
Recommended
Recommended
More Related Content
Similar to Number of Pages 4 (Double Spaced)Number of sources 8Writi.docx
Similar to Number of Pages 4 (Double Spaced)Number of sources 8Writi.docx (20)
More from cherishwinsland
More from cherishwinsland (20)
Recently uploaded
Recently uploaded (20)
Number of Pages 4 (Double Spaced)Number of sources 8Writi.docx
- 1. Number of Pages: 4 (Double Spaced) Number of sources: 8 Writing Style: APA Type of document: Coursework Category: Healthcare Order Instructions: Comprehensive Article Review Caverly, T.J., Fagerlin, A, & Wiener, R.S. (2018, January 22). Comparison of observed harms and expected mortality benefit for persons in the Veterans Health Affairs Lung Cancer Screening Demonstration Project. JAMA Internal Medicine. 1. What research questions are addressed in this study and what is their purpose (5 points)? 2. What type of research design was used (experimental, quasi-experimental, correlational) in this study and what led you to your decision (5 points)?
- 2. 3. Are the instruments in this study valid and reliable, why or why not (10 points)? 4. Discuss the specific results of each of the ANCOVAs (analysis of covariance) done in this study. What was the purpose of"each" of the ANCOVAs? What was the covariate in each and why did they do an ANCOVA in each case (5 points)? 5. In the Tables, results are presented, Please explain the tables and summarize the results (15 points). 6. Explain, in simple language, any significant results of this study (25 points)? 7. Identify and discuss any threats to internal and/or external validity in this study (10 points). 8. If you could redesign this study correcting anything you have found wrong with the research, what would you correct and how would you do it (20 points)? Opinion
- 3. EDITORIAL Reducing Harms in Lung Cancer Screening- Bach to the Future Michael ln cze, MD, MSEd: Rita F. Redberg, MD, MSc TbeUS PreventativeServices Task Force cmrcntly recom- mends si:;ree ning (grade Brecommendation)for lung canc er witha nnuallow-dose computed tomo graph}' for high-risk in- dividuals ages55 to 80 years, defined as those having greate r gLblefor LCS using the Bach risk tool,11 a vaJidatcd risk model usingsex,age, smokingduration, durationof abstinence from smoking and number of cigarettes smoked per day as inpu ts. The asto undingly high ratesof false-pos itiveresults in the low- =Related attid e than a 30 pack-year cumula tivesmoking historyand h av• ing quit with in the past 15 years.1 The evide nce to sup- est risk quintiles (eg, 2221false-positive resul ts per lung ca n- cer death averted and a NNS of nearly 5600 in quintile1), as well as extremelylow ratesoflungcancerincidencein the low- est- risk groups, confirm trends illustrated in previous stud- port thisrecommendation overwhelminglycomes rrom the Na- tional Lung CancerScreenfngTrial(NL ST). While3 other large randomized clinical trials failed to show any mortality ben- efit tolung cancer screening (LCS), the NLST demonstrateda 20% reduction in lungcan ce r mortality,a lo ng with a 6.7% re- duction in .ill-ca use mortality, when compared with an an- nual chest radiograph, witb a number needed toscreen (NNS} of256to prevent I lung-cancerassociated death over3years.-2 5 Real-
- 4. worldapplication ofLCS has been particularly chal- lenging, w ith evidence of inappropriate U.% in low-risk per- sonsalong with very high rates.o fincidental lindings a.nd false - positive resultsleadiag to a muchhigher harm o benefit ratio than what was seen in randomized clinical trials.·2 7 The most robust implementation data to date,conducted on alargehigh- risk population through the Veterans Health Administration system, dcmonstr.itc-0 that 56% of those screened had nod- ules requiring follow-up with repeated imaging and/or inva- siveprocedures, and 40%ha.d incidentalfindings,such asem- physema and coronary arte ry calcificatio, 11 with a relatively !ow cm ce r detection rate of 1.5% (even lower for early-stage ( - )cancers tbat mostbenefit fro m sc;r,eening).GTncreasing l y, there has beenconcern aboutboth the cost-effectiven essofLCSand the harms associated with screening, including high rates of incidentalfindings (resulting in unnecessary i.nvasive proce- dures and emotionalstress), as well as radiation ex posure (pos - sibly leading tosecondar y malignant neop!asm.7 9 1 hese flild- ings raise the question of whethe r a more targeted inclusion criteria maydecrease the total numberofpatientsscreened and the false-posi tivity ra te withoutsacrificingt.he mortality ben- efit seen in the NLST. It is against this background that Caverly ct al10 examine the impact of riskstratifying a real-world cohort of patientseli· ies and make lhe case for refined guidelines for LCS.1 .n This is es pecially salienti n light of recent evi dence suggesting t ha t bl,gh numbers oflow-riskindividuals arebeingscreenedin.real· world practice.7 Unfortunately, the useof LDCTscreeningevenin the high- est - risk quintiles isstill associated with alarm ingly high rates of false-positive results-302 false-positive resqJts for every lung cancer death prevented (NNS, 552), in addition to high rates ofincidental findingspotentiaUy req uiringinterven lion as noted
- 5. in theoriginalcohort study.6 Furthem1ore, while the author co rrectly poi.n,t out large differences in sc ree ning ef- ficacy and benefit to risk ratio between the highest and low- est risk quintiles, thedata are murkier in between, with greater than 500 false-positive res ults per lung cancer death pre- vented foraII b ut the highest-risk quintile, mea.ning th at most participants are exposed to an unfavorable benefit to risk ra- tio. Caverly et a.110 have made the important contribution of applying a validated risk stratification tool toa real-world co- hort to improve sc reening c rite ria. Other groups have retro- spectively demonstrated reduced hamis in stu dy popula- tions with novel1iskstratificationtoolsusingeasilyobtainable patient infomiation, such as em physema diag1l0s is, s moking history,age,sex,and family history.'2·' 3 However,dearly more work is needed to minimizethe harms of radiation eiq,osure, invasive procedure,sand emotionalstressundercurrentguide- Jines , while preservingbenefit for those whose livescould be saved by the early detection oflung cancer. Ifand howwe will get there has yet to be deterrni.necl, but one thing is d ear: the future of LCSdepends on our ability to reexamine and refine our approach to patient selection and clearly commun.icate risks and benefits of screening. ARTICLE INF ORMATION Author Afffliatlons: partmellt of Medicine, Uniot!rsityof C lifomia,S/ln Francisco. Schoolcl Medicine.SanFrancis.co (rncre,Redberg}:l:di tor, JAMA lntemcl Medi6ne (Re<Jberg). Corrcspondnl g Author: AltaF.Re<lbcrg, MO, MSc, Departm I of Medicine, Universrtyof Calirorni a, Sa11Fralldsm,5d1oolof Medicine, 505 f>amassus, M i l 80 , SanFrancisco, CA9414 3·0124-(r it a.redberg @ucsf.edu).
- 6. f>ubllshedOnHnc : January22. 20 18 . doi:10.1001/ Jan; ainternrni:d.20T7.8217 Conflict ofl nterest Di.sdosur : Nooe l'<!p<,rted. Jamaintemalmedidne.comJAMA l llt .ern alMed[dnc Publishedonline Janua1y 22,2018 El © 2018 American Medical Association. All rights reserve,d. Letters RESEARCHLETTER LESSISMOREComparison of Observed Harms and Expected Mortality Benefit for Persons in the Veterans Health Affairs Lung Cancer Screening Demonstration Project The Veterans Health Affairs (VHA) lungcancer screening (LCS) demonstration project identified a much higher false- positive rate following initial low-dose computed tomo- graphic screening than did the National Lung Screening Trial Next, we separated patients into risk quintiles and as- sessed for each: number of LC cases observed; screening ef- fectiveness (number needed to screen[NNS] per LC death pre- vented); and screening efficiency (number of false-positive result s and downstream diagnostic procedures [eg, ad- vanced imaging, bronchoscopies,biopsies] per LC death pre- vented). Following
- 7. VHA policy and as part of the VA Quality Enhancement Research Initiative, thisevaluation was not con- sidered to be researchand wasdeclared to benonresearch qual- ity improvement activities by the VHA National Center for Health Promotion and Disease Prevention , and the Ann Ar - =Editorial (58.2% VS 26.3%).1•2 Most false -positive result s (nod- ules not confirmed to belung bor Veterans Affairs Medical Center institutional review board. Asa quality improvement activity, patient consent was not re- quired. Patient data were deidentified in analyses. cancer [LC]after follow-up) resulted in repeated imaging, but 2.0% of people screened also required nonbeneficial down- stream diagnostic evaluation to determine these noduleswere not cancer.2 We sought to put these findings into context by examining how this high false-positive rate influences the harm- to-benefit ratio for higher- vs lower-risk patients. Methods I From March 31, 2015, through June 30, 2015, 2106 patients were screened across 8 academic VAs. Screening processes and population-average outcomes for this project have been reported.2 In trials, LCS's 20% relative risk reduc- tion (RRR) in LC mortality did not vary by baseline LC risk,3 so we estimated each patient's absolute risk reduction (ARR) by multiplying the 20% RRR by their baseline LC mortality risk (ARR = Baseline Risk x RRR). We estimated annual baseline LC mortality risk using the Bach risk model. 4 Unlike other models, the Bach mo del's inputs are obtainable in VHA's Corporate Data Warehouse. In addition, a recent analysis indicates it is one of the best performing models.s Results I Patients in higher quintiles of LC risk had signifi-
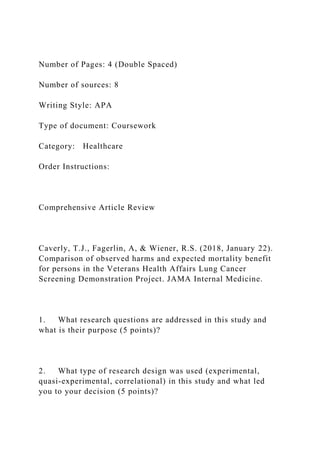
- 8. cantly more lung cancers diagnosed during the project, sup- porting the Bach model's ability to risk stratify in this popu- lation (Figure, A: 4.8 LCs per 1000 in quintile 1 vs 29.7 per 1000 in quintile 5). Initial screens were least effective for veterans in quintile 1 (lowest LC risk) (NNS of 6903) and most effective for vete rans in quintile 5 (NNS of 687) (Figure). Rates of false-positive results and downstream evaluations did not differ significantly across risk quint iles (P= .52 and P = .15 for trend, respectively). That is, the over- all 56.2% rate of false-positive results requiring tracking remain ed relatively stable across risk quintiles (95% CI, 53.1%-62.6% in quintile 1 vs 51.9%-61.5% in quintile 5), as did the overall 2.0% rate of false-positive results requiring downstream diagnostic evaluations (95% CI, 0.3%-2.6 % in quintile 1 vs 1.7%-5.2 %). This relationship of increasing absolute benefit and relatively stable harms enhances the favorable harm vs benefit balance for higher-risk vs lower- risk per so ns. The initial screen was leas t efficient for Figure. Observed Rateof Lung cancer Diagnosis and Predicted Effectiveness WithInitial Low-Dose Computed Tomography Screening 0 Observedrate of lung cancer diagnoses [!} Screeningeffectiveness ( 50 P = .004 z ci
- 9. 40 0 0 0 30 0. § 20 . " 3 ' 10 u T,i ) ( P < .001 )8000 "' 7000 6000 u 5000 40 00 Ql Q2 Q3 Q4 QS
- 10. li_ 3000 0 ;:,:; 2 000 z z 10 0 0 0 QI Q2 Q3 Q4 Q5 A.Observed rateof lungcancer diagnoses (per 1000persons screenedonce). B. Screening effectiveness: number needed to BaselineLung Cancer Risi< Quintile BaselineRisk Quintile screen(NNS) to prevent1lungcancer death. Error barsindicate 95% Os. jamainternalmedicine.com JAMA Internal Medicine Published online January 22.2018 El © 2018 American Medical Association. All rights reserved. Downloaded From: by donna hammaker on 02/17/2018 Letters Table. Outcomes of Initial Low-DoseComputed Tomography Screening According to Risk Quintile No.(%) Predicted' LC Deaths Efficiency Calculation
- 11. (No. of Harms per LCDeath Observed (During VHA Demonstratio n Project) Prevented) ( Quintile of Risk FPs Requiring Nonbeneficial FPS per LC Diagnostic Risk LC ' ) Participants• Casesb,c Tracking Diagnostic Evalua ti on Total, No.' P revented,No.' De a h t Prevented ' Evaluations per
- 12. LC Allquintiles 2084 (100) 31 (100) 11 7 5 (100) 42 (100) 7.97 1.59 737 26 Quintile 1 420 (20.2) 2 (6.5) 243 (20.7) 6 (14.3) 0.45 0.09 2749 68 Q u n i til e 2 459 (22.0) 2 (6.5) 249 (21.2)
- 13. 5 (11.9) 1.07 0.22 1152 23 Quintile 3 379 (18.2) 5 ( 16 .1) 205 (17.4) 8 (19.0) 1.29 0.26 793 31 Quintile 4 422 (20.3) 10 (32.3) 249 (21.2) 9 (21.4) 2.0 0.40 622 22 Quintile 5 404 (19.4) 12 (38.7) 229 (19.5) 14 (33.3) 3.16 0.63
- 14. 36 3 22 )(1-y Cumu lative Observed LC FPs Requiring DeathPrevented' Abbreviations: FP, false-positive screening result; LC. lungcancer; VHA, Veterans Health Administration. · Based on lung cancer risk prediction model of Bach etal.4 which uses the followinginputs to calculate anindi vidual's1- year cumulative risk of LC: sex, age, smoking status (current/formersmoker), years since quitting if former smoker. mean number cigarettes per day while smoking, andasbestos exposure. Asbestos exposure wasnot available for participants and wasnot considered in these calculations. The Bach model has been shown to have excellent predictivenesswithout this variable.3·5 For example. theBach model (in the absence of asbestos exposure information) showed satisfactory calibration and excellent discriminativeability inarecent external validation study (areas under curves of O 68 to 0.8for predictingLCdeath ).5 bTwenty-two of the 2106 participants hadincompletesmokinghistory and wereexcluded fr om thisanalysis. 'P < .05 by linear test of trend for continuousoutcomes.
- 15. patients in quintile 1 (2749 false-positive results and 68 non- beneficial diagnostic procedures per LC death prevented) and most efficient for t hose in quintile 5 (eg, 363 false- positive results and 22 nonbeneficial diagnostic procedures per death prevented) (Table). Discussion I The high rate of false-positive resultsidentified in the VHA's LCSdemonstration project hascaused concern about whether LCS sho uld be implemented in this population. We reex amined these data and found that the high false-positive rateresults ina more concerning harm-to-benefitratiofor those eligible persons at lower LC risk, but a much better harm -to- benefit ratiofor high-risk patients (Table). Wefound that even given these very high false-posit ive rates, the overall balance of prosand consamong patients at highLC riskstillsurpasses those of most established cancer screening programs. These results should be interpreted with several caveats in mind.The high rateoffalse-positive results found in the VA demonstration project may represent a substantial overesti- mate offuture ratesfor 2 reasons: (1) initial screens likely have more false-positive resu lts than recurrent screening, and (2) newer nodulemanagement guidelines areshowing great prom- ise in loweringfalse-positiverates.6 Reducing the rateoffalse- positive findings would improve the harm-to-benefit balance for all quintiles. However, our analysis did not include all po- tential harms ofLCS, such as overdiagnosis and psychologi- cal effects from false-positive results. In addition, effective- nessstudies arestill needed to confirm the extent towhich the mortality benefit observed in the National Lung Screening Trial, a 20.0% reduction in lung cancer and a 6.7% reduction in all- cause mortality,1 applies in actual practice. These real-world findings reinfo rce the need to risk- stratify patients for LCS and provide support for personal- ized, risk- based harm-benefit estimates for all eligible per- sons during LCS de cision-making. Tanner J. Caverly, MD, MPH
- 16. Angela Fagerlin, PhD Renda Soylemez Wiener, MD, MPH Christopher G. Slatore, MD, MS Nichole T. Tanner, MD, MSCR Shira Yun, MD Rodney Hayward, MD Author Affiliations: VACenter for Clinical Management Research. Ann Arbor. Michigan (Caverly, Yun. Hayward): University of Michigan Medical School. Ann Arbor (Caverly. Yun. Hayward);Institutefor HealthPolicy Innovation. University ofMichigan. AnnArbor (Caverly, Hayward); VASalt Lake Oty Center for Informatics Decision Enhancement and Surveillance (IDEAS). Salt Lake City. Utah(Fagerlin); University ofUtah Schoolof Medicine. Salt Lake City (Fagerlin); Center for Healthcare Organization and Implementation Research. Edith Nourse Rogers Memorial Veterans Affairs Hospital, Bedford, Massachusetts (Wiener); Boston University School of Medicine, Boston. Massachusetts (Wiener); VA PortlandHealth Care System Center to Improve Veteran Involvement in Ca,re Portland. Oregon (Slatore);Oregon Health & Science University School of Medicine. Portland(Slatore); Health Equity and Rural OutreachInnovation Center (HEROIC). Ralph H. Johnson Veterans Affairs Hospital,Charleston,South Carolina (Tanner); Medical University of South Carolina. Medicine. Charleston (Tanner). Corresponding Author: Tanner J. Caverly. MD.MPH. VACenter for Clinical Management Research and Universityof Michigan MedicalSchool. 2800 Plymouth Rd. Building 16. Room 321. Ann Arbor. Ml 48109 ([email protected] .umich.edu). Accepted for Publication: November 27, 2017. Published Online: January 22,2018. doi:10.1001/jamainternmed.20178. 170 Author Contributions:DrCaveryl had fullaccess to allof the data in thestudy and takes responsibility for theintegrity of thedata and the accuracy of the data analysis.
- 17. Study concept and design: Caverly,Fageriln, Siatore, Yun, Hayward. Acquisition. analysis. orinterpretation o fdata:Caverly. Wiener. Tanner. Yun. Hayward. Drafting of themanuscript:Caverly. Criticalrevisionof the manuscript forimportant intellectual content: All authors. Statistical analysis:Caverly.Hayward. Obtained funding: Caverly. Administrative.technical, or material support: Caverly,Yun. Studysupervision:Caverly. Fagerlin. Conflict of Interest Disclosures: Nonereported. Funding/Support:Funding for thisstudy was provided by the US Department of Veterans Affairs (VA) Quality Enhancement Research Initiative.Dr caverly is E2 JAMA InternalMedicine Published online January 22, 2018 © 2018 American Medical Association. All rights reserved. jamainternalmedicine.com Downloaded From: by donna hammaker on 02/17/2018 Comprehensive Article Review Caverly, T.J., Fagerlin, A, & Wiener, R.S. (2018, January 22). Comparison of observed harms and expected mortality benefit for persons in the Veterans Health Affairs Lung Cancer Screening Demonstration Project. JAMA Internal Medicine. 1. What research questions are addressed in this study and what is their purpose (5 points)?
- 18. 2. What type of research design was used (experimental, quasi- experimental, correlational) in this study and what led you to your decision (5 points)? 3. Are the instruments in this study valid and reliable, why or why not (10 points)? 4. Discuss the specific results of each of the ANCOVAs (analysis of covariance) done in this study. What was the purpose of"each" of the ANCOVAs? What was the covariate in each and why did they do an ANCOVA in each case (5 points)? 5. In the Tables, results are presented, Please explain the tables and summarize the results (15 points). 6. Explain, in simple language, any significant results of this study (25 points)? 7. Identify and discuss any threats to internal and/or external validity in this study (10 points). 8. If you could redesign this study correcting anything you have found wrong with the research, what would you correct and how would you do it (20 points)? Risks of Lung Screening Seen Outweighing Benefits in Many with Smoking History Very high false-positive screening rate seen in Veterans Affairs study Real-world findings from a Veterans Affairs (VA) population reinforce the need for personalized decision-making about lung cancer screening using validated risk-stratification models. Using the Bach risk tool for assessing lung cancer risk in veterans screened at eight academic VA centers (MSKCC, 2018), nearly 5,600 veterans in the lowest risk quintile needed
- 19. to be screened to prevent one lung cancer death. Meanwhile, the number of false-positive cases per death averted was 2,221. See generally Caverly, Fagerlin, & Wiener, 2018. Patients in the highest quintiles of lung cancer risk had significantly more lung cancers diagnosed supporting the model's ability to stratify risk in this population. These findings, recently published in the Journal of the American Medical Association Internal Medicine (Caverly et al., 2018) bolster those from a VA screening trial published last March (Kinsinger et 1 Letters coinvestigatoronaresearch grant fromGenentech·s Corporate Giving Scientific Project Support Program that isunrelated to this study andunrelated to any Genentechor Rocheproducts. No other disclosures are reported. Roleof theFunde/rSpon sor: The funding sourceshadnorolein thedesign and conduct of th e study: colleciton.management. analysis. and interpretationof the data: preparation. review. or approval of themanuscript: and decision to submit the manuscript for publication. Disclaimer: Allauthors were employees of the VA at the timethis work was conducted. The viewsexpressed inthis article are those of the authors and do not necessarily represent the views of the VA or the US Government. Meeting Presentation:Anearlier version of this work was anoral presentation at the 2017 Veterans Affairs Health Services
- 20. Research &Development (HSR&D)/ Quality Improv ementEnhancement Initiative (QUERI) National Conference: July 18-20. 2017: Arlington. Virginia. 1. Aberle DR, Adams AM. BergCD, etal,NationalLungScreening Trial Research Team.Reduced lung-cancer mortality with low- dosecomputed tomographic screening. N Engl J Med. 2011:36 5 (5):395· 409. 2. . Kinsinger LS. Anderson C.Kim J. etal.Implementationof lungcancer screeningin the VeteransHealth Administration. JAMA Intern Med. 2017:177(3): 399 -406. 3. Kovalchik SA.TammemagiM.Berg CD. et al. Targeting of low-dose CT screening according to theriskof lung-cancer death. NEnglJ Med. 2013:369(3): 245-254. 4. . BachPB, Elkin EB. Pastorino U. et al. Benchmarkin g lungcancer mortality rates in current andformer smokers. Chest. 2004:126(6):1742-1749. 5. Ten Haaf K, JeonJ. Tammemagi MC. etal. Risk prediction models for selection of lungcancer screeningcandidates: aretrospective validation study. PLoS Med. 2017;14(4):e1002277. 6. Pinsky PF.Gierada OS. Black W. et al.Performance of Lung- RADS in th e National LungScreening Trial: aretrospectiveassessment. AnnInternMed. 2015:162(7):485-491.
- 21. jamainternalmedicine.com JAMA Internal Medicine Published onlineJanuary 22.2018 E3© 2018 American Medical Association. All rights reserved. Downloaded From: by donna hammaker on 02/17/2018
- 22. al., 2017), showing a very high false-positive rate associated with lung cancer screening. The false-positive rate in that population was around 58 percent, which was more than twice the false-positive rate seen in the National Lung Screening Trial (National Cancer Center, 2014). The U.S. Preventive Services Task Force recommends lung cancer screening with low-dose CT for high-risk people between the ages of 55 and 80, defined as having a greater than 30 pack- year cumulative smoking history and having quit within the past 15 years for those no longer smoking (grade B recommendation). In an editorial published with the current VA study, it was observed that the future oflung cancer screening "depends on our ability to reexamine and refine our approach to patient selection and clearly communicate risks and benefits of screening" (Incze & Redberg, 2018). The study cohort consisted of 2,106 veterans screened for lung cancer at eight academic VA centers during a 3-month period in the spring of 2015 as part of the Veterans Health Affairs Lung Cancer Screening Demonstration Project. Annual baseline lung cancer mortality risk was estimated using the Bach risk model, which is a validated tool calculating sex, smoking duration, duration of abstinence from smoking, and number of cigarettes smoked per day to estimate lung cancer risk. Participants were separated into risk quintiles and assessed for lung cancer cases observed, number needed to screen (NNS) per lung cancer death prevented, and number of false-positive results and downstream diagnostic procedures. The research found "that even given these very high false-positive rates, the overall balance of pros and cons among patients at high lung cancer risk still surpassed those of most established cancer screening programs" (Caverly et al., 2018). Supporting References
- 23. Caverly, T.J., Fagerlin, A., & Wiener, R.S. (2018, January 22). Comparison of observed harms and expected mortality benefit for persons in the Veterans Health Affairs Lung Cancer Screening Demonstration Project. JAMA Internal Medicine. Retrieved from https://jamanetwork.com/joumals/jamainternalmedicine/article- abstract/2599437?redirect=true Kinsinger, L.S. , Anderson C., Kim, J., Larson, M., King, H.A., Rice, K.L.Jackson, G.L. (2017, March 1). Implementation of lung cancer screening in the Veterans Health Administration. JAMA Internal Medicine, 1 77(3), 399-406. Incze, M., & Redberg, R. F. (2018, January 22). Editorial: Reducing harms in lung cancer screening- Bach to the future. JAMA Internal Medicine. Retrieved from https://app.jamanetwork. com/#page=issuesContainer Memorial Sloan Kettering Cancer Center (MSKCC). (2018). Lung cancer screening decision tool. New York, NY: MSKCC. Retrieved from https://www.mskcc.org/cancer- care/types/lung/screening/lung-screening-decision-tool National Cancer Center (NCI). (2014). National lung screening trial. Washington, DC: U.S. Department of Health and Human Services, National Institutes of Health NCI. Retrieved from https://www.cancer.gov/types/lung/research/nlst 2