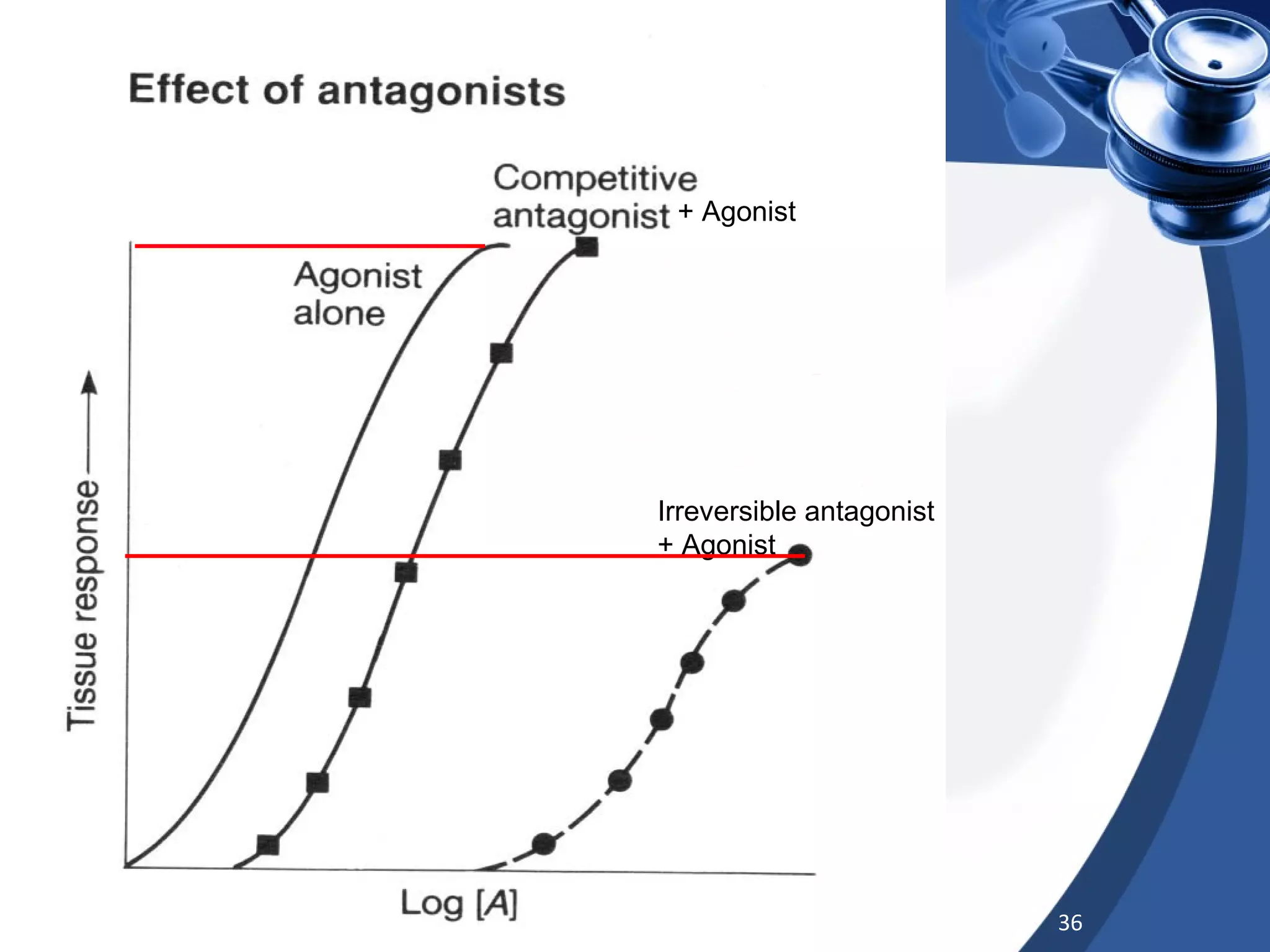



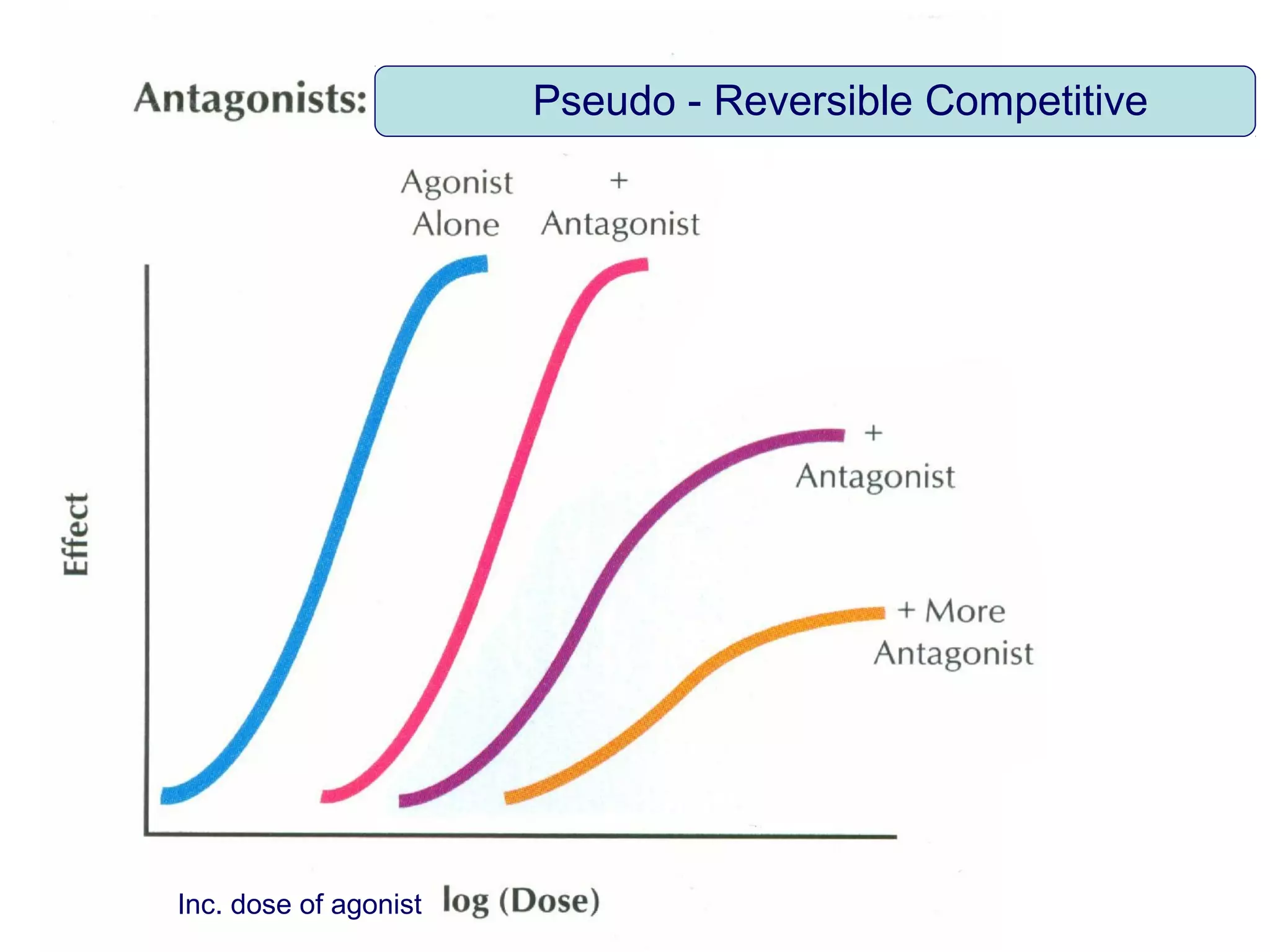



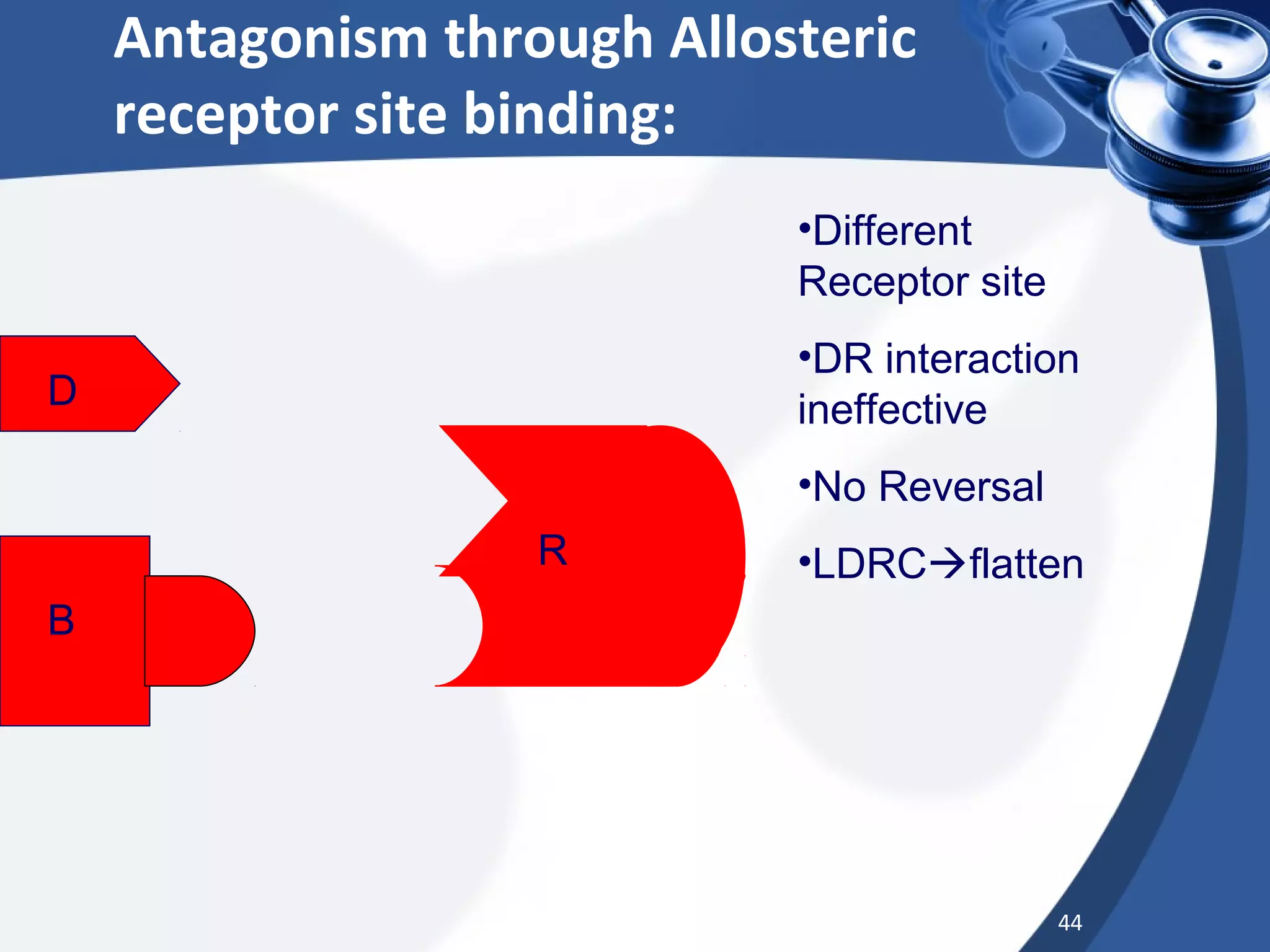

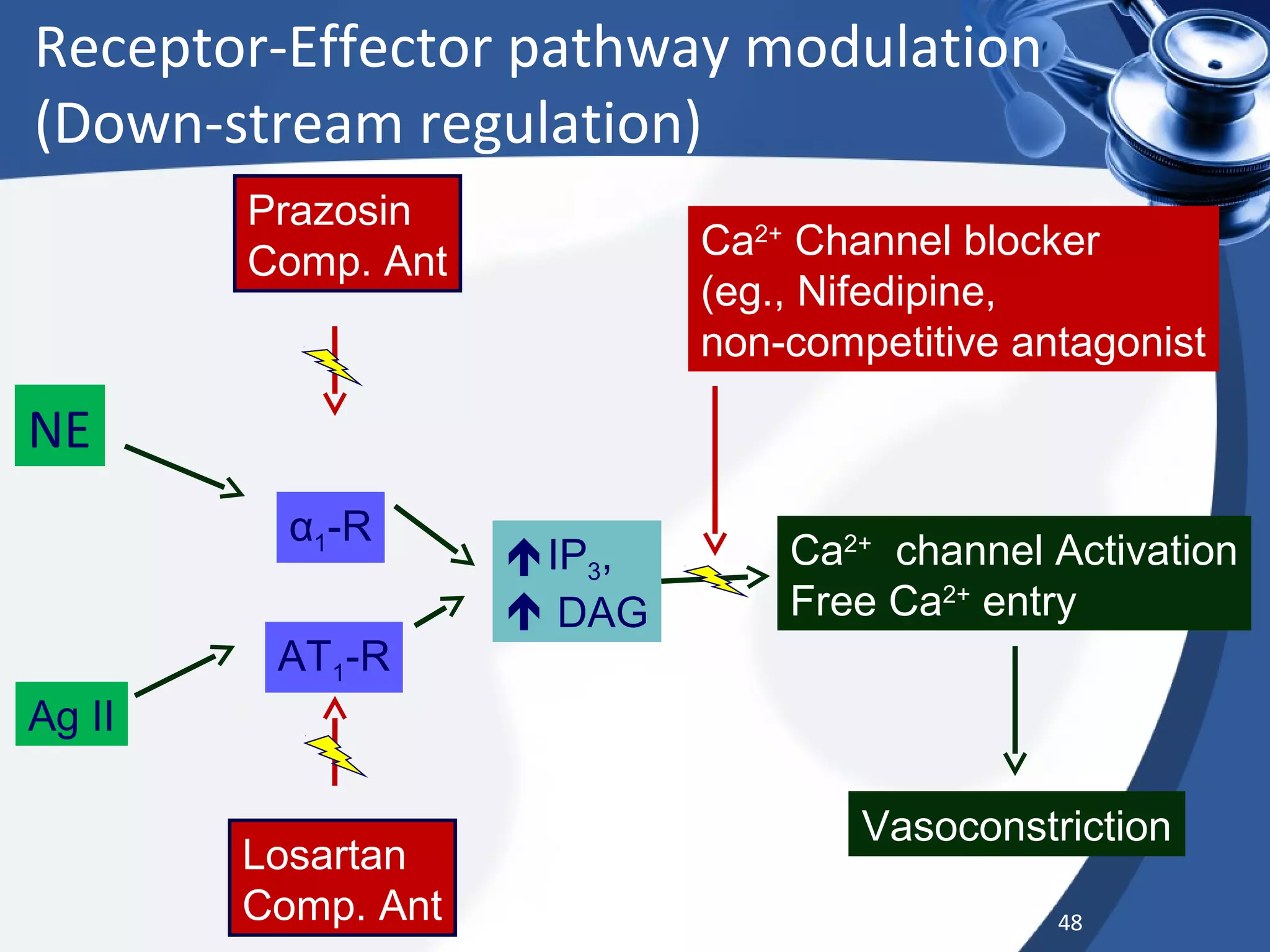

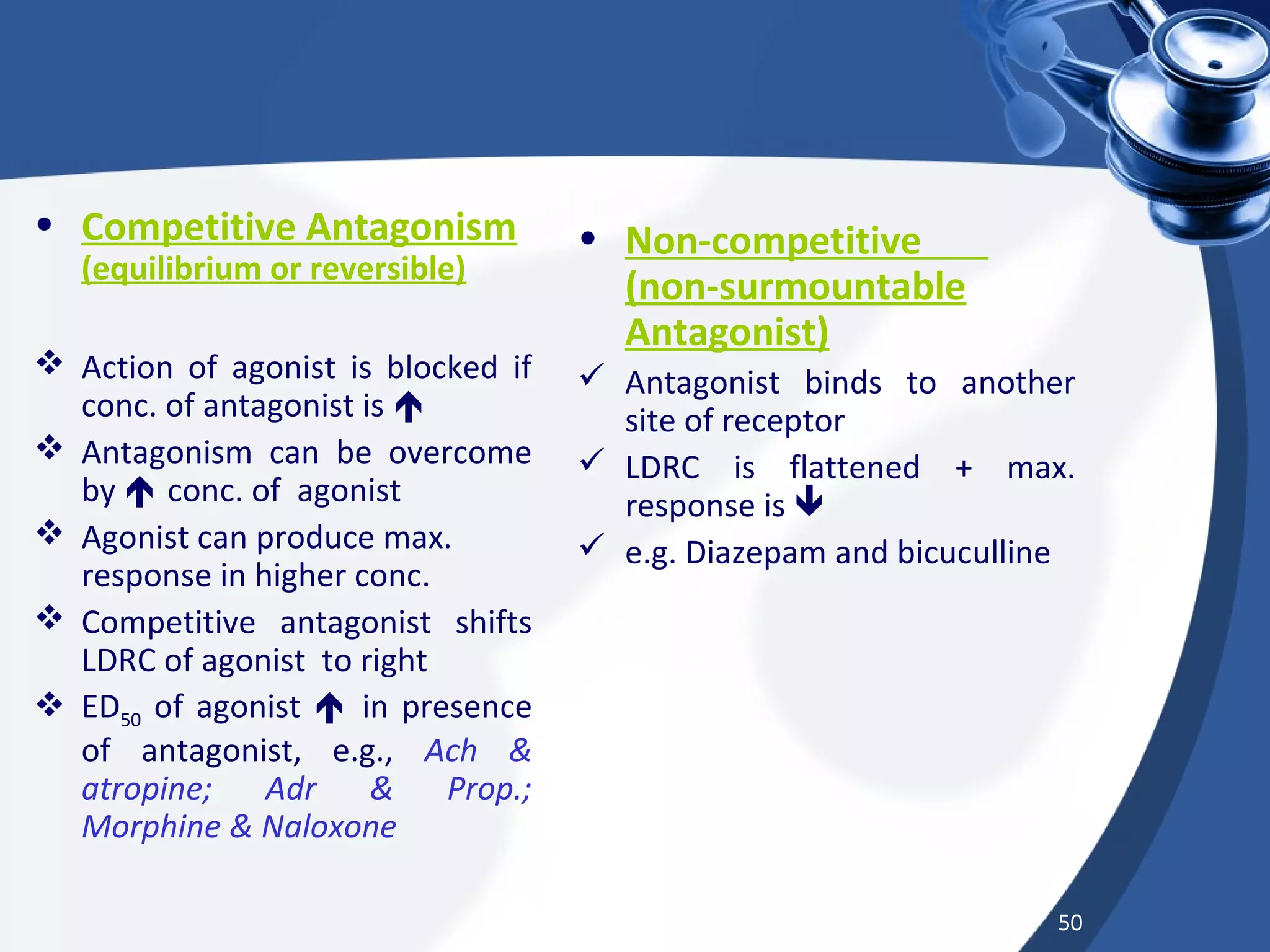




The document discusses different types of interactions that can occur when two or more drugs are taken together. It describes additive or summation effects when the effects of the drugs combine in an additive fashion. It also explains drug synergism, where the combined effect is greater than the sum of the individual drug effects. Additionally, it covers drug antagonism, where the combined effect is less than additive due to one drug opposing or decreasing the effects of another drug. The types of antagonism discussed include competitive, non-competitive, chemical, physiological, and physical antagonism.



































































