
Recommended
Recommended
More Related Content
Similar to R E S E A R C H I N B R I E FThe effect of ambulation afte.docx
Similar to R E S E A R C H I N B R I E FThe effect of ambulation afte.docx (20)
More from audeleypearl
More from audeleypearl (20)
Recently uploaded
Recently uploaded (20)
R E S E A R C H I N B R I E FThe effect of ambulation afte.docx
- 1. R E S E A R C H I N B R I E F The effect of ambulation after cardiac catheterization on patient outcomes Sek Ying Chair MBA, PhD, RN Assistant Professor, The Nethersole School of Nursing, The Chinese University of Hong Kong, Hong Kong, China David R Thompson PhD, MBA, RN, FRCN, FESC Director and Professor of Clinical Nursing, The Nethersole School of Nursing, The Chinese University of Hong Kong, Hong Kong, China Shu Kin Li MBBS, FRCP Chief of Service, Department of Medicine, Pamela Youde Nethersole Eastern Hospital, Hong Kong, China Submitted for publication: 24 August 2005 Accepted for publication: 26 January 2006 Introduction Cardiac catheterization remains the most definitive procedure for diagnosis and evaluation of coronary artery disease
- 2. (Woods et al. 2005). Currently, cardiac catheterization has become a routine diagnostic procedure performed in many hospitals in Hong Kong. Although it can be performed through brachial, radial, or femoral arteries (Woods et al. 2005), the transfemoral puncture is the most common approach (Noto et al. 1991, Chair et al. 2003). However, because vascular complications occur in 0Æ43–5Æ8% of transfemoral cardiac catheterization patients (Noto et al. 1991, Lehmann et al. 1997, Chair et al. 2003), strict bed rest and immobilization of the catheterized leg have been consid- ered essential to reduce the risk of their development (Grossman 1980, Woods et al. 2005). The recommended bed rest duration after transfemoral cardiac catheterization varies from two to 24 hours (Baum & Gantt 1996, Chair et al. 2003). Many patients find it difficult to use the bedpan or urinal in the recumbent position during bed rest, more- over, studies reported that back pain severity increased with longer duration of bed rest after cardiac catheterization
- 3. (Barkman & Lunse 1994, Baum & Gantt 1996, Chair et al. 2003). Therefore, to obtain optimal patient outcomes, the length of bed rest duration after cardiac catheterization should be minimized. Aims The aims of this study were to compare patient outcomes of vascular complications, back pain, and urinary discomfort between patients ambulated at four and 12–24 hours (usual care) post-transfemoral cardiac catheterization. Methods Patients admitted for elective cardiac catheterization at a general hospital in Hong Kong Island were recruited to the study. Inclusion criteria were that patients should be ethnic Chinese, aged over 18 years, had no bleeding disorders, were not receiving anti-coagulant therapy within the previous 24 hours before the procedure, had no back pain, blood pressure <180/110 mmHg before the procedure and no complications developed during cardiac catheterization.
- 4. Patients were randomly assigned to either a control or experimental group according to a computer-generated random table of number. Patients in the experimental group were ambulated after four hours bed rest postcardiac catheterization, whereas patients in the control group were ambulated the morning after the procedure, 12–24 hours Correspondence: Sek Ying Chair, The Nethersole School of Nursing, The Chinese University of Hong Kong, Shatin, New Territories, Hong Kong, China. Tel: (852) 2609 6225, E-mail: [email protected] edu.hk � 2007 Blackwell Publishing Ltd 212 doi:10.1111/j.1365-2702.2006.01599.x after bed rest depending on the time the patient had the procedure completed during the day (usual care). The puncture site was assessed for vascular complications hourly for the first six hours then the next morning at 08:00 hours using the guidelines (Christenson et al. 1976).
- 5. Significant bleeding was defined as blood loss estimated at >100 ml, haematoma >5 cm in width or bleeding that led to further attempts to reestablish haemostasis by manual pres- sure, sandbag, or reinforcement of pressure dressing. For all patients, back pain was assessed at four hours, eight hours and the next morning at 08:00 hours after cardiac catheterization by using a visual analogue scale consisting of a 100-mm long line with the left anchor representing ‘no pain’, and the right anchor representing ‘the worst possible pain’. Urinary discom- fort was assessed at six hours after the procedure by use of a five-point Likert scale self-developed measurement consisting of four questions, a higher value referring to more urinary discomfort. The test–retest reliability of the urinary discomfort measurement on 18 subjects was significantly correlated (r ¼ 0Æ95, P < 0Æ001), and the Cronbach’s alpha was 0Æ876. Findings A total of 86 (male, n ¼ 41; female, n ¼ 45) subjects completed the study, 43 in each group with a mean age of
- 6. 63 years (SD ¼ 9Æ6, range 34–75). Fifty-six (65%) subjects had either received no formal education or were educated at elementary level, and eight (9Æ3%) had received a college education. Most (65Æ1%) subjects had a monthly family income <HK$8000 (approximately US$1000). Seventy-one patients (82Æ6%) were either retired or housewives. Table 1 shows that the two groups were not significantly different in age, gender, education level, and monthly household income. Occupation status was significantly different between the two groups (chi-square, P ¼ 0Æ009) with more retired subjects in the control groups but more housewives in the experimental group. There was no difference between the two groups on vascular complications. One subject in the control and none in the experimental group developed bleeding at the puncture site that required manual pressure to re-establish haemostasis (Fisher’s exact test, P ¼ 1). Repeated measures analysis of variance was used to evaluate the back pain experienced across time and between groups. There was a significant difference between the two groups at the three time intervals on back
- 7. pain intensity (F2,83 ¼ 9Æ80, P < 0Æ001) with the control group reporting more pain at each time interval. Moreover, the two groups also differed significantly on urinary discom- fort (t65Æ6 ¼ 3Æ24, P ¼ 0Æ006) with the control group experi- encing higher levels of urinary discomfort (Table 1). Table 1 Demographic and outcomes comparisons between groups Control (n ¼ 43) Experimental (n ¼ 43) P-value Statistical test used Age [years: mean (SD)] 63Æ2 (±9Æ7) 62Æ7 (±9Æ7) 0Æ816 t- Test Gender, n (%) Male 19 (44Æ2) 22 (51Æ2) 0Æ517 Chi-square Female 24 (55Æ8) 21 (48Æ8) Educational level, n (%) No formal education 11 (25Æ6) 12 (17Æ9) 0Æ729 Mann– Whitney U-test Primary school 16 (37Æ2) 17 (39Æ6) Secondary school 13 (30Æ2) 9 (20Æ9) University 3 (7) 5 (11Æ6) Monthly household income, n (%) £HK$8000 22 (51Æ2) 34 (79) 0Æ052 Mann–Whitney U-test HK$8001–$18 000 14 (32Æ6) 6 (14) >HK$18 001 7 (16Æ2) 3 (7)
- 8. Occupation, n (%) Retired 30 (69Æ8) 21 (48Æ8) 0Æ009 Chi-square Housewife 4 (9Æ3) 16 (37Æ2) Presently working 9 (20Æ9) 6 (14) Vascular complications, n (%) 1 (2Æ3) 0 (0) 1Æ00 Fisher’s exact test Back pain Four hours 1Æ55 0Æ97 <0Æ001 Repeated measure of ANOVAANOVA Eight hours 4Æ41 1Æ34 The next morning 4Æ01 1Æ77 Urinary discomfort 2Æ57 1Æ09 0Æ006 t-Test Research in brief � 2007 Blackwell Publishing Ltd, Journal of Clinical Nursing, 16, 212–214 213 Discussion Prolonged bed rest in the supine position is difficult for many patients who have undergone cardiac catheterization. Some patients complain of back pain and have the desire to move from side to side. Others complain of difficulty to urinate in a supine position. In this study, patients allowed to ambulate at
- 9. four hours postcardiac catheterization experienced signifi- cantly less back pain and less urinary discomfort, but did not experience any increase in vascular complications at puncture site. The average age, high unemployment rate, low education standard and low-income level of patients in this study was reflective of the study site which is less affluent than the general Hong Kong population Implications for practice The results suggests that early ambulation may play a substantial role in reducing back pain and urinary discomfort in post-transfemoral cardiac catheterization. Allowing pa- tients to get out of bed after four hours of bed rest following cardiac catheterization could be introduced into routine practice in Hong Kong, as it was found to be safe and might aid in promoting patient comfort without increasing the incidence of vascular complications. In addition, the shorter bed rest duration may reduce the nursing time needed for
- 10. administering analgesics or back rubs to relieve back pain. Early ambulation after cardiac catheterization may also reduce the nursing time needed for assisting patients to use urinal and bedpan during bed rest period after the procedure. References Barkman A & Lunse C (1994) The effect of early ambulation on patient comfort and delayed bleeding after cardiac angiogram: a pilot study. Heart & Lung 23, 112–117. Baum RA & Gantt DS (1996) Safety of decreasing bedrest after coronary angiography. Catheterization and Cardiovascular Diag- nosis 39, 230–233. Chair SY, Taylor-Piliae RE, Lam G & Chan S (2003) Effect of po- sitioning on back pain after coronary angiography. Journal of Advanced Nursing 42, 470–478. Christenson R, Staab E, Burko H & Foster J (1976) Pressure dres- sings and postarteriographic care of the femoral puncture site. Radiology 119, 97–99.
- 11. Grossman W (1980) Cardiac Catheterization and Angiography. Lea & Febiger, Philadelphia, PA. Lehmann KG, Feris ST & Heath-Lange SJ (1997) Maintenance of hemostasis after invasive cardiac procedures: implications for outpatient catheterization. Journal of American College of Cardi- ology 30, 444–451. Noto T, Johnson LW, Krone R, Weaver WF, Clark DA, Kramer JR & Vetrovec GW (1991) Cardiac catheterization 1990: a report of the registry of the society for cardiac angiography and interven- tions (SCA&I). Catheterization and Cardiovascular Diagnosis 24, 75–83. Woods SL, Froelicher ESS, Motzer SU & Bridges EJ (2005) Cardiac Nursing, 5th edn. Lippincott, Philadelphia, PA. Research in brief
- 12. 214 � 2007 Blackwell Publishing Ltd, Journal of Clinical Nursing, 16, 212–214 060 Reading and Writing Climate Change “Are Electric Vehicles Really So Climate Friendly?” Hans-Werner Sinn The Guardian November 25, 2019 Germany’s automobile industry is its most important industrial sector. But it is in crisis, and not only because it is experiencing the effects of a recession brought on by Volkswagen’s cheating on emissions standards, which sent consumers elsewhere. The sector is also facing the existential threat of exceedingly strict European Union emissions requirements, which are only seemingly grounded in environmental policy. The EU clearly overstepped the mark with the carbon dioxide regulation that went into effect on 17 April 2019. From 2030 onwards, European carmakers must have achieved average vehicle emissions of just 59 grams of CO2 per km, which corresponds to fuel consumption of 2.2 litres of diesel equivalent per 100 km (107 miles per gallon). This simply will not be possible. As late as 2006, average emissions for new passenger vehicles registered in the EU were around 161 g/km. As cars became smaller and lighter, that figure fell to 118 g/km in 2016. But this average crept back up, owing to an increase in the market share of gasoline engines, which emit more CO2 than diesel engines do. By 2018, the average emissions of newly registered cars had once again climbed to slightly above 120 g/km, which is twice what will be permitted in the long term. Even the most gifted engineers will not be able to build internal combustion engines (ICEs) that meet the EU’s prescribed standards (unless they force their customers into soapbox cars). But, apparently, that is precisely the point. The EU wants to reduce fleet emissions by forcing a shift to electric vehicles.
- 13. After all, in its legally binding formula for calculating fleet emissions, it simply assumes EVs do not emit any CO2 whatsoever. The implication is that if an auto company’s production is split evenly between electric vehicles and ICE vehicles that conform to the present average, the 59 g/km target will be just within reach. If a company cannot produce electric vehicles and remains at the current average emissions level, it will have to pay a fine of about €6,000 (£5,150) per car, or otherwise merge with a competitor that can build electric vehicles. But the EU’s formula is nothing but a huge scam. Electric vehicles also emit substantial amounts of CO2, the only difference being that the exhaust is released at a remove – that is, at the power plant. As long as coal- or gas-fired power plants are needed to ensure energy supply during the “dark doldrums” when the wind is not blowing and the sun is not shining, EVs, like ICE vehicles, run partly on hydrocarbons. And even when they are charged with solar- or wind-generated energy, enormous amounts of fossil fuels are used to produce EV batteries in China and elsewhere, offsetting the supposed emissions reduction. As such, the EU’s intervention is not much better than a cutoff device for an emissions control system. Earlier this year, the physicist Christoph Buchal and I published a research paper showing that, in the context of Germany’s energy mix, an EV emits a bit more CO2 than a modern diesel car, even though its battery offers drivers barely more than half the range of a tank of diesel. And shortly thereafter, data published by VW confirmed that its e-Rabbit vehicle emits slightly more CO2 than its Rabbit Diesel within the German energy mix. (When based on the overall European energy mix, which includes a huge share of nuclear energy from France, the e-Rabbit fares slightly better than the Rabbit Diesel.) Adding further evidence, the Austrian thinktank Joanneum Research has just published a large-scale study commissioned by the Austrian automobile association, ÖAMTC, and its
- 14. German counterpart, ADAC, that also confirms those findings. According to this study, a mid-sized electric passenger car in Germany must drive 219,000 km before it starts outperforming the corresponding diesel car in terms of CO2 emissions. The problem, of course, is that passenger cars in Europe last for only 180,000km, on average. Worse, according to Joanneum, EV batteries don’t last long enough to achieve that distance in the first place. Unfortunately, drivers’ anxiety about the cars’ range prompts them to recharge their batteries too often, at every opportunity, and at a high speed, which is bad for durability. As for EU lawmakers, there are now only two explanations for what is going on: either they didn’t know what they were doing, or they deliberately took Europeans for a ride. Both scenarios suggest that the EU should reverse its interventionist industrial policy, and instead rely on market-based instruments such as a comprehensive emissions trading system. With Germany’s energy mix, the EU’s regulation on fleet fuel consumption will not do anything to protect the climate. It will, however, destroy jobs, sap growth, and increase the public’s distrust in the EU’s increasingly opaque bureaucracy. https://www.theguardian.com/environment/2019/nov/25/are- electric-vehicles-really-so-climate-friendly In introduction, the author points the automobile that is most important industry in Europe to make readers initially think that the context is about the relationship between the Europe and the cars, and then he gives an example that about cheating on emission standards to deeply clarify what he would discuss about in the following paragraph. Therefore, for the following paragraph, to persuade the readers, the author instantly show the numbers of emission in carbon dioxide in 2019, and the goal they want to achieve after 2030. Also, he gives the gasoline engine and diesel engine to compare which emit more CO2, and shows the trend of CO2 emission between 2006 to 2018. It
- 15. indicates that the average emissions for new registered vehicles were around 161g/km in 2006, and then because the cars become smaller and lighter, the emission falls to 118g/km. However, the emission climbs back to 120g/km by 2018. After the author discuss the gasoline engine, he tries to guide readers to the electric vehicles. And then he instantly points out the flaws which EU consider that EVs do not emit any CO2. He states that the formula is a scam because of EV’s battery. It uses a lot of fossil fuel to produce EV batteries, and it just offsets the emission reduction. Moreover, he gives another evidence to convince readers. He published a research paper with the physicist. The paper is about EV emits slightly more CO2 than diesel car, although the battery offers drivers more than half range of a tank of diesel. And the data is from VW. Furthermore, the author gives the study that shows only if the EV must drive over 219,000 km, it equals to the CO2 emission of the diesel cars, but the batteries cannot last for this distance. After that, he gives his solution that the EU need to modify its policy in its emissions trading system. Also, he believes that the EU would not do anything on this issue because it will influence many stratus. Consequently, after analyzing the whole passage, I found that author use a lot of ethos concept, like facts, research, and numbers, to get readers’ credibility. By using these evidences, he can easily convince his readers. Also, he uses the proper ideas to give his solution, and conclusion, and then he lets readers more believe the author’s passage. PAGE 106 JOURNAL OF VASCULAR NURSING SEPTEMBER 2016 www.jvascnurs.net Evaluation of feasibility and safety of changing body position after transfemoral angiography: A randomized clinical trial
- 16. Sina Valiee, PhD, Mohammad Fathi, PhD, Nooshin Hadizade, MD, Daem Roshani, PhD, and Parvin Mahmoodi, MS From t Kurdista Nursing Kurdista Departm Departm Sanand Univers Corresp Commit Street, S Funding Kurdista 31229/1 1062-03 Copyrig http://dx Background: Considering the growing number of patients who suffer from cardiovascular and coronary artery disease and the significant importance of angiography in the diagnosis of coronary artery disease, this study investigated the ef- fects of position change on the acute complications of coronary angiography. Methods: This study was a randomized clinical trial. Sixty
- 17. patients undergoing coronary angiography, which was per- formed by a single operator were selected by convenience sampling method and were assigned to intervention or control groups by randomized block design (30 cases in each group). Intervention group patients’ position was changed according to schedule, whereas patients in the control group remained in the supine position in complete bed rest. At the entrance hours, 3, 6, 8, and 24 hours after the angiography, patients in both groups were evaluated in terms of vascular complica- tions, urinary retention, low back pain, groin pain, and comfort. Data were analyzed by repeated measures, Friedman, Mann–Whitney, chi-square, independent t-test, and Kolmogorov–Smirnov tests with SPSS-22. Results: The two groups did not show any significant difference in terms of demographic, clinical, and preinterventional catheterization characteristics (P > 0.05). There was no significant difference with regard to vascular complications including hematoma (P = 0.149), bleeding (P > 0.01), bruise (P = 0.081), and thrombosis in the two groups of patients during 5 consecutive reviews. However, there was a significant statistical difference regarding low back pain (P < 0.001), groin pain (P < 0.001), urinary retention (P = 0.02), and comfort (P < 0.001). Conclusions: The results of this study showed that changing the
- 18. positions of patients after angiography based on the provided program created no change in the incidence of vascular complications (hematoma, bleeding, thrombosis, and bruise) but resulted in reduced severity of back pain, groin pain, urinary retention, and increased patients’ comfort. (J Vasc Nurs 2016;34:106-115) Cardiovascular disease is one of the leading causes of death for women and men of all ethnicities and races,1 and it is ex- pected to remain the most common cause of death in the world until 2020.2 Among heart disease, coronary artery diseases is the most common and life-threatening one.3 he Social Determinants of Health Research Center, n University of Medical Sciences, Sanandaj, Iran; Department, School of Nursing & Midwifery, n University of Medical Sciences, Sanandaj, Iran; ent of Epidemiology and Biostatistics, Medicine ent, Kurdistan University of Medical Sciences, aj, Iran; Student Research Committee, Kurdistan ity of Medical Sciences, Sanandaj, Iran. onding author: Parvin Mahmoodi, MS, Student Research tee, Kurdistan University of Medical Sciences, Pasdaran anandaj, Iran (E-mail: [email protected]). : This work was supported by the Research Council of n University of Medical Sciences (grant number 1035/ 4). 03/$36.00 ht � 2016 by the Society for Vascular Nursing, Inc.
- 19. .doi.org/10.1016/j.jvn.2016.05.001 There are different diagnostic methods for assessing coronary artery disease.4 Coronary angiography is the golden standard test to identify the presence and extent of atherosclerotic disease of coronary artery.5 Annually, nearly three million cardiac catheter- izations are done in the United States of America.6 Angiography involves injecting a radiopaque dye into the coronary arteries un- der fluoroscopy which determines the condition of the coronary arteries and the degree of atherosclerosis. 7 Although the risks and complications associated with angiog- raphy depends on the patient’s condition, operator’s skill, and judgment, any invasive procedure has some complications asso- ciated with the procedure.5 Coronary angiography can be ac- cessed via the potential arteries included brachial, radial and femoral arteries.7–11 About 95% of angiography is performed via femoral artery.12,13 Access to the heart via femoral artery can be accompanied with complications such as arrhythmia, vascular complications (bleeding, hematoma, and thrombosis), injury and myocardial ischemia, coronaryartery perforation, hemodynamic collapse, cer- ebrovertebral accident including transient ischemic attack, allergy to contrast media and acute renal failure.14–18 Demonstration of these complications can be divided in two main form of acute and chronic. The former includes hematoma, bleeding,
- 20. thrombosis, urinary retention, low back pain, and groin pain.5 Studies have shown that to avoid possible complications due to arterial injuries, the current method of treatment after Delta:1_given name Delta:1_surname Delta:1_given name Delta:1_surname Delta:1_given name mailto:[email protected] http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://crossmark.crossref.org/dialog/?doi=10.1016/j.jvn.2016.05 .001&domain=pdf http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net Vol. XXXIV No. 3 JOURNAL OF VASCULAR NURSING PAGE 107 www.jvascnurs.net angiography in many health care facilities in Iran is to have the patient rest in the supine position with the head angle of zero de- grees for 8–24 hours and keeping 4 kg (8.82 lbs) sandbag on the catheter insertion site for 6 hours,19–21 which has often been conducted based on tradition and experience.19 This insistence on bed rest for patients after coronary catheterization can lead to restlessness, discomfort, and frequent complaint of back and groin pain. 11 About 42% of patients who get out of bed after 4 hours of rest experience back pain.24 In addition, 11.4% of
- 21. pa- tients undergoing this procedure may develop urinary reten- tion.14,25 Back pain, groin pain, and urinary retention leads to the use of analgesic medications and urinary catheterization which are associated with their own specific complications. To avoid complications resulting from the use of analgesic medications and urinary catheterization, nonmedical measures and nursing care are appropriate.10 Development of technology along with procedures requires appropriate medical and nursing care. 22,23 Although there is much evidence for medical approach to care, little evidence exists to support the suggestions relating to management areas such as patient’s position, the time of getting out of bed, and the time of removing sandbag which are generally related to the nursing activities territory.9,24-26 A recent literature review showed that caring of patients undergoing cardiac catheterization requires a revision in key areas of nursing care.19,22,25 Abdollahi et al14 (2013) reported that in addition to changes in body position and leaving the bed early, no vascular complications in patients undergoing coronary angiography was seen, whereas urinary retention in the control group was observed. Rezaei-Adaryani et al 19 (2009) reported that patients whose positions were switched during the period of bed rest had experiences less fatigue but more comfort and satisfaction in the 3, 6, 8, and 24 hours after arrival to the postangiography
- 22. ward. In addition, changes in body position had no significant impact on increased bleeding and hematoma compared with the control group.19 Heravi et al27 (2013) comparing the patients in supine positions with the head angle of 0, 15, 30, 45, and 60 in separate groups reported that patients with head angle of 45� had experienced the lowest pain, so it was declared as the best position. One of the nursing measures is changing the position of the patient who has undergone transfemoral angiography during bed rest, but it is avoided due to the fear of the vascular complications. The effects of position change in patients after transfemoral angiography during bed rest will be evaluated as it relates to vascular complications. This study aimed to determine the ef- fect of changing position on urinary retention, back pain, pain in the groin, and comfort of patients undergoing coronary angiography. METHOD The study is a single-blind randomized clinical trial in two groups which was approved by the Kurdistan University of Medical Sciences research Council. The study’s proposal is registered at (www.irct.com) by the registration number IRCT2015091424018N1. Sample size and sampling The samples were chosen by convenience sampling method, and they were randomly allocated into control and intervention groups. The sample size with 95% confidence interval and 80% statistical power was estimated 60 patients (30 patients in the intervention group and 30 patients in the control group)
- 23. (Figure 1). Participants Participants were patients undergoing coronary angiography. Inclusion criteria included nonemergency catheterization, age 18–65 years old, less than 180/100 mm Hg blood pressure, absence of active bleeding disorders, prothrombin time (PT), and partial thromboplastin time (PTT) of less than 16 and 90 sec- onds, respectively, consent to participate in the study, angiog- raphy via the femoral artery, no history of deep vein thrombosis (DVT) before the procedure, not being treated with thrombolytic (not taking streptokinase) and anticoagulant drugs (not taking warfarin), no history of diabetes with sensory prob- lems, not taking any analgesic medications before the procedure, not suffering from peripheral arterial disease, no history of uri- nary problems, no history of allergy to contrast media, no depen- dency to drugs, lack of chronic low back pain, absence of blood and liver diseases. Exclusion criteria included needle entrance more than once to access the artery, cardiopulmonary resuscita- tion during angiography, movement disability, and disorder in the level of consciousness in a way that the patient can not coop- erate to change position and incomplete termination of clinical intervention period. Ethical considerations This study was approved by the Research Council of Kurdi- stan University of Medical Sciences with the contract number 1035/31229/14 and was confirmed for ethical considerations by receiving the moral code muk.rec.1394.194 from the ethics com-
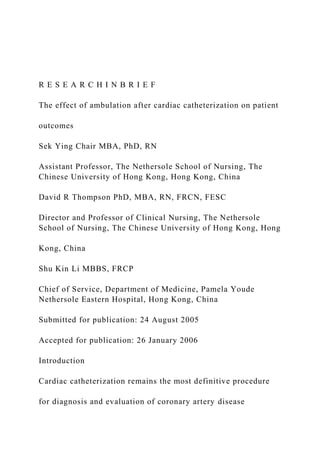
- 24. mittee of Kurdistan University. While explaining the purpose and method of study for the patients, informed consent was obtained from them. Measuring tool The instrument used to collect and record information in this was a three-part questionnaire which was designed according to the study. The first part was demographic and clinical information form which contained information about age, height, weight, gender, marital status, education, occupation, history of smoking, dia- betes, history of previous coronary angiography, systolic and dia- stolic blood pressure, body mass index, PT, PTT, international normalized ratio, and platelet count which was recorded based on the information contained in patients’ medical records. Patients’ blood pressure was measured and recorded by one person using a mercury sphygmomanometer (ALP K2 model: no 300-VS; Tanaka Sangyo Co, Ltd, Tokyo, Japan) which was calibrated before the start of the study. Their height and weight were measured and recorded by one person using digital scales (Bermend BD7750) and centimeters. The second section con- tained procedural information form which contained the length http://www.irct.com http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net Assessed for eligibility (n = 81)
- 25. Excluded (n= 15): • Chronic Low Back Pain(n = 6) • unwillingness to participate in the study(n = 4) • history of taking anticoagulant(n = 2) • Dependence on opium (n = 3) Randomized (n = 66) Allocated to intervention group(n = 33): • Received routine care (n = 33) • Did not received routine care (n = 0) A llo ca ti on E nr ol lm en t Allocated to control group (n = 33) • Received changing of body
- 26. position(n = 33) • Did not receive allocated intervention(n = 0) F ol lo w u p Lost to follow up (n =3): • Had anaphylactic reactions to the contrast agent(n =2) • Failure to did angiography because of obstruction in abdominal aortic (n =1) Lost to follow up (n =3): • Had chest pain and take analgesic medications (n=2) • 3 times needle inserted to access artery (n =1) A na ly
- 27. si s Analyzed (n =30) Analyzed (n =30) Figure 1. Consolidated Standards of Reporting Trials (CONSORT) flow diagram. PAGE 108 JOURNAL OF VASCULAR NURSING SEPTEMBER 2016 www.jvascnurs.net of angiography, homeostasis time, size of the catheter used, injury of the femoral artery, and the type and volume of contrast agent, diagnosis of coronary artery stenosis which were prepared using a chronometer and the information contained in patient records. Part three of the evaluation form included angiographic com- plications such as hematoma, bleeding, urinary retention, back pain, groin pain, and comfort. Back pain, groin pain, and comfort were measured and recorded with standard numeric rating scale.28 Patients’ comfort level was measured by a general ques- tion about the overall level of comfort at the time of measure- ment. The patients were asked to rate their comfort from 0 to 10 grades. The validity of this scale was set by Johnson and Carol.22 The reliability was estimated by Farrar et al and Good et al to be 0.78 and 0.83.29,30 Hematoma shape and bruise was placed on transparent paper and then on graph paper, and the side of intended shape was measured and recorded (based on the biggest length and width) per square centimeter. The amount of bleeding was measured by weighing Gauze soaked in blood by 0.1 gm sensitive Japanese scale (standard future).
- 28. Urinary retention was also analyzed based on patient interview. All the measurements were carried out by the principal researcher. Intervention procedures After the selection of eligible patients for inclusion into the study and providing the necessary explanations, obtaining informed consent, necessary data were obtained from medical re- cords, and blood pressure was measured and recorded. The pa- tients were randomly entered into to the intervention group. After controlling patients’ vital signs and marking dorsal pedis and posterior tibialis pulses on their feet, the patients were entered in the angiography catheterization room. On completion of angiography and exiting the catheterization laboratory, the sheath was removed by cardiology nurses, mechanical or manual homeostasis was applied on the insertion site until the blood coagulated. The time hemostasis was measured by stopwatch, and it procedural information was recorded based on the case. After hemostasis, 2 folded 4 � 4 (4 cm length and width) gauzes was put on the catheter site (the reason of making the gauzes 2 folded was to expose the catheter insertion site to the maximum extent possible for ease of evaluating complications). Transparent bandage covered the dressing to check for the ease in monitoring for hematoma and bleeding. Then, two 4 kg (8.82 lbs) sandbags were placed on the site, and the second sandbag was removed after stabilization of the patient. The patient came to the postangiography ward with only one sandbag. After entering http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net
- 29. TABLE 1 PROTOCOLS OF BODY POSITION AND METHODS OF ANALYSIS IN THE GROUPS Group 1st & 2nd hour 3rd & 4th hour 5th hour 6th hour 7th & 8th hour 9th hour 24th hour Intervention Group Supine Supine, HOB Right side, HOB Left side, HOB Sitting position OOB OOB 45� El 15� El 15� El Control group Supine Supine Supine Supine Supine OOB OOB HOB = head of bed; EL = elevation. Vol. XXXIV No. 3 JOURNAL OF VASCULAR NURSING PAGE 109 www.jvascnurs.net the control group patients to the postangiography ward routine, cares were performed. The patient was immobile in the supine position, with head angle of zero degree, 8 hours complete bed rest, and 4 kg (8.2 lbs) sandbags was put on the site where the catheter was inserted for 6 hours. After entering the intervention group patients to the post angiography ward, the patient had 8 hours complete bed rest, 4 kg sandbag was put on the site where the catheter was inserted for 6 hours, but changing position was applied while taking rest in the bed for 8 hours (Table 1). During the first and second hours, the patient was kept in the supine position and the head angle of
- 30. zero degree. During the third and fourth hours, the patient was kept in the supine position with the head angle of 45�. During the fifth and sixth hours, the patient was lying on the left or right side with the head angle of 15� and in the seventh and eighth hour the patients were cared in the sitting position (Table 2). The third part of the questionnaire was measured and recorded immedi- ately after entering the ward, third, sixth, eighth, and 24th hours later (before discharge from the ward; Table 2). Statistics After collecting data to assess the normal distribution of data, Kolmogorov–Smirnov test was used. To compare the two inter- vention and control groups in terms of demographic, clinical, and procedural quality, chi-square and Fisher’s exact tests were used. Moreover, to compare quantitative variables independent t-test and Mann–Whitney tests were used. RESULTS Eighty-one patients were assessed for inclusion criteria. Some patients were excluded from the study for the following reasons including; three patients because of a history of chronic low back pain, four patients because of an unwillingness to participate in the study, two patients because of the history of anticoagulant, and three patients due to taking opium. Thirty- three patients were assigned to each group. During the study, in the intervention group, two patients were excluded from the study due to chest pain and taking analgesic and one patient due to needle entrance to the arteries more than once. In the con- trol group, two patients were excluded due to anaphylactic reac- tions and one patient due to stenosis in the abdominal aorta.
- 31. Finally, two groups (n = 30, each group) were analyzed. There was no significant difference between the two groups of participants in terms of demographic and clinical data include of mean age, height, weight, systolic blood pressure, diastolic blood pressure, body mass index, PT, PTT, platelet count, inter- national normalized ratio, homeostasis time length, contrast me- dia volume, amount of smoking, marital status, education level, smoking history, history of diabetes, history of previous coronary angiography, rupture of the femoral artery, final diagnosis, recommend treatment, and the amount of stenosis in the right coronary, left main coronary, left circumflex arteries, and the two groups were homogenous (Tables 3 and 4). But in terms of gender, occupation, catheter size, type of contrast, the stenosis of left anterior descending artery, and duration of angiography were significantly different (Tables 3 and 4). The mean age of the patients was 10.445 � 57.71, and 34 patients (56.66%) were male and 58 (96.65%) were married. The results showed that the incidence of hematoma between the two groups was not significant. Moreover, hematoma in the intervention group (P = 0.006) was significantly different at different times, but in the control group (P = 0.149), the differ- ence was not significant (Table 4). Considering the P values in Table 5, to compare between intervention and control groups at different times, there were no significant differences between the intervention and control groups in terms of hematoma (Table 5). The results showed that the incidence of urinary retention in the control group (P = 0.023) and intervention group (P = 0.020) were significantly different at different times (Table 4). With re- gard to the P values in Table 5, pairwise comparison between intervention and control group at different times, there were no
- 32. significant differences between the intervention and control groups in terms of complications of urinary retention (Table 4). Furthermore, the incidence of thrombosis remained un- changed at different times and was not observed in none of the participants. In addition, the incidence of bleeding was significantly different in terms of time (P $ 0.001). The test results of Bonfer- roni procedure showed that in the control group at third, eighth, and 24th hours were not significantly different in terms of the mean of this variable and in the intervention group there was a significant difference only between the time of entrance and the other times. The results showed that the incidence of bruise between the two groups in different measurements did not differ significantly in terms of time (P = 0.081). http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net TABLE 2 DISTRIBUTION OF UNITS IN TERMS OF VARIABLES Variable Group Mean � SD P value Age* Control 56.56 � 9.15 0.401 Intervention 58.86 � 11.74 Heighty Control 164.16 � 11.31 0.151
- 33. Intervention 166.16 � 12.58 Weight* Control 74.88 � 21.67 0.52 Intervention 77.43 � 22.64 The number of cigarettes smoked per dayy Control 8.1 � 4.1 0.076 Intervention 9.15 � 56.56 No. of previous angiographyy Control 0.66 � 0.33 0.076 Intervention 16.36 � 0.1 Systolic blood pressurey Control 122.26 � 19.11 0.653 Intervention 123.33 � 14.93 Diastolic blood pressure y Control 74.03 � 11.58 0.583 Intervention 75.33 � 8.6 Volume of contrast dyey Control 51.33 � 23 0.564 Intervention 51.33 � 22.55 BMI y Control 55.99 � 36.64 0.6 Intervention 26.34 � 3.62 PTy Control 11.73 � 0.86 0.364 Intervention 11.56 � 0.93 PTT
- 34. y Control 31.7 � 3.00 0.298 Intervention 33.1 � 6.7 Plt count* Control 245230 � 9.15 0.298 Intervention 250610 � 80.01 INRy Control 17 � 1.15 0.292 Intervention 1.14 � 0.28 Duration of hemostasis periody Control 7.95 � 3.69 0.603 Intervention 6.41 � 1.67 Duration of angiography periody Control 23.78 � 10.51 0.031 Intervention 245230 � 9.15 BMI = body mass index; INR = international normalize rate; PT = protrombin time; Plt count = platelet count; PTT = partial thromboplastin time. *T independent. yMann–Whitney. PAGE 110 JOURNAL OF VASCULAR NURSING SEPTEMBER 2016 www.jvascnurs.net The results showed that the incidence of groin pain was significantly different in terms of time (P > 0.001). The results of Bonferroni for comparing sampling time between the inter- vention and control groups showed that during the study period except at zero and 24th hour the difference was significant in terms of intended complication. The results showed that the incidence of comfort (based on numeric rating scale) had a significant difference in terms of
- 35. time in this complication (P = 0.001). Bonferroni procedure for pairwise comparisons of the sampling time between the intervention and control groups during the study period showed a significant difference except for the time of admission and 24th hour. Moreover, there was a significant difference for the incidence of back pain in terms of time. Bonferroni for pairwise comparisons of the sampling time between the intervention and control groups during the study period showed a significant dif- ference in terms of comfort except for the time of entrance and 24th hour. http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net TABLE 3 DISTRIBUTION OF SUBJECTS BASED ON QUALITATIVE VARIABLES BETWEEN THE TWO GROUPS OF CONTROL AND INTERVENTION Variable Subgroup Intervention Control P value Gender** Male 22 12 0.009 Female 8 18 Marital status** Married 30 28 0.492 Single 0 1 Widow 0 1 Divorced 0 0
- 36. Education** Illiterate 22 18 0.445 Under diploma 7 9 Diploma 1 3 Academic 0 0 Job status** Clerk 2 1 0.002 Self-employed 19 6 Retired 3 4 Housewife 6 18 Unemployed 0 1 Smoking history* Has 17 8 0.018 Has not 13 22 Diabetes record* Has 7 9 0.559 Has not 23 21 Angiography history** Has 1 6 0.103 Has not 29 24 Catheter size** F400 1 0 0.006 F500 1 0 F600 20 29
- 37. F700 8 1 Rupture of the femoral artery** Has 0 0 1.00 Has not 30 30 Type of contrast media** Meglumine 14 20 0.019 Visipaque 16 7 Meglumine and Visipaque 0 3 Disease diagnosis* NECA 10 16 0.425 1VD 2 2 2VD 12 7 3VD 6 5 Significance stenosis of coronary arteries *RCA 9 7 0.559 **LMCA 1 0 1.00
- 38. *LAD 14 6 0.028 **LCX 4 8 0.333 (Continued) Vol. XXXIV No. 3 JOURNAL OF VASCULAR NURSING PAGE 111 www.jvascnurs.net http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net TABLE 3 CONTINUED Variable Subgroup Intervention Control P value Urinary retention*** Has 9 10 Has not 21 20 F00 = French; NECA = normal epicardial coronary arteries; 1VD = one vessel disease; 2VD = two vessel disease; 3VD = three vessel disease; RCA = right coronary artery; LMCA = left main coronary artery; LCX = left circumflex artery; LAD = left anterior descending. Chi-square test**, Fisher exact test*, and Friedman test*.
- 39. PAGE 112 JOURNAL OF VASCULAR NURSING SEPTEMBER 2016 www.jvascnurs.net DISCUSSION The findings of this study showed that changes in body posi- tion after angiography did not create a change in the incidence of vascular complications including hematoma, bleeding, throm- bosis, and bruising compared to the control group, whereas uri- nary retention was reduced. In addition, changing body position reduced back pain, groin pain, and finally improved the comfort of the patient. Other studies finding agree with the results of this study and a significant difference in the incidence of complications after cor- onary angiography at the catheter insertion site between the inter- vention and control groups was not reported. For example, TABLE 4 RESULTS OF ACUTE COMPLICATIONS Variable Group Hour 0 Hour 3rd Hematoma* Control 1.07 � 3.23 1.07 � 3.23 Intervention 0.43 � 2.19 0.43 � 2.19 Urinary retention* Control 2 1.93 � 0.25 Intervention 1.93 � 0.25 2.56 � 3.68 Bruise y
- 40. Control 1.08 � 3.37 1.1 � 3.37 Intervention 0.35 � 1.82 0.36 � 1.82 Bleeding y Control 0 0.01 � 0.07 Intervention 0 0.01 � 0.05 Back painy Control 2.74 � 2 3.1 � 4.46 Intervention 2.66 � 1.6 3.3 � 2.83 Groin painy Control 0.26 � 0.63 3.1 � 2.57 Intervention 0 1.03 � 2.04 Comforty Control 9.66 � 1.82 7.6 � 2.48 Intervention 10 9.06 � 1.7 Thrombosisy Control 0 0 Intervention 0 0 *Friedman test. yRepeated measures test. Abdollahi et al (2015) studied the simultaneous effects of early ambulation (4 hours of bed rest) and changes in body position with a different protocol from this study. The time points for analyzing the patient in terms of complications were different. In their study, no hemorrhage and hematoma was reported. It was found that changes in body position in and early ambulation after coronary interventions did not increase the vascular complications.14 Furthermore, the results indicated that changes in body posi- tion had no impact on the incidence of acute vascular complica- tions, including hematoma and bleeding. Moreover, Yeganeh Khah et al (2012) compared the effect of different ways of
- 41. chang- ing patients’ position on the vascular complications of after Hour 6th Hour 8th Hour 24th Sig 0.61 � 1.78 0.31 � 0.97 0.08 � 0.43 0.006 0.33 � 1.64 0.1 � 0.40 0 0.149 1.83 � 0.37 1.76 � 0.43 1.8 � 0.4 0.023 1.8 � 0.4 1.7 � 0.46 1.9 � 0.25 0.02 1.03 � 3.18 0.8 � 2.54 0.12 � 0.45 0.081 0.16 � 0.73 0.026 � 0.14 0.026 � 0.14 2.3 � 12.77 0.16 � 0.54 4.38 � 7.56 0.001> 0.01 � 0.03 0.11 � 0.19 5.34 � 4.59 3.14 � 5.8 3.26 � 4.03 1.85 � 0.43 0.001> 3.14 � 2.3 2.75 � 1.56 0 4.86 � 3.08 3.7 � 2.74 2.36 � 2.20 0.001> 1.96 � 2.37 1.86 � 2.16 1.66 � 2.45 6.03 � 2.2 6.6 � 2.4 8.63 � 1.67 0.001> 8.5 � 2.2 7.9 � 2.39 8.9 � 2.15 0 0 0 0 0 0 0 0 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net TABLE 5 MANN–WHITNEY TEST TO COMPARE THE GROUPS TWO BY TWO IN TERMS OF STUDY TIME
- 42. Variable Measurement time P value Hematoma Entrance time 0.317 Third hour 0.579 Sixth hour 0.394 Eighth hour 0.222 24th hour 0.222 Urinary retention Entrance time 0.312 Third hour 0.563 Sixth hour 0.741 Eighth hour 0.977 24th hour 0.154 Vol. XXXIV No. 3 JOURNAL OF VASCULAR NURSING PAGE 113 www.jvascnurs.net coronary angiography and reported that none of the patients developed bleeding and arterial occlusive and no significant dif- ference between intervention and control groups were observed in changing body position. Rezaei-Adaryani et al (2009) compared the effect of three different body positions including the supine position, changing the head angle and changing side by side in three separate groups and found that changing body positions did not have an impact on the amount of bleeding and hematoma of the two groups at
- 43. different times after angiography.19 This study was different from Adaryani study because it was a comparative study con- ducted on two groups, and different body positions were used, but the findings were consistent with the Adaryani study. Acute vascular complications after coronary angiography are hema- toma, bleeding, and thrombosis.14–18 Farmanbar et al (2012) studied changes in body position and duration of bed rest in two separate groups. Fisher’s exact test showed no significant difference between the two groups. In this study, patients had sandbags just for 2 hours and after 4 hours changing position they got out of bed. Three patients in the con- trol group and one patient in the experimental group had hema- toma. One case of bleeding in the control group and one in the intervention group were reported as well. 31 However, in this study, the effect of changing position was studied not only on the complications but also on back pain, groin pain, urinary retention, and comfort, and the rate of incidence of complications was lower. Nyshabouri and Ashke-e-torab (2007) studied the ef- fect of changing the bed angles on the incidence of vascular com- plications and reported no case of hematoma, bleeding, and thrombosis among the groups.32 In this study after two hours of rest in the supine position, the patient’s head angle was in 45� because in previous studies the lowest amount of complica- tions was in this position. Therefore, changing body positions in the bed based on the presented method had no effect on the incidence of vascular complications such as hematoma, bleeding, and thrombosis and did not make any complications in the pa-
- 44. tients. Based on several studies, movement limitations and com- plete bed rest resulted in frequent complaint of low back pain.14 As a result patients request for analgesic and changing position frequently to resolve the pain in the bed.19 Therefore, relieving pain and providing patient comfort without increasing vascular complications after coronary angiography is one of the nursing goals.13 Yilmaz et al (2007) in Turkey studied the effect of sandbags and changing the patient’s position on the incidence of vascular complications, and they claimed that there was no difference be- tween the groups of patients who had or had not sandbag on the site of catheter insertion. However, the pain severity in the group who had changing positions was by far less than the other group which is consistent with the findings of our research. Moreover, there was no significant difference between the two groups in the second hour which was not in accordance with our findings 21 because in Yilmaz et al study the sandbag was on the site of cath- eter insertion for two hours and a half, whereas in our study it was 6 hours. To compare changes in bleeding, bruise, back pain, groin pain, comfort, and thrombosis over time within groups repeated measures test was used and if the difference was significant Bon- ferroni test was used. To compare changes regarding hematoma
- 45. and urinary retention over time within groups Friedman test was used, and for pairwise comparison of intervention and control groups Mann–Whitney test was used based on distinct time of study. Back pain and urinary retention were observed as common complication in looking after patients undergoing angiography. Relying on noninvasive methods to empty the bladder is prefer- able because bladder catheterization increases the risk of urinary tract infection.22 Abdolahi et al (2015) in a study regarding changing positions compared the control and experimental groups with a different protocol from this study and found that no significant differences exist between the two groups in terms of complications of urinary retention14 which is consistent with our study. Pairwise comparisons of sampling time showed that there was significant difference in terms of the intended compli- cation between intervention and control groups during the study period except at zero and 24th hour which was probably due to the reason that at the zero hour patients in both groups were in supine position with head angle of zero degree and at 24th hour both groups were out of bed and as a result due to the equality of body position, it is expected that the difference did not become significant. Changing body position in the bed improves the patient’s comfort.13 Many teams emphasizes on immobilitzation to avoid bleeding, which can cause patient comfort Rezaei-Adaryani et al 19 (2015) in a study regarding changing positions compared the control and experimental groups with a different protocol from this study and found that the intervention group had signif-
- 46. icantly more comfort at third, sixth, eighth hours, and the morn- ing after angiography compared with the control group which was consistent with our study.19 Change in body position based on the proposed manner resulted in decrease in lower back pain, groin pain, urinary retention, and increase in comfort. http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net PAGE 114 JOURNAL OF VASCULAR NURSING SEPTEMBER 2016 www.jvascnurs.net Limitations and suggestions for future research It is recommended that in future studies analyze the impact of early ambulation, the duration of keeping sandbag on the catheter insertion and sandbags with different weights on the incidence of acute and chronic complications at different time points from this study, to improve care after coronary angiography. CONCLUSIONS The results of this study showed that changing position after angiography based on the method provided, without change in the incidence of vascular complications (hematoma, bleeding, thrombosis, and bruise) reduced the severity of back pain, groin pain, urinary retention, and improved patients’ comfort. By changing position in bed after coronary angiography, nurses can increase patients’ comfort. New nurses tend to be cautious and the more seasoned nurses adhere to routine. Therefore, it is recom- mended that cardiology and postangiography ward nurses, use
- 47. the position change based on the present study. Interventionalist and nurse comfort play a role in patient comfort and reposition. Inter- ventionalists will need to address any postprocedural complica- tion for patients which may affect the level of their comfort. We can reduce the complications including urinary retention, discom- fortback and groin pains by positionchange. So by decreasing the- ses complications, the interventionalists comfort will increase due to lower discuses about postprocedural complications and their high level of comfort affect patients comfort. ACKNOWLEDGMENTS Hereby, the authors want to appreciate the Deputy of Research at Nursing and Midwifery faculty of Kurdistan Uni- versity of Medical Sciences, angiography and cardiac ward’s staff at Tohid Hospitals affiliated with Kurdistan University of Medical Sciences and all those patients who have helped us in this study. This study entitled the Comparative Study of the Effects of Sand Bag Keeping Time and Changing Body Posi- tion on Acute Complications of Coronary Angiography in Referring Patients to the Sanandaj Tohid Hospital, 2015 is a part of MS thesis of Parvin Mahmoodi which is approved in Kurdistan University of Medical Sciences. REFERENCES 1. Brunner LS, Suddarth DS. The Text Book Medical Surgical Nursing. 10th ed. Philadelphia: Williams &Wilkins; 2014: 122-3. 2. Rashidi M, Ghias M, Ramesht MH. Geographical Epidemi- ology of Death Due to Cardiovascular Diseases in Isfahan
- 48. Povince, Iran. J Isfahan Med Sch 2011;29(125):13-9. 3. Parkosewich JA. Assessment of Cardiovascular Function. In: Smeltzer SC, Bare BC, Hinkle JL, et al., editors. Brunner and Suddarth’s: Text book of medical surgical nursing. 12th ed. Philadelphia: Lippincott Williams &Wilkins; 2010:713-5. 4. Tahmasbi H, Mahmoodi G, Mokhberi V, et al. The impact of aromatherapy on the anxiety of patients experiencing coro- nary angiography. J Urmia Nurs Midwifery Fac 2012; 14(3):51-5. 5. Tavakol M, Ashraf S, Brener SJ. Risks and complications of coronary angiography: a comprehensive review. Glob J Health Sci 2012;4(1):65. 6. Sedlacek MA, Newsome J. Identification of vascular bleeding complications after cardiac catheterization through development and implementation of a cardiac catheterization risk predictor tool. Dimens Crit Care Nurs 2010;29(3): 145-52. 7. Burn KL, Marshall B, Scrymgeour G. Early mobilization af- ter femoral approach diagnostic coronary angiography to reduce back pain. J Radiol Nurs 2015;34(3):162-9. 8. Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral ac- cess for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, par- allel group, multicentre trial. Lancet 2011;377(9775): 1409-20. 9. Bertrand OF, B�elisle P, Joyal D, et al. Comparison of trans- radial and femoral approaches for percutaneous coronary in- terventions: a systematic review and hierarchical Bayesian meta-analysis. Am Heart J 2012;163(4):632-48.
- 49. 10. Rigattieri S, Sciahbasi A, Brilakis E, et al. TCT-429 Radial versus Femoral Approach for Coronary Angiography and Intervention in Patients with CABG: Systematic Review and Meta-analysis. J Am Coll Cardiol 2015;66(15_S): B175. 11. Cortese B, Russo F, Trani C, et al. TCT-430 Ancillary radial versus femoral/brachial approach to reduce vascular compli- cations in complex coronary, peripheral and structural inter- ventions. Preliminary results of a study from the Italian Radial Club. J Am Coll Cardiol 2015;66(15_S):B175-176. 12. Jolly SS, Niemel€a K, Xavier D, et al. Design and rationale of the RadIal Vs. femorAL access for coronary intervention (RIVAL) trial: A randomized comparison of radial versus femoral access for coronary angiography or intervention in patients with acute coronary syndromes. Am Heart J 2011; 161(2):254-260. e1–e4. 13. Chair SY, Thompson DR, Li SK. The effect of ambulation after cardiac catheterization on patient outcomes. J Clin Nurs 2007;16(1):212-214. 14. Abdollahi AA, Mehranfard S, Behnampour N, et al. Effect of Positioning and Early Ambulation on Coronary Angiography Complications: a Randomized Clinical Trial. J Caring Sci 2015;4(2):125. 15. Nikolsky E, Mehran R, Halkin A, et al. Vascular complica- tions associated with arteriotomy closure devices in patients undergoing percutaneous coronary procedures: a meta-anal- ysis. J Am Coll Cardiol 2004;44(6):1200-1209. 16. Nagai S, Abe S, Sato T, et al. Ultrasonic assessment of
- 50. vascular complications in coronary angiography and angio- plasty after transradial approach. Am J Cardiol 1999;83(2): 180-186. 17. Castillo-Sang M, Tsang AW, Almaroof B, et al. Femoral ar- tery complications after cardiac catheterization: a study of patient profile. Ann Vasc Surg 2010;24(3):328-335. 18. Christakopoulos GE, Christopoulos G, Carlino M, et al. Meta-analysis of clinical outcomes of patients who under- went percutaneous coronary interventions for chronic total occlusions. Am J Cardiol 2015;115(10):1367-1375. http://refhub.elsevier.com/S1062-0303(16)30067-X/sref1 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref1 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref1 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref2 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref2 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref2 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref3 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref3 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref3 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref3 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref4 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref4 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref4 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref4 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref5 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref5 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref5 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref6 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref6 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref6 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref6 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref6 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref7
- 52. http://refhub.elsevier.com/S1062-0303(16)30067-X/sref14 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref15 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref15 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref15 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref15 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref16 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref16 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref16 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref16 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref17 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref17 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref17 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref18 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref18 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref18 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref18 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.net Vol. XXXIV No. 3 JOURNAL OF VASCULAR NURSING PAGE 115 www.jvascnurs.net 19. Rezaei-Adaryani M, Ahmadi F, Asghari-Jafarabadi M. The effect of changing position and early ambulation after car- diac catheterization on patients’ outcomes: a single-blind randomized controlled trial. Int J Nurs Stud 2009;46(8): 1047-53. 20. Moraveji M, Naserian J, Bazarghan M. The effect of early ambulation of patients on bleeding and hematom via the femoral artery in post angiography ward in Ayatollah Moo- savy Hospital (Zanjan 2011). JSSU 2012;20(2):167-75. 21. Yilmaz E, Gurgun C, Dramali A. Minimizing short-term
- 53. complications in patients who have undergone cardiac inva- sive procedure: a randomized controlled trial involving posi- tion change and sandbag/Kardiyak invazif girisim yapilan hastalarda kisa donem komplikasyonlari azaltma: kum tor- basi ve pozisyon degisikligini iceren randomize kontrollu bir calisma. Anadolu Kardiyol Derg 2007;7(4):390-7. 22. Augustin AC, de Quadros AS, Sarmento-Leite RE. Early sheath removal and ambulation in patients submitted to percutaneous coronary intervention: a randomised clinical trial. Int J Nurs Stud 2010;47(8):939-45. 23. Mahmodi Y, Valiee S. A clinical trial of the effect of sexual health education on the quality of life of married Muslim women in Iran. Women Birth 2016;29:e18-22. 24. Mahmmodi Y, Masroor-Roodsari D, Varee S, et al. The role of family-based education in the management of depression in gastric cancer patients undergoing chemotherapy: a controlled clinical trial. Gastrointestinal Nurs 2016;14(1): 43-9. 25. Rolley JX, Salamonson Y, Dennison CR, et al. Development of clinical practice guidelines for the nursing care of people undergoing percutaneous coronary interventions: An Austra- lian & New Zealand collaboration. Aust Crit Care 2010; 23(4):177-87. 26. Woods SL, Froelicher ESS, Motzer SA, et al. Cardiac nursing. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. 27. Heravi MAY, Yaghubi M, Joharinia S. Effect of change in pa- tient’s bed angles on pain after coronary angiography accord- ing to vital signals. J Res Med Sci 2015;20(10):937.
- 54. 28. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986; 27(1):117-26. 29. Farrar JT, Troxel AB, Stott C, et al. Validity, reliability, and clinical importance of change in a 0—10 numeric rating scale measure of spasticity: a post hoc analysis of a random- ized, double-blind, placebo-controlled trial. Clin Ther 2008; 30(5):974-85. 30. Good M, Stiller C, Zauszniewski JA, et al. Sensation and distress of pain scales: reliability, validity, and sensitivity. J Nurs Meas 2001;9(3):219-38. 31. Farmanbar R, Afshar Mohammadian M, Nia M, et al. The ef- fect of position change and bed-rest duration after coronary angiography on vascular complications. Can J Crit Care Nurs 2012;4(4):177-82. 32. Neyshabouri M, Ashk T. Effects of change positioning on vascular complications and comfort in patients undergoing heart catheterization. KOOMESH 2007;9(1):53-8. http://refhub.elsevier.com/S1062-0303(16)30067-X/sref19 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref19 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref19 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref19 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref19 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref20 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref20 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref20 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref20 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref21 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref21
- 56. http://refhub.elsevier.com/S1062-0303(16)30067-X/sref31 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref31 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref32 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref32 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref32 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref32 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref33 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref33 http://refhub.elsevier.com/S1062-0303(16)30067-X/sref33 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://dx.doi.org/10.1016/j.jvn.2016.05.001 http://www.jvascnurs.netEvaluation of feasibility and safety of changing body position after transfemoral angiography: A randomized clinical trialMethodSample size and samplingParticipantsEthical considerationsMeasuring toolIntervention proceduresStatisticsResultsDiscussionLimitations and suggestions for future researchConclusionsAcknowledgmentsReferences