2. The role of ERCP in managing
pancreaticobiliary disorders is mostly
therapeutic one because other
of diagnostic testing (eg, MRI with
MRCP, endoscopic ultrasound)
high diagnostic accuracy without the
risks associated with ERCP (eg, acute
pancreatitis)
3. Indications for ERCP-guided interventions include :
1. Choledocholithiasis
2. Acute cholangitis
3. Drainage of malignant biliary obstruction (eg, pancreatic
cancer, hilar cholangiocarcinoma)
4. Post-surgical biliary complications (eg, biliary stricture, bile
leak)
5. Management of complications related to acute or chronic
pancreatitis (eg, pancreatic duct stricture, pancreatic stones)
6. Extrahepatic biliary strictures related to primary sclerosing
cholangitis
7. Endoscopic therapy for some patients with sphincter of Oddi
4. Contraindications
ERCP is usually contraindicated in conditions where the risk
of complications is high, and thus, the risks outweigh the
potential benefits of the procedure.
Some patients who are at high risk for complications, such
as those with acute severe cholangitis associated with sepsis
sepsis and cardiorespiratory dysfunction, may undergo
interventional ERCP to relieve biliary obstruction because of
the high risk of mortality related to severe cholangitis.
5. Relative contraindications to ERCP include:
Patients who cannot tolerate monitored anesthesia care or general anesthesia
Patients with an untreated hemostatic disorder who are deemed to be at high risk for
bleeding by the advanced endoscopist
Patients with gastrointestinal (luminal) obstruction may undergo endoscopy, but the
examination is limited to an area proximal to the level of obstruction
Patients with type III sphincter of Oddi dysfunction
Type III SOD: biliary-type pain but normal liver tests and common bile duct diameter
6. Risk factors
Some ERCP-related complications are due to the effect
of procedural sedation (eg, hypotension), while others
are due to the endoscopy itself or to an intervention.
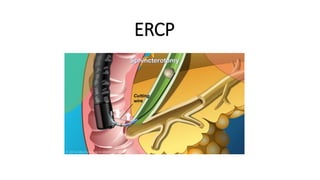
I. Procedure-related factors (eg, difficulty of
cannulation, biliary sphincterotomy, precut [access]
sphincterotomy)
II. Patient-related factors (eg, surgically-altered
anatomy, sphincter of Oddi dysfunction,
periampullary diverticulum, cirrhosis, older age,
and end-stage kidney disease)
7. Complications related to ERCP have also been characterized based on the following factors
Location – Complications may be focal, occurring at the point of endoscopic contact (eg, perforation,
bleeding, pancreatitis), or a complication may affect an organ system (eg, cardiopulmonary)
Timing – Complications may occur early (typically within 30 days after the procedure) or late (beyond
30 days).
Severity – The severity of complications can be assessed by duration and type of hospital stay (eg,
intensive care unit); blood transfusion requirement; need for surgical, radiologic, or endoscopic
interventions; and rates of morbidity and mortality
8. Complications
Pancreatitis — May result from mechanical injury to the pancreatic duct,
hydrostatic injury from contrast injection or guidewire manipulation.
Bleeding :Related to instrumentation such as biliary and/or pancreatic
sphincterotomy.
Infection — May be related to incomplete drainage of an infected biliary
system, obstruction of the cystic duct, infected pancreatic fluid collection, or
or rarely, contaminated endoscopic equipment
9. Perforation — ERCP may be complicated by
perforation of the esophagus, stomach, or
small intestine
Other complications — Several rare
complications have been associated with
ERCP including gas embolism, pneumothorax,
10. • Sphincterotomy-related complications
Rates overall have ranged from 3 to 12 % .
Sphincterotomy-related perforations are typically retroperitoneal.
Other interventions that are performed in addition to
sphincterotomy (eg, stone extraction, biliary stent placement) may
also contribute to the risk of complications
Anesthesia-related complications — Complications related to
procedural sedation and anesthesia (eg, hypoxemia, hypotension)
11. Post ERCP pancreatitis
• Post-ERCP pancreatitis (PEP) is the
most common serious adverse
event attributed to the ERCP,
resulting in annual estimated costs
exceeding 150 million dollars in the
United States.
12. Elevated serum pancreatic enzyme levels alone do not constitute
PEP, because transient increases in serum pancreatic enzyme levels
may occur in up to 75% of individuals after the procedure,
regardless of symptoms.
Conversely, individuals with low serum amylase levels less than 1.5
times the upper limit of normal, obtained 2 to 4 hours after ERCP,
are unlikely to have or develop PEP.
13. A recent meta-analysis of 108 randomized, controlled trials
involving 13,296 patients, reported a 9.7% overall incidence of PEP
(95% confidence interval [CI], 8.6%-10.7%), with an increased
incidence of 14.7% (95% CI, 11.8%-17.7%) in high-risk patients.
The majority of PEP cases were mild, with a mortality rate of
0.7%.
14. The definition of post-ERCP pancreatitis
●New or worsened abdominal pain combined with >3 times
the normal value of amylase or lipase more than 24 hours after
ERCP and requirement of hospital admission .
Mortality rates related to post-ERCP pancreatitis have also
been low and range from 0.1 to 0.7 percent
15.
16.
17. Pharmacologic prophylaxis
• Rectal nonsteroidal anti-inflammatory drugs —
We agree with society guidelines that endorse the use of NSAIDs; administered rectally to reduce the incidence
of post-ERCP pancreatitis in patients undergoing ERCP who do not have contraindications for NSAIDs.
We typically give indomethacin suppository 100 mg or diclofenac suppository 100 mg immediately before ERCP
ERCP .
Contraindications for rectal NSAIDs include pregnancy at ≥30 weeks gestation, history of skin disease such as
Steven-Johnson syndrome, or NSAID allergy .
Contraindications and adverse events associated with NSAIDs are discussed in more detail separately.
18. • NSAIDs inhibit several mediators of the inflammatory cascade that
are thought to play a role in the pathogenesis of acute pancreatitis
(ie, prostaglandins and phospholipase A2)
19. • Other pharmacologic strategies —However, some society
guidelines suggest that nitrates may be a reasonable alternative
alternative for prophylaxis in patients in whom NSAIDs and
aggressive intravenous hydration .
20. IV hydration
IV hydration is thought to prevent further injury to the pancreas from microvascular hypoperfusion.
Aggressive IV hydration with lactated Ringer’s (LR) solution ( preferred).
Patients in the aggressive hydration group received 3 mL/kg/hour during the procedure, a 20
mL/kg bolus immediately after the procedure, and 3 mL/kg/hour for 8 hours after the procedure.