
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Catheter associated uti
Similar to Catheter associated uti (20)
More from Dr.Amjed Alnatsheh
More from Dr.Amjed Alnatsheh (16)
Recently uploaded
Recently uploaded (20)
Catheter associated uti
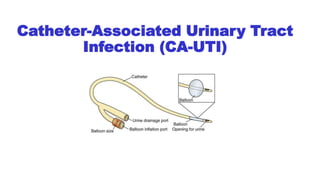
- 1. Catheter-Associated Urinary Tract Infection (CA-UTI)
- 2. Outlines 1. DEFINITIONS 2. EPIDEMIOLOGY 1. Incidence 2. Risk factors 3. PATHOGENESIS 4. MICROBIOLOGY 1. Spectrum of organisms 2. Antimicrobial resistance 5. CLINICAL FEATURES 1. Symptoms and signs 2. Laboratory findings 6. DIAGNOSIS 1. General approach 2. Specimen collection 7. TREATMENT 1. Antimicrobial therapy 2. Catheter management 8. COMPLICATIONS 9. ASYMPTOMATIC BACTERIURIA 10.PREVENTION
- 3. 1.DEFINITIONS A. Symptomatic Bacteriuria (UTI) 1. Culture growth of ≥103 colony forming units (cfu)/mL of uropathogenic bacteria in the presence of symptoms or signs compatible with UTI without other identifiable source in a patient with indwelling urethral, indwelling suprapubic, or intermittent catheterization. 2. Compatible symptoms include fever, suprapubic or costovertebral angle tenderness, and otherwise unexplained systemic symptoms such as altered mental status, hypotension, or evidence of a systemic inflammatory response syndrome.
- 4. B.Asymptomatic bacteriuria Culture growth of ≥105 cfu/mL of uropathogenic bacteria in the absence of symptoms compatible with UTI in a patient with indwelling urethral, indwelling suprapubic, or intermittent catheterization.
- 5. Patients who are no longer catheterized but had urethral, suprapubic, or condom catheters within the past 48 hours are also considered to have catheter-associated UTI or asymptomatic bacteriuria if they meet these definitions.
- 6. 2.EPIDEMIOLOGY A. Incidence Bacteriuria in patients with indwelling bladder catheters occurs at a rate of approximately 3 to 10 % per day of catheterization . Of those with bacteriuria, 10 to 25 % develop symptoms of UTI This translates into a substantial burden of CA-UTIs in hospitalized patients. In USA the incidence of CA-UTIs in 2012 was 1.4 to 1.7 per 1,000 catheter days in inpatient adult and pediatric medical/surgical floors
- 7. B. Risk factors I. The duration of catheterization is an important risk factor for catheter- associated bacteriuria and UTI II. Other risk factors include 1. Female sex 2. Older age 3. Diabetes mellitus 4. Bacterial colonization of the drainage bag 5. Errors in catheter care (eg, errors in sterile technique, not maintaining a closed drainage system, etc.)
- 8. 3.PATHOGENESIS • UTI associated with catheterization may be extraluminal or intraluminal. 1. Extraluminal infection occurs via entry of bacteria into the bladder along the biofilm that forms around the catheter in the urethra. 2. Intraluminal infection occurs due to urinary stasis because of drainage failure, or due to contamination of the urine collection bag with subsequent ascending infection. Extraluminal is more common than intraluminal infection
- 9. 4.MICROBIOLOGY A. Spectrum of organisms The causative pathogens in CA-UTI and asymptomatic bacteriuria are similar to those that are associated with complicated UTI in general. 1. E. coli —24 % of cases 2. Candida spp (or yeast) — 24 % 3. Enterococcus spp — 14 % 4. P. aeruginosa — 10 % 5. Klebsiella spp — 10 %
- 10. Some of these organisms associated with catheter-related bacteriuria or funguria may lack some of the virulence factors that allow the usual uropathogens to adhere to uroepithelium, but they take advantage of easy access to the bladder via the catheter. A good example of such an organism is Candida spp, which almost never cause UTI in the absence of an indwelling catheter. In contrast, candiduria is a common finding in patients with indwelling bladder catheters, particularly in those who are taking antimicrobials or are diabetic . Most patients are asymptomatic, funguria merely represents colonization, and progression to candidemia is uncommon .
- 11. A.Symptoms and signs Symptoms of catheter-associated UTI are protean and do not necessarily refer to the urinary tract. Fever is the most common symptom . Localizing symptoms may include flank or suprapubic discomfort, costovertebral angle tenderness, and catheter obstruction. 5. CLINICAL FEATURES
- 12. Patients with spinal cord injury may have especially atypical and nonspecific symptoms, including increased spasticity, malaise/lethargy, and autonomic dysreflexia. Individuals who develop UTI soon after removal of a catheter may be more likely to have the typical urinary symptoms of dysuria, frequency, and urgency.
- 13. • Pyuria is a common finding in catheterized patients with bacteriuria, whether they are symptomatic (ie, have UTI) or not. • Quantitative urine WBC >10 cells/microL had low sensitivity for predicting growth of >105 colony forming units (cfu)/mL (47 %) . • Specificity = 90 %. • The vast majority of these patients had no symptoms attributable to UTI. B.Laboratory findings
- 14. • The vast majority of patients with symptomatic bacteriuria (ie, UTI) have bacterial culture growth ≥105 cfu/mL or fungal growth in urine, although occasionally bacterial counts as low as 102 cfu/mL have also been described in individuals with UTI in the absence of a catheter . • The frequency of low count bacteriuria in the setting of catheter- associated UTI is not clearly defined but expected to be very low .
- 15. 6. DIAGNOSIS A.General approach The diagnosis of a CA-UTI is made by the finding of bacteriuria in a catheterized patient who has signs and symptoms that are consistent with UTI or systemic infection that are otherwise unexplained. A UTI diagnosed in a patient who had a catheter removed within the past 48 hours is also considered a CA-UTI.
- 16. Consistent findings may be specific to the urinary tract or may be more general, such as fever, leukocytosis, or signs of sepsis. If the diagnosis is based on such nonspecific findings, the evaluation should rule out the possibility of other systemic infections (eg, bacteremia, pneumonia, skin or soft tissue infection) prior to attributing them to a CA-UTI
- 17. B.Specimen collection Ideally urine samples for culture should be obtained by removing the indwelling catheter and obtaining a midstream specimen. if ongoing catheterization is warranted, a specimen through a new catheter. When this is not possible, the culture should be obtained through the catheter port, not the drainage bag
- 18. 7.TREATMENT A. Antimicrobial therapy • The approach to empiric antimicrobial therapy for patients with CA- UTI depends in part on the presentation and whether there are features that suggest an infection that has extended beyond the bladder (which use to distinguish acute complicated UTI from acute simple cystitis). • Most patients with CA-UTI come to clinical attention because of fever, flank pain, costovertebral angle tenderness, or systemic signs or symptoms of infection in the setting of pyuria and bacteriuria; such cases are consistent with acute complicated UTI and are managed as such.
- 19. • Some patients, in particular those who have recently had catheter removal, present with isolated symptoms of cystitis (eg, dysuria, urinary frequency or urgency) in the absence of fever or features of ascending infection or prostatitis. • Such patients can be managed as having acute simple cystitis
- 20. Categorization of UTIs Acute simple cystitis Acute UTI that is presumed to be confined to the bladder . There are no signs or symptoms that suggest an upper tract or systemic infection . Acute complicated UTI Acute UTI accompanied by signs or symptoms that suggest extension of infection beyond the bladder: 1. Fever (>37.7°C) 2. Chills, rigors, significant fatigue or malaise beyond baseline, or other features of systemic illness 3. Flank pain 4. Costovertebral angle tenderness 5. Pelvic or perineal pain in men, which can suggest accompanying prostatitis By this definition, Pyelonephritis is a complicated UTI, regardless of patient characteristics.
- 21. Suspect MDR gram-negative UTI in patients with a history of any of the following in the prior 3 months: An MDR gram-negative urinary isolate Inpatient stay at a health care facility (eg, Hospital, Nursing home, long-term acute care facility) Use of a fluoroquinolone, trimethoprim-sulfamethoxazole, or broad-spectrum beta-lactam (eg, third or later generation cephalosporin) Travel to parts of the world with high rates of multidrug-resistant organisms particularly high include India, Israel, Spain, and Mexico. Risk factors for multidrug-resistant (MDR) gram-negative UTI Acute simple cystitis in Women Treatment Acute simple cystitis in women Low risk for resistance First-line 1. Nitrofurantoin monohydrate/macrocrystals –100 mg orally twice daily for five days. 2. Trimethoprim-sulfamethoxazole–Double-strength tablet (160/800 mg) orally twice daily for three days. 3. Fosfomycin–3 grams of powder mixed in water as a single oral dose. 4. Pivmecillinam–400 mg orally two or three times daily for three to seven days Alternative 1. Amoxicillin-clavulanate (500 mg twice daily), 2. Cefpodoxime (100 mg twice daily), 3. Cefdinir (300 mg twice daily), and 4. Cefadroxil (500 mg twice daily), each given for five to seven days If beta-lactams cannot be used, a fluoroquinolone is reasonable; however, these should be reserved for more serious infections than acute simple cystitis, if possible, because of concerns of adverse effects. High risk for resistance First obtain urine culture and susceptibility testing 1. Nitrofurantoin monohydrate/macrocrystals (100 mg orally twice daily for five days) 2. Fosfomycin (3 grams of powder mixed in water as a single dose), or 3. Pivmecillinam (400 mg orally three times daily for three to five days)
- 22. Acute simple cystitis in Men Treatment Men is generally classified in the literature as a complicated UTI, it is reasonable to consider a healthy man without a neurogenic bladder who has mild to moderate dysuria, urinary frequency and/or urgency, with no symptoms or signs of infection outside the bladder, as having simple cystitis. For empiric antimicrobial treatment : 1. Nitrofurantoin monohydrate/macrocrystals (Macrobid, 100 mg orally twice daily) 2. Trimethoprim-sulfamethoxazole [160 mg TMP/800 mg SMX] orally twice daily) 3. Fosfomycin (3 grams of powder mixed in water as a single dose) Nitrofurantoin, fosfomycin, and beta-lactams do not achieve reliable tissue concentrations in the prostate and may not adequately treat subclinical prostatitis. For men who have more severe cystitis symptoms or concern about early involvement of the prostate, use a fluoroquinolone (Ciprofloxacin 500 mg orally twice daily or 1000 mg extended release once daily, or Levofloxacin 750 mg orally once daily) to achieve more reliable tissue concentrations. Fluoroquinolones can be given for five days, and other agents seven days.
- 23. Suspect MDR gram-negative UTI in patients with a history of any of the following in the prior 3 months: An MDR gram-negative urinary isolate Inpatient stay at a health care facility (eg, Hospital, Nursing home, long-term acute care facility) Use of a fluoroquinolone, trimethoprim-sulfamethoxazole, or broad-spectrum beta-lactam (eg, third or later generation cephalosporin) Travel to parts of the world with high rates of multidrug-resistant organisms particularly high include India, Israel, Spain, and Mexico. Risk factors for multidrug-resistant (MDR) gram-negative UTI Acute complicated UTI Treatment Patient population Risk for MDR? Empiric regimens Hospitalized with: 1- Critical illness warranting intensive care (eg, severe sepsis) or 2- Urinary tract obstruction N/A •Vancomycin 15 to 20 mg/kg IV every 8 to 12 hours with or without a loading dose plus •An antipseudomonal carbapenem: • Imipenem 500 mg IV every 6 hours or • Meropenem 1 g IV every 8 hours or • Doripenem 500 mg IV every 8 hours Other hospitalized patients No •Ceftriaxone 1 g IV once daily or •Piperacillin-tazobactam 3.375 g IV every 6 hours or •Alternatives: • Levofloxacin 750 mg IV or orally daily • Ciprofloxacin 400 mg IV twice daily • Ciprofloxacin 500 mg orally twice daily • Ciprofloxacin extended-release 1000 mg orally once daily Yes •Piperacillin-tazobactam 3.375 g IV every 6 hours or •An antipseudomonal carbapenem: • Imipenem 500 mg IV every 6 hours or • Meropenem 1 g IV every 8 hours or • Doripenem 500 mg IV every 8 hours
- 24. Patient population Risk for MDR?* Empiric regimens Outpatients No, and no concerns with fluoroquinolones (eg, at low risk for adverse effects) •For patients with low risk of fluoroquinolone resistance/toxicity: • Ciprofloxacin 500 mg orally twice daily for 5 to 7 days or • Ciprofloxacin extended-release 1000 mg orally once daily for 5 to 7 days or • Levofloxacin 750 mg orally once daily for 5 to 7 days No, but with concerns with fluoroquinolones (eg, at risk for adverse effects) •For patients who cannot use a fluoroquinolone: • One dose of a long-acting parenteral agent: • Ceftriaxone 1 g IV or IM once or • Ertapenem 1 g IV or IM once or • Gentamicin 5 mg/kg IV or IM once or • Tobramycin 5 mg/kg IV or IM once • Followed by one of the following: • TMP-SMX one double-strength tablet orally twice daily for 7 to 10 days or • Amoxicillin-clavulanate 875 mg orally twice daily for 10 to 14 days or • Cefpodoxime 200 mg orally twice daily for 10 to 14 days or • Cefdinir 300 mg orally twice daily for 10 to 14 days or • Cefadroxil 1 g orally twice daily for 10 to 14 days Yes •Ertapenem 1g IV or IM once •Followed by: • Ciprofloxacin 500 mg orally twice daily for 5 to 7 days or • Ciprofloxacin extended-release 1000 mg orally once daily for 5 to 7 days or • Levofloxacin 750 mg orally daily for 5 to 7 days Acute complicated UTI Treatment
- 25. The optimal duration of therapy is uncertain. Depending on the clinical response, the infecting organism, and the agent used for treatment, 7 to 14 days of therapy is generally appropriate
- 26. B-Catheter management • The optimal approach to catheter management in the setting of UTI is uncertain, although minimization of the use of indwelling catheters, when possible, is preferred. • In general, patients who no longer require catheterization should have the catheter removed and receive appropriate antimicrobial therapy . • Patients who require extended catheterization should be managed with intermittent catheterization, if possible.
- 27. • Intermittent catheterization is associated with a lower rate of bacteriuria and UTI than long term indwelling catheterization . • If long term catheterization is needed and intermittent catheterization is not feasible, the catheter should be replaced at the initiation of antimicrobial therapy . • Catheter replacement is associated with fewer and later relapses than retaining the original catheter, as biofilm penetration of most antimicrobials is poor
- 28. 8.COMPLICATIONS Important complications of CA-UTIs include Sepsis, Bacteremia, and involvement of the upper urinary tract. Approximately 20 % of health care-associated bacteremias arise from the urinary tract, and the mortality associated with this condition is about 10 %. In the ICU setting, a lower proportion of bacteremia is attributable to CA-UTIs .
- 29. 9.ASYMPTOMATIC BACTERIURIA Bacteriuria in the absence of symptoms is very common among catheterized patients . Treatment of asymptomatic bacteriuria does not affect patient outcomes, including the risk of complications and or the subsequent development of UTI symptoms, and increases the likelihood of emergence of resistant bacteria . Thus, with few exceptions, screening and treatment for asymptomatic bacteriuria in catheterized patients is not indicated.
- 30. Evaluating for asymptomatic bacteriuria in patients with indwelling catheters is warranted only in the setting of pregnancy or prior to urologic procedures for which mucosal bleeding is anticipated because of very specific risks of bacteriuria in these particular populations
- 31. 10.PREVENTION In general, the most important aspects of prevention of CA UTI are : 1. Avoidance of unnecessary catheterization 2. Use of sterile technique when placing the catheter 3. Removal of the catheter as soon as possible.
Editor's Notes
- Other risk factors include [13-15]: ●Female sex ●Older age ●Diabetes mellitus ●Bacterial colonization of the drainage bag ●Errors in catheter care (eg, errors in sterile technique, not maintaining a closed drainage system, etc.)
- unless the patient has a history of an isolate with documented resistance to these agents in the prior three months.
- Although cystitis in men is generally classified in the literature as a complicated urinary tract infection (UTI), it is reasonable to consider a healthy man without a neurogenic bladder who has mild to moderate dysuria, urinary frequency and/or urgency, with no symptoms or signs of infection outside the bladder, as having simple cystitis.