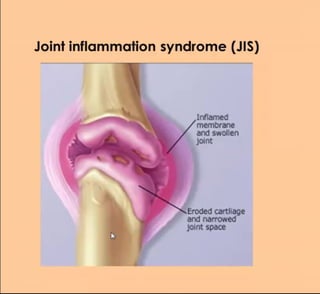
1. Joint inflammation syndrome (JIS)
Inflamed
membrane
and swollen
joint
Eroded cartliage
and narrowed
joint space
2. History
Complaints
Joint pain
The additional information. Arthralgia is joint pain with no abnormal examination
findings. The concept ofarthritis includes other pathological signs.
If the patient complains of a joint pain, ask him to specify a place where
he feels the joint pains. Let him to tell about character and intensity of
pains, about precipitating and relieving factors.
The character and intensity of a joint pain depend on both the
expression of the inflammation and the nature of disorder.
Dull or sharp joint pains, which worsen after rest,
and are relived by movements (rest pains), are
typical for JIS. Joint pains are most marked in the
early morning and after inactivity.
2
1.
If there is the joint damage the usage pain may be
present too.
The patient can note the occurrence of the swelling of the joint or its deformity;
the deviation of the fingers.
Also the patient frequently mentions presence of limitation of the function of
joints.
3. Non-specific symptoms of systemic llness
(reflecting acute phase response)
Fever
Sweats and chills, particularly at night
Weight loss,
t reduction in appetite
Fatigability, poor concentration
4. History of Present illness
1.Speed of onset. For example, crystal synovitis develops very rapidly, often
reaching maximum severity with extreme pain within just 2-12 hours, whereas sepsis
is more sub acute and continues to progress until treated.
Many inflammatory joint disorders have chronic beginning.
2.The previous infections or other provoking factors (a trauma, stress, labor,
overcooling, sunlight, the use of alcohol or intake a fat food, starvation, etc.).
3.Clinical course. The chronic inflammatory joint disorders are usually life-long, with
intermittent exacerbations and remissions.
Some patients have mild disease; in others it is more severe.
Some diseases have progressive character. Each exacerbation of disease involves
new joins while in the affected joints the pathologic process continues. At other
diseases the localization of a joint inflammation varies.
4.Previous investigations and treatment; them results
Life history
[past medical history; current health status; family history: psychosocial history]
Environmental hazards, at home, school, and workplace;
the occurrence of Inflammatory joint disorders in members of their family;
allergies.
5. Physical Examination
Inspection of gait
Antalgic gait. Jerky asymmetric gaitwith less time
weight-bearing on painfulleg.
Ifthe patient feels acute pain in the
metotarsophalangeal joints he can support on the heel
only.
Attitude of the extremities
(held in "loose-pack" position)
Inspection of involved joints at rest
The character and intensity of
joint disorders are correlated
with the amount of inflammatory
activityand nature of disease.
Redness of the overlyingskin
Swelling due to the synovitis,
effusion
6. Deformityofjoint.It is the
permanent change of the joint
shape due to:
Boutonniere deformity
1. the proliferativeor sclerotic
process in ether synovial
membrane or soft tissue,
2.new bone formation,
3.the bone destruction,
Swan neck deformity
4.the fibrous or bony ankylosis,
5.damages of the periarticular
structures,
6.subluxations.
Deviations of fingers. These are deviations of
axes of jointed bones from normal position.
For example, the patients with Rheumatoid
arthritis have the deviation ofaxes of all fingers
in one direction (ulnardeviation of fingers)
7. There are the deviations of fingers
axes in different directions in the
patients with Psoriasis arthropathy
or Gout.
Palpation of involved joints at rest
Increased warmth (e.g. synovitis)
Tenderness (Overjoint line)
-Swelling: fluid (fiuctuant), Soft tissue (soft, non-fluctuant)
8. If you suspect a small amount offluid in the knee jointlook for a Bulge
Sine
1.With the ball of your handmilkthemedial aspect of the knee firmly
upward two or three times to displace any fluid.
2. Then press or tap the knee just behind the lateral margin of the patella.
3. Watch for a bulge of returning fluid in the hollowmedial to the patella.
9. Try to Ballotte a "Floating Patella." Firmly grasp the thighjust above the
knee with one hand, thus forcing fluid out of the superior portion of the
jointspace between the patella and femur. With the fingers of your other
hand, push the patella sharply against the femur. Feel for a palpable tap.
Mecto HagaanwBawR
Ha HAQKoneHHIK Mecto, pe ouyujaeTca
nepetexa-ne xopHOCTH
It is useful when large amounts of fluid are present.
10. Inspection during movement
In the beginning check the range of active movements of joints. In the
pathology:
Functional restriction (Affected most or
allactivemovements)
HeiTpanbHoenonaweHwe
Paarvóane
YnbHapHOe lyveaoe
OTBeeHne OTBeNeHMe
HetpanbHo
nonoxeHwe
OICTM KOICTM
Cr6awe
Stress pain =
increasing pain towardsextremes of
movement. Universalstress
pain (inmost/all directions - synovitis). Pain worsens as the joint moves
towards the "tight-pack" positionsbecauseofincreased intracapsularoressure
from inflammatory and effusion. In the mid "loose-pack" position, when the
capsule is at its slackest, there is no pain.
Then compare ranges of active and passive movements in joints.
Active and passive movement afected equally
11. The additional information. Monoarthritis is situation when one joint is involved.
Acute monoarthritis should always to consideration of sepsis and crystals.
Monoarthritis can be the presentation of what subsequently evolves into oligo-or
polyarthtritis, and atypical presentation of common disease is more prevalent than
rare disease.
Oligoarthritis is arthritis affecting two, three or four joints orjoint groups (for
example, the wrist or midfoot, which have many joint but are counted as a single
site). Polyarthritis is involvement of five or more joints or joint group. In
determining the cause it is helpful to considerwhether the polyarthritis:
is symmetrical or asymmetrical
shows predominant or equal involvement for upper and lower limbs
shows predominant or equal involvement for large and small joints
A Rheumatoid arthrits J iniamnmatorys00a
12. Investigations
Lab tests
The full blood count (anaemia, leukocytosiss or leukopenia)
Increased ESR
C-reactive protein (CRP)> 6 mg/L;
Serum proteins (12-globulin>10,5%; T-globulin>19%);
Rheumatoid factor is an antibody directed against a specific region of the Fc
fragment of human lgG. One traditional method of detecting IgM rheumatoid factor is
to coat latex beads with human IgG ("latex fixation test"). Pathological titer is higher
than 1:24. High titer of serum RF is typical for RA, but it is not feature of seronegative
spondarthritis.
.Serum uric acid (in male with gout >0,42 mmol/L; in female with gout >0,36 mmol/L)
and urine uric acid (in gout >3,8 mmol/24hr)
Immunological test for antibodies to Brucella; chlamydia; Antistreptolysin O (ASLO);
mycobactera tuberculesis
Tuberculinskintest;Spectrolux (porfirins);
Bacterial swabs from genitaliaformicroscopy;
Synovial fluid analysis. This is the pivotalinvestigationto confim the diagrnosis of
septic arthritis, crystal-associated arthritis and intra-articular bleeding. With
increasing joint inflammation the volume of synovial fluid (SF) increases, the total cell
count and proportion of neutrophils rise (causing turbidity), and viscosity lowers (due
to proteas degradation of hyaluronate). If you see the
frank pus or "pyarthrosis" (very high neutrophil count),
SF should be sentfor urgent Gram stain and culture.
PCR (real-time) for chlamydia, mycoplasma, and ureaplasma
16. CT. Computerized reconstruction of multiple radiographic scan
sections gives detailed information on anatomy, especially of bone,
allowing three-dimensional visualization of joints.
17. Scintigraphy. This readily
available technique involves
gamma-camera imaging
following an intravenous
injection of radioisotope,
usually 99mTc-
bisphosphonate. Early post
injection images reflect
vascularity and can show, for
example, the increased
perfusion of inflamed
synovium.