
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ppts of 3rd and 4th stage.ppt
Similar to ppts of 3rd and 4th stage.ppt (20)
More from Sarita591896
More from Sarita591896 (7)
Recently uploaded
Recently uploaded (20)
ppts of 3rd and 4th stage.ppt
- 1. M.M.COLLEGE OF NURSING PRESENTED BY: SIMARJEET KAUR M.Sc. NURSING 1ST YEAR
- 2. INTRODUCTION • Series of events that takes place in the genital organs in an effort to expel the viable products of conception out of the womb through the vagina into the outer world is called labour. It begins after explusion of the fetus and ends with explusion of the placenta and membranes
- 3. THIRD STAGE OF LABOUR • It begins after explusion of the fetus and ends with explusion of the placenta and membranes (after-births). Its average duration is about 15 minutes in both primigravidae and multiparae. The duration is, however, reduced to 5 minutes in active management.
- 4. EVENTS IN THIRD STAGE OF LABOUR placental separation; and finally its. explusion with the membranes its descent to the lower segment
- 5. Placental Separation At the beginning of labour, the placental attachment roughly corresponds to an area of 20 cm in diameter. There is no appreciable diminution of the surface area of the placental attachment during first stage. During the second stage, there is slight but progressive diminution of the area following successive retractions, which attains its peak immediately following the birth of the baby. After the birth of the baby, the uterus measures about 20 cm vertically and 10 cm antero- posteriorly, the shape becomes discoid. The wall of the upper segment is much thickened while the thin and flabby lower segment is thrown into folds. The cavity is much reduced to accommodate only the after- births.
- 6. Mechanism of Separation Marked retraction reduces effectively the surface area at the placental site to about its half . It cannot keep pace with such an extent of diminutio n resulting in its buckling.. A shearing force is instituted between the placenta and the placental site which brings about its ultimate separation The plane of separation runs through deep spongy layer of decidua basalis so that a variable thickness of decidua covers the maternal surface of the separated placenta.
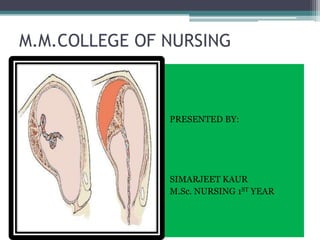
- 7. Two ways of separation of placenta Central Separation (Schultze) Detachment of placenta from its uterine attachment starts at the centre resulting in opening up of few uterine sinuses and accumulation of blood behind the placenta.
- 9. Marginal Separation (Mathews- Duncan): Separation starts at the margin as it is mostly unsupported. With progressive uterine contraction, more and more areas of the placenta get separated. Marginal separation is found more frequently.
- 10. Separation of the Membranes After complete separation of the placenta, it is forced down into the flabby lower uterine segment or upper part of the vagina by effective contraction and retraction of the uterus. Thereafter, it is expelled out by either voluntary contraction of abdominal muscles ( bearing down efforts) or by manipulative procedure.
- 11. MECHANISM OF CONTROL OF BLEEDING • After placental separation, innumerable torn sinuses which have free circulation of blood from uterine and ovarian vessels have to be obliterated. • The occlusion is effected by complete retraction where by the arterioles, as they pass through the interlacing intermediate layer of the myometrium, are literally clamped.
- 12. CONT….. • It is the principal mechanism to prevent bleeding. However, thrombosis occurs to occlude the torn sinuses, a phenomenon which is facilitated by hypercoagulable state of pregnancy • Apposition of the walls of the uterus following explusion of the placenta also contributes to minimise blood loss
- 13. CLINICAL COURSE OF THIRD STAGE OF LABOUR PAINS: For a short time, the patient experiences no pain. Intermittent discomfort in the lower abdomen reappears, corresponding with the uterine contractions. BEFORE SEPARATION: Per abdomen – Uterus becomes discoid in shape, firm in feel and non-ballottable. Fundal height reaches slightly below the umbilicus. Per vagina- There may be slight trickling of blood. Length of the umbilical cord as visible from outside, remains static.
- 14. AFTER SEPARATION It takes about 5 minutes in conventional management for the placenta to separate. • Per abdomen- Uterus becomes globular, firm and ballottable. The fundal height is slightly raised as the separated placenta comes down in the lower segment and the contracted uterus rests on top of it. There may be slight bulging in the suprapubic region due to distension of the lower segment by the separated placenta.
- 15. • Per vagina- There may be slight gush of vaginal bleeding. Permanent lenghthening of the cord is established. This can be elicited by pushing down the fundus when a length of cord comes outside the vulva which remains permanent, even after the pressure is released. Alternatively, on suprapubic pressure upwards by fingers, there is no indrawing of the cord and same lies unchanged outside the vulva.
- 16. EXPLUSION OF PLACENTA AND MEMBRANES The explusion is achieved either by voluntary bearing down efforts or more commonly aided by manipulative procedure. The after-birth delivery is soon followed by slight to moderate bleeding amounting to 100-250 ml.
- 18. MANAGEMENT OF THE THIRD STAGE OF THE LABOUR Principles of the management of third stage are • to ensure strict vigilance and • to follow the management guidelines strictly in practice • to prevent the complications
- 19. STEPS OF MANAGEMENT • Expectant management • Active management
- 20. EXPECTANT MANAGEMENT • Placental separation and descent into the vagina are allowed to occur spontaneously. • Minimal assistance may be given for the placental explusion if it needed • Constant watch is mandatory and the patient should not be left alone • If the mother is delivered in the lateral position, she should be changed to dorsal position to note features of placental separation and to assess the amount of blood loss
- 21. A hand is placed over the Fundus a) to recognise the signs of separation of placenta b) to note the state of uterine activity- contraction and relaxation c) to detect cupping of the fundus which is an early evidence of inversion of the uterus Placenta is separated within minutes following the birth of the baby.
- 23. Explusion of the placenta When the features of placental separation and its descent into the lower segment are confirmed, the patient is asked to bear down simultaneously with the hardening of the uterus. • If the patient fails to expel, one can wait safely upto 10 minutes if there is no bleeding. • As soon as the placenta passes, it is grasped by the hands and twisted round and round with gentle traction so that the membranes are stripped intact
- 24. • If the membranes threaten to tear, they are caught hold of by sponge holding forceps and twisting movements the rest of the membranes are delivered • Gentleness, patience and care are prerequisites for complete delivery of the membranes • If the spontaneous explusion fails or is not practicable, because of delivery under anaesthesia, any one of the following methods can be used to expedite explusion
- 25. ASSISTED EXPLUSION: Controlled cord traction (modified Brandt- Andrews method)- • The palmar surface of the fingers of the left hand is placed above the symphysis pubis approximately at the junction of upper and lower uterine segment. • The body of the uterus is pushed upwards and backwards, towards the umbilicus while by the right hand steady tension is given in downward and backward dirction holding the clamp until the placenta comes outside the introitus.
- 26. FUNDAL PRESSURE • The fundus is pushed downwards and backwards after placing four fingers behind the fundus and the thumb infront using the uterus as a sort of piston. • The pressure must be given only when the uterus becomes hard. If it is not, then make it hard by gentle rubbing. • The pressure is to be withdrawn as soon as the placenta passes through the introitus.
- 27. • If the baby is premature, this method is preferable to cord traction as the tensile strength of the cord is much reduced in both the instances • The uterus is massaged to make it hard, which facilitates explusion of retained clots if any. Injection of oxytocin 5-10 units I.V. or methergin 0.2 mg is given I.M. Oxytocin is more stable and has lesser side effects as compared to ergometrine.
- 28. EXAMINATION OF THE PLACENTA, MEMBRANES AND CORD • The placenta is placed on a tray and is washed out in running tap water to remove the blood and clots. • The maternal surface is first inspected for its completeness and anomalies. • The maternal surface is covered with greyish decidua. Normally the cotyledons are placed in close approximation and any gap indicates a missing cotyledon.
- 29. • The membranes- chorion and amnion are to be examined carefully for completeness. The amnion is shiny but the chorion is shaggy. • The cut end of the cord is inspected for number of blood vessels. There are two umbilical arteries and one umbilical vein. • The absence of cotyledons or evidence of missing membranes demands exploration of the uterus urgently.
- 30. VULVA, VAGINA AND PERINEUM • INSPECTED carefully for injuries and to be required, if any. • The episiotomy wound is now sutured. • The vulva and adjoining part are cleaned with cotton swabs soaked in antiseptic solution. • A sterile pad is placed over the vulva.
- 31. ACTIVE MANAGEMENT OF THIRD STAGE • Principles in active management is to excite powerful uterine contractions following birth of the anterior shoulder by parenteral oxytocin which facilitates not only early separation of placenta but produces effective uterine contractions following its separation.
- 32. Advantages • To minimise blood loss in third stage approximately to 1|5th • To shorten the duration of third stage to half Disadvantages • Increased incidence of retained placenta and increased incidence of manual removal of placenta • Accidental administration during delivery of the first baby in undiagnosed twins produces danger to the unborn second baby caused by asphyxia due to tetanic contraction of the uterus
- 33. PROCEDURE • Inj. Ergometrine o.25mg or methergin 0.2mg is given intravenously following the birth of anterior shoulder. • If administered prior to this, there is chance of imprisonment of the shoulder behind the symphsis pubis. • This is followed by slow delivery of the baby taking atleast 2-3 minutes. • The placenta is expected to be delivered following the delivery of the buttocks.
- 34. • If the placenta is not delivered, it should be delivered forthwith by controlled cord traction technique after clamping the cord while the uterus still remains contracted. • If the first attempt fails, another attempt is made after 2-3 minutes failing which another attempt is made at 10 minutes. If this still fails, manual removal is to be done.
- 35. Limitation To be effective, it should be administered in proper time followed by slow delivery of the baby and followed by rapid delivery of the placenta It should not be used in cardiac cases or severe pre-eclampsia, for fear of precipitating cardiac overload in the aggravation of the blood pressure.
- 36. MANUAL REMOVAL OF THE PLACENTA STEP- I: The operation is done under general anaesthesia. The operation may have to be done under deep sedation with 10 mg diazepam given intravenously. The patient is placed in lithotomy position. With all aseptic measures the bladder is catheterised. STEP-II: One hand is introduced into the uterus after smearing with the antiseptic solution in cone shaped manner following the cord, which is made taut by the other hand.while introducing the hand, the labia are separated by the fingers of the other hand. The fingers of the uterine hand should locate the margin of the placenta. STEP-III: Counter pressure on the uterine fundus is applied by the other hand placed over the abdomen. The abdominal hand should steady the fundus and guide the movements of the fingers inside the uterine cavity till the placenta is completely separated. STEP-IV: As soon as the placental margin is reached, the fingers are insinuated between the placenta and uterine wall with black of the hand in contact with the uterine wall. The placenta is gradually separated with a sideways slicing movement of the fingers, until whole of the placenta is separated.
- 37. STEP-V: When the placenta is completely separated, it is extracted by traction of the cord by the other hand. The uterine hand is still inside the uterus for exploration of the cavity to be sure that nothing is left behind. STEP-VI: Ergometrine 0.25mg is given I.V. and uterine hand is gradually removed while massaging the uterus by the external hand to make it hard. After the completion of manual removal, inspection of the cervico-vaginal canal is to be made to exclude any injury STEP-VII: The placenta and membranes are to be inspected for completeness and be sure that the uterus remains hard and contracted
- 38. NURSING MANAGEMENT OF THE THIRD STAGE OF LABOUR Identification of the third stage Placental separation is indicated by the following, in sequence • A firmly contracting fundus • A change in the uterus from a discoid to a globular shape • A visible and palpable rounded bulge above the symphysis • A sudden gush of dark blood • Apparent lengthening of the umbilical cord • A vaginal fullness noted on vaginal or rectal examination, or fetal membranes seen • After the placenta is explused, it is examined for intactness to be certain that no portion of it remains in the uterine cavity.
- 39. MATERNAL PHYSICAL STATUS • Cardiac output is increased rapidly as maternal circulation to the placenta ceases and the pooled blood from the lower extremities is mobilized • The pulse rate slows to the change in cardiac output. Pulse rates tend to remain slightly slower than before pregnancy during the first 7 to 10 days after delivery. • The nurse observes the mother for signs of an altered level of consciousness or alteration in respirations due to change in rapid cardiovascular changes
- 40. NURSING CARE IN THE DELIVERY AREA • To assist in the delivery of the placenta , the nurse instructs the mother to push as contractions are felt • If an oxytocin medication is ordered, the nurse administers the medication in the dosage and by the route indicated by the physician • When the delivery of the placenta is complete and the episiotomy is sutured, the vulva is gently cleansed with sterile water by the physician • The nurse then performs the following: • Applies a sterile perineal pad • Removes the drapes
- 41. • Repositions the delivery table or bed • Lowers the mother’s legs simultaneously from the stirrups • Assists the woman onto her bed if she is to be transferred from the delivery area to the recovery area • Dresses the woman in a clean gown and covers her with a warmed blanket • Raises the side rails of the bed during the transfer
- 43. DEFINITION It starts with the explusion of placenta and ends one hour later. This stage marks the completion of the tasks associated with the first three stages of labour. The mother may have expressions of relief and accomplishment, intermingled with excitement.
- 44. Activities may include • Evaluation of the uterus • Inspection and evaluation of the cervix and vagina • Inspection and evaluation of the placenta, membranes and umbilical cord • Repair of episiotomy and laceration, if any. • Vital signs and other physiological manifestations are checked and evaluated as indicators of recovery from the stress of labour
- 45. Evaluation of the Uterus • The uterus is normally found in the midline of the abdomen approximately two- third to three- fourth of the way up between the symphysis pubis and umbilicus. • A uterus found above the umbilicus is indicative of blood clots inside, which need to be expressed and expelled. • A uterus found above the umbilicus and to one side, usually the right side indicates full bladder. • A firm uterus is indicative of effective uterine homeostasis.
- 46. Inspection of the Cervix and Upper Vaginal Vault The cervix and upper vaginal vault must be inspected in the presence of any or a combination of the following indications. • The uterus is well contracted but there continues to be a steady trickle or flow of blood from the vagina • The mother was pushing prior to complete dilatation of the cervix • The labour and delivery were rapid and precipitous
- 47. • There was manipulation of the cervix during labour, such as manually pushing back an edematous anterior lip of cervix • Traumatic procedures were necessary such as forceps application • Traumatic second stage of delivery such as prolonged shoulder dystocia or large baby • Following normal, spontaneous, vaginal deliveries, if none of these indications is present, it is not necessary to do a cervical and upper vaginal vault inspection.
- 48. REPAIR • The repair of any laceration or an episiotomy is done after examination of the placenta and membranes. If a uterine exploration for retained placental fragments is necessary, it is done prior to the repair. The uterus is checked again for consistency and repair is begun. • Inspection and evaluation of the placenta, membranes and umbilical cord are done before repairing any lacerations or an episiotomy.
- 49. CONTINUING CARE AND MONITORING • Throughout of the fourth stage of labour the mother’s vital signs, uterus, bladder and lochia are monitored and evaluated. This monitoring is maintained until all are stabilized within normal range.
- 50. The technique of monitoring should be organised and include the following: • Check the Vital signs • Palpation of the fundus of the uterus for contractility • Massage of the fundus in relation to the umbilicus • Inspection of the bladder • Inspection of the perineal pad and change if necessary • Offering food and fluids if allowed and comfort, and safety measures
- 51. VITAL SIGNS • The mother’s blood pressure, pulse and respirations are evaluated every 15 minutes until stable at pre-labour levels. • The temperature is taken at least once during the fourth stage of labour. • The temperature continues to be elevated with normal being less than 20 f increase, or below 100.40 f • In assessing the blood pressure and pulse rate, it must be remembered that, the excitement after delivery may cause an elevation in some mothers.
- 52. PALPATION OF THE FUNDUS • During fourth stage of labour, the uterus continues to contract and relax. • The uterus controls postpartum hemorrhage by contracting and compressing the patent blood vessels at the site where the placenta was implanted.
- 53. • Medications such as ergometrine, methargin, pitocin may have been given to the mother IM OR IV during the delivery of the anterior shoulder or immediately after the placenta is delivered. • It stimulates the uterine contractions. Contractions of the uterus occur when the mother hears her newborn baby’s cry or when she can see or hold the baby.
- 54. The fundus of the uterus is palpated by placing the side of one hand on top of, and slightly cupped above the fundus while other hand is placed suprapubically with the exertion of slight pressure. Ideally, the fundus should lie on the mid – plane of the pelvis at or below the umbilicus.
- 55. MASSAGE OF THE UTERUS AND EXPRESSION OF CLOTS • If the uterus is found boggy on palpation, it is massaged until it contracts and becomes firm. Care must be taken not to over massage or over stimulate the fundus. Over stimulation can result in undue muscle fatigue with subsequent relaxation of the organ and possible haemorrhage.
- 56. • During expression, pressure is applied to the fundus with one hand while equal pressure is applied suprapubically with the other hand until the nurse is sure that clots and free blood held in the uterus is expressed sufficiently. After palpation, massage and expression have been completed, the uterus usually stays firm for a period.
- 57. MEASUREMENT OF THE FUNDUS • A measurement of the height of the fundus is taken after the fundus is expressed, measuring from the top of the fundus to the umbilicus. The fundus of the uterus tends to lie closer to the umbilicus in mother’s who are multiparous than in those who are primiparous.
- 58. Some factors which affect the size, placement and muscular tone of the uterus include • Antepartum hydramnios • Multiple births • Uterine inertia • Amount of urine in the bladder
- 59. INSPECTION OF THE BLADDER • The bladder must be evaluated and emptied if it is full and displacing the uterus. If the bladder is full, a bladder bulge will be evident. It feels and appears as a spongy, fluid filled mass below the uterus and above the symphysis pubis. It is important for the bladder to be emptied, because a full bladder displaces the uterus and decreases its ability to contract properly.
- 60. INSPECTION AND CHANGE OF PERINEAL PAD • keep the area as clean and dry as possible. • Regular change of perineal pad and linens under her buttocks is required in order to keep the lochia from becoming dry and adhering to mother’s body. • wash the perineal area and buttocks with mild soap and water to remove lochia not absorbed by the perineal pad.
- 61. • The lochia during the fourth stage of labour is rubra, neither dark red nor bright red. • The lochia consist of blood from the placental site, shreds of membranes, vernix, lanugo, decidua and meconium. • If the bleeding is more than normal, the midwife must keep a perineal pad count, so that estimation of blood loss is more accurate. • Notations must be made in the mother’s chart of how many pads were used, the degree of saturation of each pad, the size and character of clots and the colour of lochia.
- 62. FLUIDS AND FOOD • She should be encouraged to take water, juices and tea or coffee with sugar. • After her condition has stabilized within the limits of normal, which will usually be by the end of the first hour postpartum, she may also eat solid foods. • Mothers must be encouraged to eat a small amount first and to eat slowly. Comfort measures should be supplied and include warm blankets, gown and warm fluids by mouth if not contraindicated.
- 63. NURSING MANAGEMENT ASSESSMENT • Physical assessment • Blood pressure returns to pre-labour state • Pulse is slightly lower than in labour • Fundus remains contracted in the midline and is located 1-2 fingerbreadths below the umbilicus • Lochia is scant to moderate • Bladder is non-palpable • Perineum is intact
- 64. • Psychosocial assessment • Assess the mother’s emotional state. May vary from exhaustion to euphoria • Some mothers may want to interact with their baby, and others may wish to rest at this time.
- 65. NURSING DIAGNOSIS • Pain • Anxiety • Imbalance nutritional pattern • Disturbed sleeping pattern • Risk for altered homeostasis
- 66. PLANNING • Frequent assessments to monitor maternal recovery from delivery • Complete maternal assessment every 15 minutes for the first hour, every 30 minutes for the second hour and then hourly for the next 2 hours • Enhance maternal newborn attachment • Teach self care measures to prevent bleeding and enhance comfort
- 67. • Provide warm blankets and hot drinks for preventing shivering and chilling • Provide clean linen • Offer sponge bath • Place ice packs on perineum to decrease swelling and increase comfort • Massage and express the fundus
- 68. Summary Third stage of labour starts after the explusion of fetus and ends with the explusion of the placenta with its membranes. Today we discussed about the definition, its events, clinical course and management of third and fourth stage of labour.
- 69. CONCLUSION: Atlast, I conclude my topic, third and fourth stage of labour are the crucial stage of labour. In these stages we prevent the patient from postpartum complications. Prevent the client from infection and also educate the client regarding diet and its management.