Recommended

Recommended
More Related Content
More from SinzianaIonescu1
More from SinzianaIonescu1 (20)
Recently uploaded
Recently uploaded (20)
Surgical approach to intra-abdominal metastases from malignant melanoma
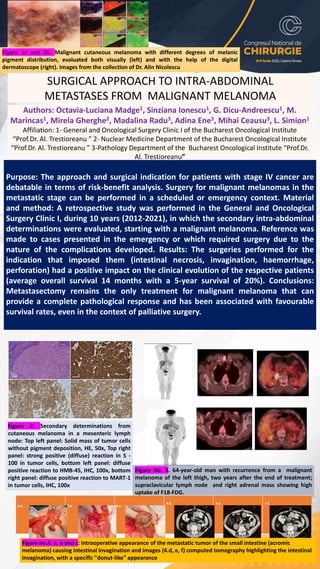
- 1. SURGICAL APPROACH TO INTRA-ABDOMINAL METASTASES FROM MALIGNANT MELANOMA Authors: Octavia-Luciana Madge1, Sinziana Ionescu1, G. Dicu-Andreescu1, M. Marincas1, Mirela Gherghe2, Madalina Radu3, Adina Ene3, Mihai Ceausu3, L. Simion1 Affiliation: 1- General and Oncological Surgery Clinic I of the Bucharest Oncological Institute “Prof.Dr. Al. Trestioreanu ” 2- Nuclear Medicine Department of the Bucharest Oncological Institute “Prof.Dr. Al. Trestioreanu ” 3-Pathology Department of the Bucharest Oncological Institute “Prof.Dr. Al. Trestioreanu” Purpose: The approach and surgical indication for patients with stage IV cancer are debatable in terms of risk-benefit analysis. Surgery for malignant melanomas in the metastatic stage can be performed in a scheduled or emergency context. Material and method: A retrospective study was performed in the General and Oncological Surgery Clinic I, during 10 years (2012-2021), in which the secondary intra-abdominal determinations were evaluated, starting with a malignant melanoma. Reference was made to cases presented in the emergency or which required surgery due to the nature of the complications developed. Results: The surgeries performed for the indication that imposed them (intestinal necrosis, invagination, haemorrhage, perforation) had a positive impact on the clinical evolution of the respective patients (average overall survival 14 months with a 5-year survival of 20%). Conclusions: Metastasectomy remains the only treatment for malignant melanoma that can provide a complete pathological response and has been associated with favourable survival rates, even in the context of palliative surgery. Figure 1a and 1b. Malignant cutaneous melanoma with different degrees of melanic pigment distribution, evaluated both visually (left) and with the help of the digital dermatoscope (right). Images from the collection of Dr. Alin Nicolescu Figure 2: Secondary determinations from cutaneous melanoma in a mesenteric lymph node: Top left panel: Solid mass of tumor cells without pigment deposition, HE, 50x, Top right panel: strong positive (diffuse) reaction in S - 100 in tumor cells, bottom left panel: diffuse positive reaction to HMB-45, IHC, 100x, bottom right panel: diffuse positive reaction to MART-1 in tumor cells, IHC, 100x Figure No. 3. 64-year-old man with recurrence from a malignant melanoma of the left thigh, two years after the end of treatment; supraclavicular lymph node and right adrenal mass showing high uptake of F18-FDG. 4.a. 4.b. 4.c. 4.d. 4.e. 4.f. Figure no.4. a, b and c: intraoperative appearance of the metastatic tumor of the small intestine (acromic melanoma) causing intestinal invagination and images (4.d, e, f) computed tomography highlighting the intestinal invagination, with a specific "donut-like" appearance