Design and Development of Low Cost 3D Printed Ambidextrous Robotic Hand Drive...
Sally Poster Final
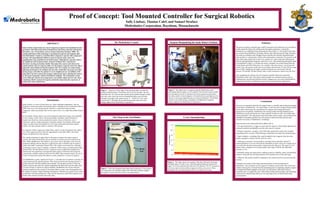
1. Proof of Concept: Tool Mounted Controller for Surgical Robotics
Sally Lindsay, Thomas Calef, and Samuel Straface
Medrobotics Corporation, Raynham, Massachusetts
ABSTRACT
Snake robotic surgical tools can convert dangerous surgeries into minimally invasive
operations with reduced duration of hospital stay, blood loss, muscular and skeletal
discomfort, rate of transfusion, and use of pain medication (Kushner 2009). The
commercialization of this technology is promising for patients and hospitals alike.
The Medrobotics Console is a tool that allows surgeons to operate with a single port
incision with unparalleled flexibility in maneuvering the snake robot, 10x
magnification zoom, and filtered out hand tremors. Although the experience allows
for significant control and precision, surgeons’ feedback have requested an
alternative steering mechanism. Rather than adjust the camera and robot at one
console and the tools at a separate table over the patient, surgeons want to be able to
adjust the robot without leaving the patient’s side. The creation of a camera/snake
adjusting mechanism to be clamped onto the tools would allow for greater precision
during surgery and allow the patient to receive heightened care. In addition, if the
clasp allows for more control, the surgeon could operate faster, allowing the robot to
be used more frequently, which is beneficial to hospitals. The mechanism created
works efficiently and has been integrated to successfully adjust and steer the robot,
complying with the requests of surgeons and further improving the experience of
using snake robot surgical tools.
Introduction
Snake robotics is a class of robots known as ‘hyper-redundant manipulators’ that are
designed to reach inaccessible and cluttered spaces with high levels of articulation (Brown
2006). Sine waves moving through the robot have a spatial and temporal (time)
component, which successfully allow for the robot to move in a snake-like method (Lipkin
2007).
For the patient, robotic surgery can convert dangerous open-heart surgery into minimally
invasive surgery, which comes with myriad benefits including: reduced duration of
hospital stay, blood loss, muscle-skeletal discomfort, chance of infection, rate of
transfusion, and use of pain medication. Generally, patients who undergo robotic heart
surgery are able to leave the hospital two to five days earlier than open-heart surgery
patients, and these patients return to normalcy 50% quicker.
For surgeons, robotic surgery gives them better control over the instruments and a better
view of the surgical site due to the 10x magnification zoom (Woo 2004). Also, hand
tremors are filtered out by the software.
The commercialization of snake robots in the medical industry has lead to surgical
consoles that utilize the flexibility and accessibility to produce powerful surgical assets
(Woo 2004). MedRobotic’s Flex Robot is one console whose flexibility comes from 30
mechanical linkages that are placed in a rigid (frozen state) or flexible state to employ a
“follow-the-leader” mechanism (Neuzil 2012). The catheter can be fitted for a fiberoptic
visualization system, suction, mapping, or ablation without losing its predetermined shape
(Neuzil 2012). The Flex Robot can use a single port access (rather than multiple ports
under the Da Vinci platform) to navigate the entire surface of the heart and accepts any
commercially available catheter-based tools (Ota 2009). Most surgeries require the use of
at least two hand tools and the Flex Robot is easily outfitted for a variety of surgeries.
The MedRobotics system, displayed in Figure 1, is divided into two portions currently: the
visual console and the operation portion. The visual console has the steering joystick to
position the robot with the installed camera aboard. The operation portion is where the
patient is laid out and where the surgeon manipulates the hand tools once the snake robot
is in place (Figure 2). Based on surgeon feedback, MedRobotics has tried to bring the
steering component of the console to the patient table to create a more fluid approach for
the surgeon to operate without breaking concentration. Therefore, my project was to create
an alternative steering mechanism to clasp onto the hand tools, rather than using the more
distant video console to position the snake robot.
Surgeon Manipulating the Snake Robot’s Position
Figure 2. This figure shows a surgeon using the Medrobotics robot
performing a throat surgery on a live patient. Note he must remove a hand
from the patient in order to reposition the robot using the joystick below
the video console. In most surgeries, two hand tools are used (shown in the
insert), so removing a hand becomes even more troublesome. This fluidity
concern is one of the primary complaints in feedback from surgeons.
(Figure adapted from Medrobotics Corporation.)
X Axis Threshold Data
Figure 4. This figure shows an example of the data collected to determine
threshold values. For the X axis, when the analog outputs are between the
range 179-218 (in red) the robot will move left; between 732-757 (in green) it
will move right; in-between those ranges (in yellow), stay at rest. These
thresholds were also determined for the Y-axis and the two Z-axes.
The Clasp on the Tool Holder
Figure 3. This is the designed clasp fitted onto the hand tool. The joysticks
are connected to the interface and the mini USB cable sends the outputs
through the console and to the robot to command motion.
Summary
The goal in creating a controller that would be mounted on the hand tool was to be able to
quickly attach the clasp to the shifting tools throughout operations. A pistol-like
mechanism was established when designing the clasp (Figure 3). The model for the clasp
was created using SolidWorks 3D design software and realized using the Objet 3D printer.
The clasp was outfitted with a Phidgets Sensor Interface Kit and three Sparkfun thumb-
slide joysticks to communicate with the robot and translate commands. The joystick on the
back of the clasp controls the X and Y axis, and the two on the clasp sides (allowing for
both left and right-handed surgeons) control the Z axis. After determining threshold values,
as exemplified in Figure 4, to dictate movement, a program was created using Microsoft
Visual Studios and QNX Momentics. For example, when the joystick is moved upwards
on the Y-axis, the joystick would read out an analog value between 215 and 244 (in a range
from 0-1024), identifying the toggle’s position along the axis, downwards will fall
between 759 and 808. All other analog values would command no motion from the robot.
After integrating the software, the tool mounted controller effectively steered the
Medrobotics snake robot. The clasp worked promptly for combined motions (such as
simultaneously inwards and leftwards motions, engaging two axes) and could feasibly be
integrated in the future of Medrobotics with some commercialization adjustments.
Conclusions
This new tool mounted control for the surgical robot is a feasible and exciting development
for the future of Medrobotics. The clasp (Figure 3) with the newly designed steering ability
for the robot will increase the concentration for surgeons and consequently lead to
improved care for patients. Furthermore, the current joystick steering mechanism cost
$20,000 per console sold but the new clasp controller would cost only a few dollars after
commercialization. The reduced price-tag would make robotic surgery more practical and
affordable for hospitals and allow for more people to benefit from the precision and
minimal invasiveness of Medrobotics’ technology.
Improvements on the clasp could still be added, such as:
• Driving mode function: a trigger to ensure that the surgeon is intentionally adjusting the
robot and would not accidentally move the robot once it is in place.
• Wireless connection: currently, a mini USB cable connects the clasp to the computer.
Using Bluetooth or wireless USB technology would help to de-clutter the operating space.
• Haptic feedback: a rumbling effect could be added to alert surgeons when the robot
brushes up against a surface, like the wall of a vessel.
• Calibration of joysticks: the threshold to command motion should be uniform if
commercialization is to occur. Presently the thresholds are quite varied, for example, the Z-
axis on the left side had a much greater variance from the other axis. The range was 331
analog values, compared to an average analog value range of 586 for the other three
joysticks (±7.55).
• Reliability testing: the clasp needs to undergo extensive reliability, safety, and feasibility
testing to ensure that the steering mechanism will stand the tests of time and usage.
• Efficiency: the joystick should be compared to the current joystick to test precision and
accuracy.
Ultimately, the creation of the clasp represents promise for the development of
Medrobotics. This tool allows for the surgeon to maintain control of the robot at all times
without removing her or himself from the demanding task of completing complex surgeries
by keeping both hands engaged on the tools, over the patient, rather than having to
constantly move to readjust the robot. With further testing and developing, this technology
could easily be implemented effectively into operating rooms worldwide and benefit
myriad patients.
The Medrobotics Console
Figure 1. ‘Section A’ of this figure is the operating table on which the
patient would be laid out. The robotic arm is set over the table. The area
identified with ‘B’ is the arm that extends into the patient through a single
port and is also where the tools are threaded through as seen from the
alternative tip angle of the snake at point ‘C.’ ‘Section D’ is the video
console and ‘E’ identifies the joystick that presently steers the robot.
(Image adapted from Medrobotics Corporation.)
A
D
E
B
Interface
Joysticks
Designed
Clasp
Hand
Tool
C