2. Differential Diagnosis of Cardiac Mass
Intra cardiac
Thrombus
Focal
myocardial
hypertrophy
Left Ventricular
noncompactio
n
Infectious
Disease
(abscess)
Primary
cardiac tumor
Secondary
Cardiac
Tumor(Metast
asis)
Lipomatous
Hypertrophy of
septum
Cyst
Imaging
Artefact
3. Classification
Benign Tumors Malignant Tumors Metastatic Tumors
Myxoma
Rhabdomyoma
Fibroma
Lipoma
Hemangioma
Papillary
Fibroelastoma
Cystic tumor of AV
node
Paraganglioma
Sarcoma
Lymphoma
Renal Cell Carcinoma
Melanoma
Breast Carcinoma
Lung Cancer
Sarcoma
Lymphoma
Leukemia
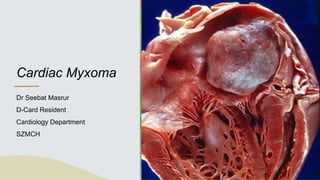
4. Introduction
• Cardiac myxomas are the most common neoplasm of the Heart.
• It can arise from any chamber of the heart, but left atrium is the most
commonly affected (75%), followed the right atrium (15-20%) and then the
ventricles (3-4%).
• Less commonly, myxomas are bi-atrial or multi-chamber in origin;
the latter may be part of the Carney Complex.
5. Introduction
• The clinical presentation of cardiac myxoma depends on their location, size and
mobility.
• Typically presented by the triad of intra-cardiac obstruction, embolization and
constitutional symptoms. Sometimes they may present with atypical features.
• Predominantly seen in females.
• Here, we present seven cases of cardiac myxomas occurring among Bangladeshi
population having originated from different cardiac chambers with different
morphological features and diverse clinical manifestations both typical and atypical.
7. Pathology
• Primarily composed of gelatin-like structure that contains
myxoma cells in a stroma composed of
glycosaminoglycans.
• Myxomas produce vascular endothelial growth factor which
is responsible for its enlargement size.
• Typical myxomas range between 1 to 15 cm in diameter.
• Around 30% of these tumors have a friable surface and can
embolize.
• Tumor does not invade myocardium.
8. Pathology
• Two-thirds represented as round to oval sessile
polypoid masses with a short, broad base attached
to the atrial septum and smooth or slightly
bosselated surface.
• One-third are soft and gelatinous with an irregular
surface consisting of papillary or finger like villi that
are prone to embolization.
• Calcification is common
• May be less than 1cm and be incidentally at autopsy
or exceed 10 cm and distend the atria.
• Over 90% occur in the region of the oval fossa.
9. Clinical Presentation
The clinical presentation of cardiac myxoma depends on their
location, size and mobility
Can be divided into four categories
1. Systemic manifestation
2. Embolic manifestation
3. Cardiac manifestation
4. Secondary Phenomena-Immunological and hematological
10. Symptoms
Early stages-No symptoms.
Later –Features of cardiac failure with
intracardiac obstruction(67%).
Signs of embolization(29%)
Immunological Manifestation of myalgia
Constitutional symptoms-Fever(19%),
malaise, weight loss etc
11. Symptoms
Exertional dyspnea commonly Platypnea (Difficulty
breathing in upright position, relieved by supine
position)
Paroxysmal nocturnal dyspnea
Dizziness
Fainting
Chest pain
Symptoms can often mimic mitral stenosis-fever,
joint pain , weight loss
12. Right Atrial symptoms
Right Atrial myxomas rarely
produce symptoms until they
have grown at least 5 inches
wide.
They can produce a clinical
picture of right sided heart
failure with signs and symptoms
of venous hypertension,
including hepatomegaly, ascites
and dependent oedema and
can cause tricuspid stenosis by
partially obstructing the orifice.
14. Cardiovascular Findings
Resembles mitral valve disease-
Loud S1Due to mobile myxoma causing delay in mitral valve
closure.
Stenosis Tumor plop/myxoma murmur due to Tumor prolapse into
the mitral orifice during diastole.
Regurgitation Injury to the valve by tumor-induced trauma.
Bi-basal crepitations incase of pulmonary oedema
15. Tumor Plop
• It is a high frequency early diastolic sound heard in left
or right atrial myxomas.
• The generation of tumor plop requires a mobile
myxoma attached to the atrial septum by a long stalk.
• It may be confused with OS or S3 as it occurs later
than OS and earlier than S3 , but intensity of TP and
diastolic rumble may vary with patient’s body position.
• The clinical features of atrial myxomas mimic those of
mitral value disease especially MS. However, often
symptoms are sudden, intermittent and related to the
patient’s body position.
• The right atrial myxoma may also have a diastolic
rumble, holosystolic murmur (of TR), elevated jugular
venous pressure with a prominent a wave and rapid y
descent.
16. Investigations
CBC-Anemia, High ESR
High CRP
High Gamma Globulin Level
ECG-Usually Normal, LAE, Arrhythmias
CXR-Features of CCF, Occasionally
calcific tumor may be visible
ECHO- DIagnostic
CT/MRI- Provide better delineation of
mass
17. ECHO is
confirmatory
Homogenous ECHO mass
filling LA attached to the
septum with a Stalk.
Tumor fills LA in systole.
Prolapses into mitral valve
orifice during diastole.
19. Management
Surgical excision through cardiopulmonary
bypass. Surgical mortality risk is less
than 5%.
No known medical treatment exists for atrial
myxoma. Drug therapy is used only for
complications such as congestive heart
failure or cardiac arrhythmias
This treatment is curative and only 1 to 2
% of sporadic cases recur.
Familial cases have a slightly higher
recurrence rate up to 20%.
20. Syndrome myxomas
Carney complex
NAME syndrome-
Nevi, Atrial
myxoma, myxoid
neurofibroma,
ephelides
LAMB syndrome-
Lentigines, atrial
myxoma, blue nevi
21. Carney
Complex/Syndrome
• 5-10% of patients with cardiac myxoma show a
familial inheritance and occur as part of the carney
complex
• Rare multiple neoplasia syndrome associated with
distinctive cutaneous lesions.
• Lentiginous skin pigmentation on 70- 80% of
patients.
• Association-Schwannoma
-Calcifying Sertoli cell tumors of the
testis
-Breast ductal adenomas
22. Take Home Message
• Myxomas are rare but the most common
of the benign cardiac tumors.
• Surgical resection is standard of care
regardless of tumor size.
• Surgery is very well tolerated with normal
life expectancy afterwards.
• Recurrence is uncommon but possible.